a1f9bd04cf18cdec6d60a9c1661461dd.ppt
- Количество слайдов: 44



Feeding the Obese Critically Ill Daren K. Heyland Professor of Medicine Queen’s University, Kingston General Hospital Kingston, ON Canada

Objective

Key Points • Not all obese patients are the same • Nutritional approach may need to vary • Challenge to the prevailing dogma that hypocaloric feeding (undernourishment) is acceptable

Obesity Trends* Among U. S. Adults BRFSS, 1990, 2000, 2010 (*BMI 30, or about 30 lbs. overweight for 5’ 4” person) 2000 1990 2010 No Data 29% <10% ≥ 30% 10%– 14% 15%– 19% 20%– 24% 25%–

Relative Trends Sturm, Pub Health, 2007, 121: 492

What to do when the obese patient becomes critically ill?
 Canadians • Insufficient evidence Americans • Provide 50")
Feeding the Obese Critically Ill (BMI>30) Canadians • Insufficient evidence Americans • Provide 50 -70% of target energy requirements (>14 kcal/kg actual body weight) and >2. 0 -2. 5 g/kg IBW/d protein)* Europeans • (silent) *Choban JPEN 2013
 • 16 hospitalized obese patients requiring PN")
RCTs of Hypocaloric Nutrition in Obesity (1) • 16 hospitalized obese patients requiring PN ICU, ‘mild-moderate stress’) • Defined obesity as >130% IBW • Goal was to show equal nitrogen balance in hypocaloric group (14 kcals/kg actual wt) vs control (25 kcals/kg actual wt) • Protein intake was the same (2. 0 g/kg IBW) • Outcomes: – – (? No difference in % of patients achieving positive Nitrogen Balance Weight change did not differ significantly between groups Infections not measured No difference in LOS or mortality Burge JPEN 1994
 • • • 30 hospitalized obese patients")
RCTs of Hypocaloric Nutrition in Obesity (2) • • • 30 hospitalized obese patients (13 in the ICU) Defined obesity as BMI >35 Hypocaloric group -13. 6 kcals/kg actual wt Control group – 22. 5 kcals/kg actual wt Protein intake was the same (2 g/kg IBW) Outcomes: – – No difference in % of patients achieving positive Nitrogen Balance Weight change did not differ significantly between groups Infections not measured No difference in LOS or mortality Choban et al, Am J Clin Nutr. 1997 Sep; 66(3)
 • Focus was on")
Clinical Inferences to ICU Patients? • N=46 (13 ICU patients) • Focus was on patients requiring PN, says nothing about patients on EN • Focus was on NB, other outcomes not assessed or underpowered.

Is there sufficient evidence that should inform one prescription on how ALL obese patients should be fed?

Extreme Obesity and Outcomes in Critically Ill Patients Analysis of data from multicenter international observational study of ICU nutrition practices in 2007 and 2008 Increased obesity= increased risk of prolongation of stay Martino Chest 2011; 140: 1198

Not all critically ill obese patients are the same: the influence of prior co-morbidities. Prospective observational study of 183 critically ill patients had a BMI ≥ 30 Raham ISRN Obesity 2012

Not all critically ill obese patients are the same: the influence of prior co-morbidities. 0 -1 co-morbidity (n=38) Discharged alive from ICU by day 28 2 or more comorbidities p values (n=145) 36 (94. 7%) 112 (77. 2%) 0. 02 Maximum SOFA score 7. 5[5. 0 to 11. 0] 9. 0[6. 0 to 13. 0] 0. 04 Delta SOFA score 1. 5[0. 0 to 3. 0] 2. 0[1. 0 to 5. 0] 0. 07 Number of days on MV 2. 0[1. 0 to 5. 0] 4. 0[2. 0 to 7. 0] 0. 09 Number of days in ICU 3. 0[3. 0 to 11. 0] 6. 0[3. 0 to 10. 0] 0. 04 24. 5[17. 0 to 25. 0] 20. 0[3. 0 to 24. 0] 0. 003 Mortality at Day 14 2 (5. 3%) 24 (16. 6%) 0. 08 Mortality at Day 28 2 (5. 3%) 30 (20. 7%) 0. 03 ICU free days in the first 28 days Raham ISRN Obesity 2012

Not all critically ill obese patients are the same: the influence of prior co-morbidities. In the adjusted analysis, compared to patients with limited co-morbidities, obese patients with multiple comorbidities were: • more likely to die at 28 days (OR 4. 28, 95%CI, CI 0. 92, 20. 02, p=0. 06) • tended to have longer ICU duration (3. 06 days, standard error [SE] 2. 28, p=0. 18) and • had significantly fewer ICU free days in the first 28 days (-3. 92 days, SE 1. 83, p=0. 03). Raham ISRN Obesity 2012

ICU Obese patients are not all created equal…should we expect the impact of nutrition therapy to be the same across all patients?

