86fdd061d6c9cf326719d7f47cda3f44.ppt
- Количество слайдов: 48



Excreta and Household Wastewaters - Introduction Global Water, Sanitation and Hygiene ENVR 890 -2 Mark D. Sobsey February, 2009

Household Human Wastes and Wastewaters

Feces - Composition Note: This number may be too low; live bacteria are shed in large quantity

Feces, Microbes and Microbial Pathogens Besides nutrients and organic matter, human and animal fecal wastes contain large numbers of microbes (>100 billion/gram). v Constitute ~1/3 rd the mass of human fecal matter v Most are beneficial or essential in the gut; they are NOT pathogens v Some gut microbes ARE human pathogens; can cause disease – Humans and animals harbor pathogens some of the time – Pathogen colonization and infection is common – In some food animals (poultry, beef and swine) – In people with poor sanitation and hygiene – Esp. in developing world; carriage rates are high – Human pathogens are typically shed in human and animal feces

Excreta and Graywater– Definitions and Properties Excreta: Human feces and urine Managed in different ways: Direct disposal on land or in water Direct use as fertilizer, soil conditioner and for aquaculture Pre-treatment prior to use Dilution with water to convey (sewage) for disposal or use Direct use of untreated (raw) sewage Treatment and discharge to land or water Treatment and reuse (agriculture, aquaculture, horticulture, industrial and civil use Graywater: Other wastewater from human activity Not directly from human fecs and urine Wastewater from washing, bathing, etc

Managing Human Excreta - Options • “Dry” Collection: – Open defecation – Collect in a container • e. g. , chamber pot – Discharge to the environment w/ or w/o Rx • Latrines – several kinds – Treat or dispose of or both – Separate feces and urine; • Then, treat/store, use, dispose to the environment
 • Use some water •")
Managing Human Excreta - Options • Semi-wet (or semidry) • Use some water • Pour-flush toilets and other low water use systems NO! Hanging Toilet/Latrine

Managing Human Excreta - Options • Wet Systems Septic tank - soil absorption system – On-site Septic Systems – Other On-site systems • Soak pits – Sewerage – Sewage treatment systems

Human Excreta – Resource or Risk? • Human excreta as a potential resource • Contains nutrients (N, P, K, and organic matter) • Nutrients and organic matter are: • Detrimental in water, esp. surface water • Eutrophication, anoxia, fish kills • Beneficial on land • Fertilizer, soil conditioner, land stabilizer • Widely used as a fertilizer and soil amendment in both developed and developing countries Nitrogen (N) 4. 5 Phosphorous 0. 6 (P) Potassium Organic matter Annual (as BOD) 1. 0 35 Amounts/Person, Kg

Nutrient Content of Human Excreta • Rich source of inorganic plant nutrients: N, P K and organic matter • Daily human excretion: ~30 g of C (90 g of organic matter), ~ 10 -12 g N, ~ 2 g of P and 3 g of K. • Most organic matter in feces most N and P (70 -80 %) in urine. K equally distributed between urine and feces.

Composition of Household Waste and Wastewater 14. 1 12. 3 5. 3 3. 6 K Organics kg COD/ (Person·year) 0. 8 N 1. 0 Nutrient content kg N, P, K / (Person·year) 500 l 50 l Volume greywater urine faeces Liter / (Person·year) source: Otterpohl 10. 000 – 200. 000 l P

Characteristics of Human Wastes fraction 1. feces 2. urine 3. greywater characteristic • hygienically critical (high risk) • consists of organics, nutrients and trace elements • improves soil quality and increase its water retention capacity • less hygienically critical (less risk) • contains the largest proportion of nutrients available to plants • may contain hormones or medical • residues of no major (or less) hygienic concern/risk • volumetrically the largest portion of wastewater • contains almost no (or less) nutrients (simpler treatment)

source: Drangert, 1998 Fertilizer Potential of Human Excreta
 faeces (brownwater) hygienisation")
Options for Excreta and Greywater Utilization substances treatment utilisation urine (yellowwater) faeces (brownwater) hygienisation by storage or drying anaerobic digestion, drying, composting liquid or dry fertiliser biogas, soil improvement greywater (shower, washing, etc. ) constructed wetlands, gardening, wastewater ponds, biol. treatment, membranetechnology irrigation, groundwaterrecharge or direct reuse

Primary Treatment or Primary Sedimentation Settle solids for 2‑ 3 hours in a static, unmixed tank or basin. • ~75 -90% of particles and 50 -75% of organics settle out as “primary sludge” – enteric microbe levels in 1 o sludge are sometimes ~10 X higher than in raw sewage • enriched by solids accumulation • Overall, little removal of many enteric microbes: – typically ~50% for viruses and bacteria

Enteric Microbe/Pathogen Reductions in Secondary or Biological Treatment • Aerobic biological treatment: typically, activated sludge (AS) or trickling filtration (TF) • Then, settle out the biological solids produced (2 o sludge) • ~90 -99% enteric microbe/pathogen reductions from the liquid phase • Enteric microbe retention by the biologically active solids: accumulation in AS flocs or TF biofilms • Biodegradation of enteric microbes by proteolytic enzymes and other degradative enzymes/chemicals • Predation by treatment microbes/plankton (amoeba, ciliates, rotifers, etc. • Aerobic microbes utililize carbon and other nutrients to form a healthy activated sludge AS biomass (floc) • The biomass floc is allowed to settle out in the next reactor; some AS is
 Treatment • Treatment of settled solids from 1 o and 2")
Waste Solids (Sludge) Treatment • Treatment of settled solids from 1 o and 2 o sewage treatment • Biological “digestion” to biologically stabilize the sludge solids – Anaerobic digestion (anaerobic biodegradation) – Aerobic digestion (aerobic biodegradation) – Mesophilic digestion: ambient temp. to ~40 o. C; 3 -6 weeks – Thermophilic digestion: 40 -60 o. C; 2 -3 weeks • Produce digested (biologically stabilized) sludge solids for further treatment and/or disposal (often by land application) – “Thickening” or “dewatering” – drying or “curing” • Waste liquids from sludge treatment are recycled through the sewage treatment plant • Waste gases from sludge treatment are released (or burned if from anaerobic digestion: methane, hydrogen, etc. )

Enteric Microbe/Pathogen Reductions by Sludge Treatment Processes • Anaerobic and aerobic digestion processes – Moderate reductions (90 -99%) by mesophilic processes – High reductions (>99%) by thermophilic processes • Thermal processes – Reductions depend on temperature • Greater reductions at higher temperatures • Temperatures >55 o. C usually produce appreciable pathogen reductions. • Alkaline processes: lime or other alkaline material – Reductions depend on p. H; greater reductions at higher p. Hs • p. H >11 produces extensive pathogen reductions • Composting: high temperature, aerobic biological process – Reductions extensive (>99. 99%) when temperatures high

“Processes to Further Reduce Pathogens” “PFRP”: Class A Sludge Class A sludge: • <1 virus per 4 grams dried sludge solids • <1 viable helminth ovum per 4 grams dried sludge solids • <3 Salmonella per 4 grams of dried sludge solids • <1, 000 fecal coliforms per gram dry sludge solids PFRPs: • Thermal (high temperature) processes (incl. thermophilic digestion); hold sludge at 50 o. C or more for specified times • lime (alkaline) stabilization; raise p. H 12 for 2 or more hours • composting: additional aerobic treatment at elevated temperature • Class A sludge or “biosolids” disposal by a variety