Start EN within 24 -48 hrs of admission to ICU Optimal Amount of Protein and Calories for Critically Ill Patients

Bias and accuracy of common estimation methods for resting metabolic rate in mechanically ventilated critically ill patients Penn State or modified Penn State if >60 recommended by experts* Curr Opin Crit Care 2012, 18: 174– 177 *Choban JPEN 2013

Increasing Calorie Debt Associated with worse Outcomes Caloric Debt Adequacy of EN § Caloric debt associated with: § Longer ICU stay § Days on mechanical ventilation § Complications § Mortality Rubinson CCM 2004; Villet Clin Nutr 2005; Dvir Clin Nutr 2006; Petros Clin Nutr 2006

• Point prevalence survey of nutrition practices in ICU’s around the world conducted Jan. 27, 2007 • Enrolled 2772 patients from 158 ICU’s over 5 continents • Included ventilated adult patients who remained in ICU >72 hours

How are Obese Patients Actually Being Fed? Total 25 -<30 30 -<35 35<-40 >=40 P-value 24. 0 (5. 8) 23. 8 (3. 7) 20. 2 (3. 4) 17. 9 (2. 8) 15. 0 (4. 0) <0. 0001 1. 2 (0. 3) 1. 0 (0. 2) 0. 9 (0. 2) 0. 8 (0. 3) <0. 0001 14. 0 (7. 6) 13. 6 (6. 7) 11. 2 (5. 9) 9. 8 (5. 1) 8. 1 (4. 4) <0. 0001 0. 6 (0. 4) 0. 6 (0. 3) 0. 5 (0. 3) 0. 4 (0. 3) <0. 0001 173 (6. 2%) 50 (6. 1%) 28 (7. 1%) 17 (10. 5%) 22 (12. 9%) 0. 0002 Nutritional Prescription Mean Energy [Kcal/kg/day] (SD) Mean Protein [grams/kg/day] (SD) Nutrition Received Mean Energy [Kcal/kg/day] (SD) Mean Protein [grams/kg/day] (SD) Received EN protein supplements

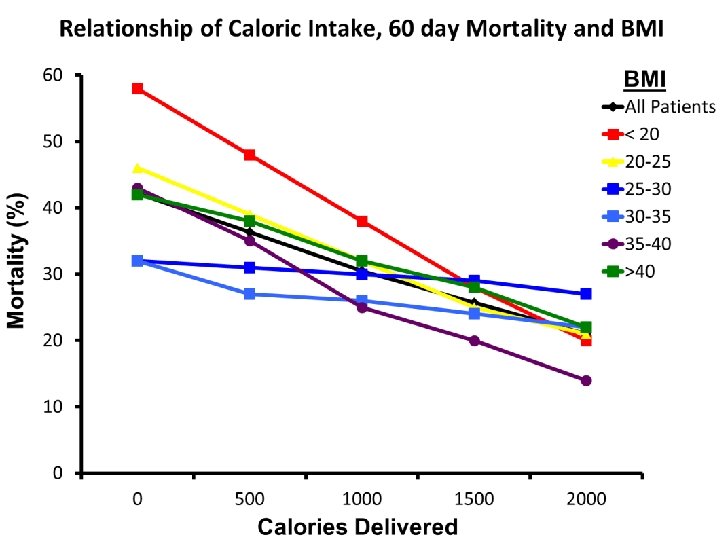
Hypothesis • There is a relationship between amount of energy and protein received and clinical outcomes (mortality and # of days on ventilator) • The relationship is influenced by nutritional risk • BMI is used to define chronic nutritional risk

What Study Patients Actually Rec’d • Average Calories in all groups: – 1034 kcals and 47 gm of protein Result: • Average caloric deficit in Lean Pts: – 7500 kcal/10 days • Average caloric deficit in Severely Obese: – 12000 kcal/10 days

Relationship Between Increased Energy and Ventilator-Free days Adjusted BMI Group 95% CI P-value Estimate LCL UCL Overall 3. 5 1. 2 5. 9 0. 003 <20 2. 8 -2. 9 8. 5 0. 337 20 -<25 4. 7 1. 5 7. 8 0. 004 25 -<30 0. 1 -3. 0 3. 2 0. 958 30 -<35 -1. 5 -5. 8 2. 9 0. 508 35 -<40 8. 7 2. 0 15. 3 0. 011 >=40 6. 4 -0. 1 12. 8 0. 053 Legend: # of VFD per 1000 kcals received per day adjusting for nutrition days, BMI, age, admission category, admission diagnosis and APACHE II score.
 is Better! If you feed them (better!) They will leave (sooner!)")
More (and Earlier) is Better! If you feed them (better!) They will leave (sooner!)

ICU Obese patients are not all created equal…should we expect the impact of nutrition therapy to be the same across all patients?