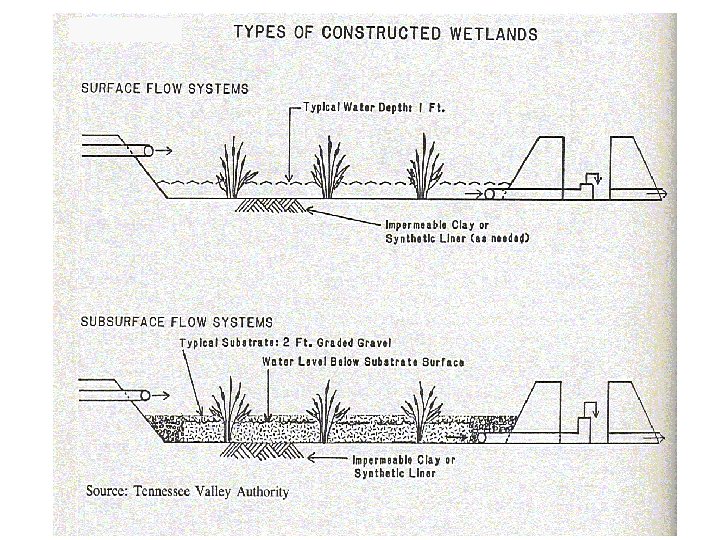
Alternative Biological Treatment of Wastewater: Alternatives for Small and Rural Communities • Lagoons, Ponds and Ditches – aerobic, anaerobic and facultative – for smaller communities and farms – enteric microbes are reduced by ~90 -99% per pond • multiple ponds in series increases overall microbe reductions • Constructed Wetlands – aerobic systems containing biologically active, oxidizing microbes and emergent aquatic plants – Microbial reductions comparable to or greater than ponds or lagoons. • Lagoons and constructed wetlands are practical and economical sewage treatment alternatives when land is available at reasonable cost
 Pond Pathogen reductions of 90 -99%, depending on design, operation")
Facultative Oxidation (Waste Stabilization) Pond Pathogen reductions of 90 -99%, depending on design, operation and conditions Two or more ponds in series achieve 90 -99% reduction per pond, giving 99 -99. 99% reduction in 2 ponds and 99. 9 -99. 9999% reduction in 3 ponds in series, etc,

Stabilization Ponds or Lagoons • Aerobic and Facultative Ponds: • Biologically Rx by complementary activity of algae and bacteria. • Used for raw sewage as well as primary‑ or secondary‑Rx’d. effluent. • Bacteria and other heterotrophs convert organic matter to carbon dioxide, inorganic nutrients, water and microbial biomass. • Algae use CO 2 and inorganic nutrients, primarily N and P, in photosynthesis to produce oxygen and algal biomass. • Many different pond designs have been used to treat sewage: • facultative ponds: upper, aerobic zone and a lower anaerobic zone. • Aerobic heterotrophics and algae proliferate in the
")
Enteric Microbe/Pathogen Reductions in Stabilization Ponds • BOD (a measure of biodegradable organic matter) and enteric microbe/pathogen reductions of 90%, esp. in warm, sunny climates • Even greater enteric microbe/pathogen reductions by using two or more ponds in series • Better BOD and enteric microbe/pathogen reductions if detention (residence) times are sufficiently long (several weeks to months) • Enteric microbes reduced by 90 -99% in single ponds and by multiples of 90 -99% for ponds in series. • Microbe removal often quite variable, depending upon pond design, operating conditions and climate. – Reduction efficiency lower in colder weather and with shorter retention times
 wetlands reduce enteric microbes")
Constructed Wetlands and Enteric Microbe Reductions • Surface flow (SF) wetlands reduce enteric microbes by ~90% • Subsurface flow (SSF) wetlands reduce enteric microbes by ~99% • Greater reduction in SSF may be due to greater biological activity in wetland bed media (porous gravel) and longer retention times • Multiple wetlands in series incrementally increase microbial reductions, with 90 -99% reduction per wetland cell.

Septic Tank-Soil Absorption Systems for On-Site Sewage Rx • Used where no sewers or community sewage treatment facilities: ex. : rural homes • Septic tank: solids settle and are digested • Septic tank effluent (STE) is similar to primary sewage effluent • Distribute STE to soil via a sub-surface, porous pipe in a trench • Absorption System: Distribution lines and drainfield • Septic tank effluent flows through perforated pipes 2 -3 feet below the land surface in a trenches filled with gravel, preferably in the unsaturated (vadose) zone. – Effluent discharges from perforated pipes into trench gravel and then into unsaturated soil, where it is biologically treated aerobically. – Enteric microbes are removed and retained by the soil and biodegraded along with STE organic matter; extensive enteric microbe reductions are possible – But, viruses and other pathogens can migrate through the soil and reach ground water if the soil is too porous (sand) and the water table is high
: Circular Flow/Recycling of Nutrients and Other Materials Basis and Approach: Considers")
Ecological Sanitation (Eco-San): Circular Flow/Recycling of Nutrients and Other Materials Basis and Approach: Considers urine, feces and water as resources in an ecological loop. Seeks to protect public health, prevent pollution and return nutrients and humus to the soil. Nutrient recycling to ensure food security. Separate urine and feces at source; Do not mixed with water. - avoid contaminating large volumes of water with pathogens. - separation make it easier to recover and recycle nutrients After dilution and/or processing, separated

Ecological Sanitation - Eco. San Advantages and options: • Affordable, flexible sanitation options for all • Wide range of toilet designs • Different ways to collect/treat urine/feces. • Low- and high-technology solutions for rural and urban settings. • Allows for central and/or decentralized management • Dry and/or waterborne systems

Log 10 Reduction of Pathogens by Wastewater Rx Processes

Log 10 Reduction of Pathogens by Wastewater Rx Processes

REMOVAL OF ENTERIC BACTERIA BY SEWAGE TREATMENT PROCESSES ORGANISM REMOVAL Fecal indicators 0‑ 60% E. coli 32 and 50% Fecal indicators 20‑ 80% Fecal indicators 40‑ 95% Fecal indicators high temp. PROCESS % Primary sed. Trickling filt. Activated sludge Stab. ponds, 1 mo. >99. 9999% @

Entamoeba histolytica Reduction by Sewage Treatment ORGANISM REMOVAL E. histolytica 50% E. histolytica 64% E. histolytica 27% E. histolytica 25% E. histolytica 74% E. histolytica 91% E. histolytica PROCESS Primary Sed. , 2 hr. Primary sed. , 1 hr. Primary sed. + Trickl. Filt. " " Primary sed. + Act. Sludge %

Microbial Reductions by Wastewater Treatment

Disinfection of Wastewater • Intended to reduce microbes in 1 o or 2 o treated effluent – Typically chlorination – Alternatives: UV radiation, ozone and chlorine dioxide • Good enteric bacterial reductions: typically, 99. 99+% – Meet fecal coliform limits for effluent dicharge • Often 200 -1, 000 per 100 ml geometric mean as permitted discharge limit • Less effective for viruses and parasites: typically, 9099% reduction • Toxicity of chlorine and its by‑products to aquatic life now limits wastewater chlorination; may have to: – Dechlorinate – Use an alternative, less toxic chemical disinfectant or – Use an alternative treatment process to reduce enteric microbes • granular medium (e. g. , sand) filtration

When Wastewater Disinfection is Recommended or Required • Discharge to surface waters: – – – near drinking water supply intakes used for primary contact recreation used for shellfish harvesting used for irrigation of crops and greenspace other direct and indirect reuse and reclamation purposes • Discharge to ground waters: – used as a water supply source – used for irrigation of crops and greenspace – other direct and indirect reuse and reclamation purposes