Muscle Matters! Skeletal muscle mass predicts ventilator-free days, ICUfree days, and mortality in elderly ICU patients • Patients > 65 years with an admission abdominal computed tomography scan and requiring intensive care unit stay at a Level I trauma center in 2009 -2010 were reviewed. • Muscle cross-sectional area at the 3 rd lumbar vertebra was calculated and sarcopenia identified using sex-specific cutpoints. • Muscle cross-sectional area was then related to clinical parameters including ventilator-free days, ICU-free days, and mortality. Moisey Crit Care 2013 Sept; 17(5): R 206

Body Composition Lab CT Imaging Analysis Skeletal Muscle Adipose Tissue

Physical Characteristics of Patients • • • N=149 patients Median age: 79 years old 57% males ISS: 19 Prevalence of sarcopenia: 71%
 Non-sarcopenic Patients (n=43) 25. 8 (22. 7,")
BMI Characteristics All Patients Sarcopenic Patients (n=106) Non-sarcopenic Patients (n=43) 25. 8 (22. 7, 28. 2) 24. 4 (21. 7, 27. 3) 27. 6 (25. 5, 30. 4) Underweight, % 7 9 2 Normal Weight, % 37 44 19 Overweight, % 42 38 51 Obese, % 15 9 28 BMI (kg/m 2) Almost half the sarcopenic patients were overweight

Low muscle mass associated with mortality Proportion of Deceased Patients Sarcopenic patients 32% Non-sarcopenic patients 14% P-value 0. 018

Muscle mass is associated with ventilator-free and ICU-free days All Patients Sarcopenic Patients Non. Sarcopenic Patients P-value Ventilator-free days 25 (0, 28) 19 (0, 28) 27 (18, 28) 0. 004 ICU-free days 19 (0, 25) 16 (0, 24) 23 (14, 27) 0. 002

What does Nutrition Risk Assessment look like for the obese critically ill? Acute Starvation (Reduced po intake, pre ICU hospital stay) Degree of Obesity (BMI) Functional Impairment (reduced mobility and strength) Chronic Malnutrition (? Sarcopenia) Nutrition Status micronutrient levels - immune markers - muscle mass Pre-existing Comorbidities (Metabolic consequences) Severity of Illness (APACHE, SOFA, IL-6) Risk Status High risk= high risk of death and greater likelihood of benefit from Nutrition
 Increasing aggressiveness Increasing complications We")
A Proposed Clinical Staging System for Obesity (non-critically ill) Increasing aggressiveness Increasing complications We need to adapt this way of thinking to the ICU setting! Sharma Int J of Obesity 2009; 33: 289

Role of PN in the Obese Patient? What if you can’t provide adequate nutrition enterally? … to add PN or not to add PN, that is the question!

Early vs. Late Parenteral Nutrition in Critically ill Adults • 4620 critically ill patients • Results: • Randomized to early PN Late PN associated with – Rec’d 20% glucose 20 • 6. 3% likelihood of early ml/hr then PN on day 3 discharge alive from ICU and hospital • OR late PN • Shorter ICU length of – D 5 W IV then PN on day stay (3 vs 4 days) 8 • Fewer infections (22. 8 vs • All patients standard EN plus 26. 2 %) ‘tight’ glycemic control • No mortality difference Cesaer NEJM 2011

Early vs. Late Parenteral Nutrition in Critically ill Adults • ? Applicability of data – No one give so much IV glucose in first few days – No one practice tight glycemic control • Right patient population? – – Majority (90%) surgical patients (mostly cardiac-60%) Short stay in ICU (3 -4 days) Low mortality (8% ICU, 11% hospital) >70% normal to slightly overweight • Not an indictment of PN – Early group only rec’d PN for 1 -2 days on average – Late group –only ¼ rec’d any PN Cesaer NEJM 2011

Lancet Dec 2012 Doig, ANZICS, JAMA May 2013

What if you can’t provide adequate nutrition enterally to critically ill obese patient? ? … to supplement with PN or not to PN, that is the question! Case by Case Decision Maximize EN delivery prior to initiating PN

The TOP UP Trial PN for 7 days High-risk ICU patients BMI <25 BMI >35 R Inadequately fed enterally in first 2 days (<60%) Stratified by: Site BMI Med vs Surg EN Alone Primary Outcome 60 -day mortality
")
HYPOTHESIS Increased early energy and protein delivery with PN+EN to underweight (BMI < 25) and obese (BMI> 35) critically ill patients will result in improved survival at 60 day versus standard EN alone

Key Methodological Features • Only enrolling nutrition ‘at risk’ patients not tolerating EN within first 48 hrs. • Paired EN/PN feeding to meet goal rate of protein/calories from initiation vs. EN alone x 7 days • High nitrogen PN solution with olive oil (Olimel, 3 in 1, Baxter) • Comprehensive assessment of muscle mass and muscle function

In Conclusion • Not all Obese ICU patients are the same in terms of ‘risk’- need to develop and validate risk assessment tools in this population • Iatrogenic underfeeding is harmful to some Obese ICU patients or some will benefit more from aggressive feeding (avoiding protein/calorie debt) • Aggressive use of EN (high protein diets) and protein supplements indicated • Supplemental PN may be beneficial in some
a1f9bd04cf18cdec6d60a9c1661461dd.ppt