Wastewater Reuse • Wastewater is sometimes reused for beneficial, nonpotable purposes in arid and other water-short regions. • Widespread in developing countries; – often done poorly with inadequate reduction of pathogens/toxins • Often uses advanced or additional treatment processes, sometimes referred to as “reclamation” • Biological treatment in “polishing” ponds, constructed wetlands and other “natural” systems • Physical-chemical treatment processes used for drinking water: – – Coagulation-flocculation and sedimentation Filtration: granular medium filters; membrane filters Granular Activated Carbon adsorption Disinfection

Indicator Microbe Levels in Raw and Treated Municipal Sewage: Sewage Treatment Efficacy Number/100 ml 10000000 100000 1000 10 1 F. col. E. coli Ent. C. p. F+ phg. Raw ( -------Bacteria----- Bact. spores Viruses) Treated (geom. mean values of 24 biweekly samples)

Estimated Pathogen Reductions by Sewage Treatment Processes: An Example Sewage Treatment Rx: Total % Reduction • Primary settling 50 • 2 o biological treatment • Granular medium filtration 99. 95 • Disinfection 99 50 99 90 99. 5 99. 9995
 Water,")
Effect of Sanitation on Health Fewtrell, L. and J. M. Colford, Jr. (2004) Water, Sanitation and Hygiene: Interventions and Diarrhoea. A Systematic Review and Meta-

Effect of Sanitation on Health • Only 2 of 4 available studies could be included in the meta-analysis • Not possible to extract data from Kumar et al. (1970) or calculate CIs for Gross et al. (1989) • Children (i. e. ≤ 60 months): random effects pooled estimate = 0. 678 (95% CI: 0. 529 – 0. 868) Fewtrell L, Kaufmann RB, Kay D, Enanoria W, Haller L, Colford JM Jr. (2005) Water, sanitation, and hygiene interventions to reduce diarrhoea in less developed countries: a systematic review and metaanalysis. Lancet Infect Dis. 2005 Jan; 5(1): 42 -52.
 - Recent Data Barreto ML Et al. ,")
Effect of Sanitation on Health (Diarrhea) - Recent Data Barreto ML Et al. , Effect of city-wide sanitation programme on reduction in rate of childhood diarrhoea in northeast Brazil: assessment by two cohort studies. Lancet 2007; 370: 1622– 28 • A city-wide sanitation intervention was started in Salvador, Brazil, in 1997 to improve sewerage coverage from 26% of households to 80%. • The effect of this programme on diarrhea morbidity in children less than 3 years of age was studied • Two longitudinal studies: 1997– 98 before the intervention & 2003– 04 after the intervention. • Each study consisted of a cohort of children (841 in the preintervention study and 1007 in the postintervention study; age 0– 36 months at baseline); followed up to 8 months. • Children were sampled from 24 sentinel areas randomly chosen to represent the range of environmental conditions in the study site. Individual or household questionnaires were initially applied by trained fieldworkers; an environmental survey was done in each area before and after the sanitation programme to assess basic neighborhood and household sanitation conditions. • Daily diarrhoea data were obtained during home visits twice/week. • The effect of the intervention was estimated by a hierarchical modelling approach fitting a sequence of multivariate regression models. • Diarrhea prevalence fell by 21% (95% CI 18– 25%), from 9· 2 (9· 0– 9· 5) days per child-year before the intervention to 7· 3 (7· 0– 7· 5) days per childyear afterwards. – After adjusting for baseline sewerage coverage and potential
 - Recent Data Genser Et al. . (2008)")
Effect of Sanitation on Health (Diarrhea) - Recent Data Genser Et al. . (2008) Impact of a city-wide sanitation intervention in a large urban centre on social, environmental and behavioural determinants of childhood diarrhoea: analysis of two cohort studies. Int J Epidemiol. 37(4): 831 -40. • • • Poor socioeconomic status (SES) increases diarrhea risk – mostly via lack of sanitation, poor infrastructure and living conditions. The effectiveness of a city-wide sanitation intervention on diarrhea in a large urban site in Northeast Brazil was recently demonstrated. The intervention altered the magnitude of relative and attributable risks of diarrhea determinants and the pathways by which those factors affect diarrhea risk. Determinants of prevalence of diarrhea were determined in two cohort studies conducted before & after the intervention; in pre-school children followed for 8 mos. Relative, attributable and mediated risks of diarrhea determinants were estimated. The intervention reduced diarrhea and also changed attributable and relative risks of diarrhea determinants by altering the pathways of mediation. Before the intervention SES was a major distal diarrhea determinant (attributable risk: 24%) with 90% of risk mediated by other factors, mostly by lack of sanitation and poor infrastructure (53%). After the intervention, only 13% of risk was attributed to SES, with only 42% mediated by other factors (18% by lack of sanitation and poor infrastructure). The intervention reduced diarrhea risk by reducing direct exposure to

Impact of Improved Sanitation on Health • Improved sanitation reduces infectious diseases in developing world settings • Evidence from intervention studies, casecontrol studies and other epid. studies. • Data are limited; few studies; poor quality • Estimate of effect: in the 25 -45% range for reduction of diarrheal disease in children • Similar to the magnitude of the effect of improved water quality (or quantity)
 • An approach to facilitate the process of empowering")
Community Led Total Sanitation (CLTS) • An approach to facilitate the process of empowering local communities to stop open defecation and to build and use latrines or other effective sanitation without the support of any external hardware (construction materials) subsidy • Focuses on creating change in sanitation behavior through community participation rather than just constructing toilets. • Done through a process of social participation; behavior focus • Focuses on the whole community not individual behaviors • Emphasizing the collective benefit from stopping open defecation by encouraging a more cooperative approach • People decide together how they will create a clean and hygienic environment that benefits everyone. • Encourages local communities to visit the dirtiest and

10 Principles of CLTS 1. Aim/Target: 100% Total Sanitation 2. Based on creating Genuine Demand but not Charity 3. Thrives through aggressive Awareness but not through Subsidies 4. Recognizes a Wide Range of Technology Options 5. Technology Choice Based on Affordability, Appropriateness and acceptability 6. Lowest Requirement: Contain or Restrict Excreta (no open defecation) 7. Communities (Villagers) Plan, Implement Monitor their own progress 8. Government to support Long Term Sustainability of initiatives 9. Facilitation is done by an indigenous organiaations –

Key Steps in CLTS 1 ST Step: Realization of Unhygienic Sanitary Practices Through Analysis of Community Feces • Community Led Participatory Rural Appraisal (PRA) • A Walk of Shame – see actual situation on ground • Ground Mapping of Feces – where are they/whose • • are they! Calculation of Feces amounts - varies Raising Flag of Feces (Flagging) – where they are Village Commitment - no open defecation! Community sanitation policing

Key Steps in CLTS 2 nd Step: Organizing and Mobilizing the Community • Have Commitment towards No Open Defecation (NOD) Followed by Hygiene Promotion • Form Village Sub-committees – for Effective Implementation and Monitoring • Use existing community groups –child club, women and local cultural groups • Monitoring/Information using an open Board • Looking at future – community vision & dream • Family Monitoring Chart • Exchange Visits • NOD Declaration - (perhaps within 3 months) • Recognize well performing communities

Sanitation Policy Issues • Sanitation policy is a challenge • Sanitation lags far behind water in coverage and effective sustained use • Sanitation intervention hardware (latrines, other toilets, sewerage and sewage treatment) is usually a major infrastructure change and investment • Sanitation requires a personal and community behavior commitment to use the sanitation facilities • The drivers for behavior change in sanitation are complex and require considerable time and effort at the personal, household and community levels • Existing sanitation infrastructure is often poor and poorly maintained • Sanitation remains one of the biggest unmet global needs; new strategies and approaches needed
86fdd061d6c9cf326719d7f47cda3f44.ppt