

cb114c07345b4116bc24624875577891.ppt
- Количество слайдов: 43
 European Working Time Directive and its impact on training Medical Education England Independent Enquiry Chair Professor Sir John Temple June 2009
European Working Time Directive and its impact on training Medical Education England Independent Enquiry Chair Professor Sir John Temple June 2009
 • Healthcare ; • is always supervised, • and") European Working Time Directive (EWTD) • Healthcare ; • is always supervised, • and is usually delivered by trained doctors
European Working Time Directive (EWTD) • Healthcare ; • is always supervised, • and is usually delivered by trained doctors
 What is a ‘Trained Doctor’? • MB Ch B or equivalent X • Membership/Fellowship of Royal College X • Certificate of Completion of Training -CCT
What is a ‘Trained Doctor’? • MB Ch B or equivalent X • Membership/Fellowship of Royal College X • Certificate of Completion of Training -CCT
 Concern about the ability of the NHS to deliver training in 48 hr week • Review the impact of the EWTD on the training of – Dentists – Doctors – Healthcare Scientists – Pharmacists
Concern about the ability of the NHS to deliver training in 48 hr week • Review the impact of the EWTD on the training of – Dentists – Doctors – Healthcare Scientists – Pharmacists
 Time for Training A review of the impact of the European Working Time Directive on the quality of training Professor Sir John Temple
Time for Training A review of the impact of the European Working Time Directive on the quality of training Professor Sir John Temple
") A comprehensive review process (Dec 2009 – April 2010)
A comprehensive review process (Dec 2009 – April 2010)
 Evidence v Assertion • Real evidence is lacking • Repeated – Assertion – Opinion or – information was taken as a proxy for evidence • Trainees perceptions were very important!
Evidence v Assertion • Real evidence is lacking • Repeated – Assertion – Opinion or – information was taken as a proxy for evidence • Trainees perceptions were very important!
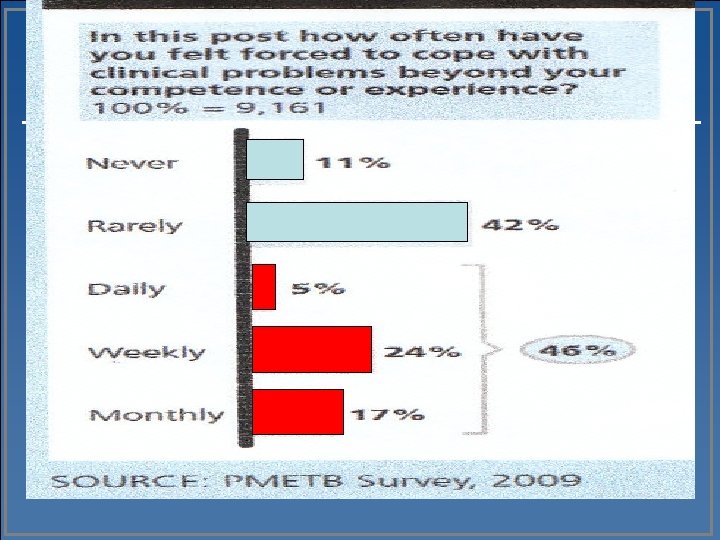
 EWTD impact • is greatest when workload involves; – high emergency and/or – out of hours cover
EWTD impact • is greatest when workload involves; – high emergency and/or – out of hours cover
 High Quality Training can be delivered in 48 hours • This is precluded when: trainees have a major role in out of hours service
High Quality Training can be delivered in 48 hours • This is precluded when: trainees have a major role in out of hours service
 EWTD impact • Training & service are inextricably linked • 48 hrs leads to > in shift working • Shifts require > doctors to maintain cover • Rota gaps > frequent
EWTD impact • Training & service are inextricably linked • 48 hrs leads to > in shift working • Shifts require > doctors to maintain cover • Rota gaps > frequent
 Rota Gaps Loss of elective training X 2 Generality not Speciality Limited learning Enforced rest Rota Gaps (usually out of hours) Poorly supervised
Rota Gaps Loss of elective training X 2 Generality not Speciality Limited learning Enforced rest Rota Gaps (usually out of hours) Poorly supervised
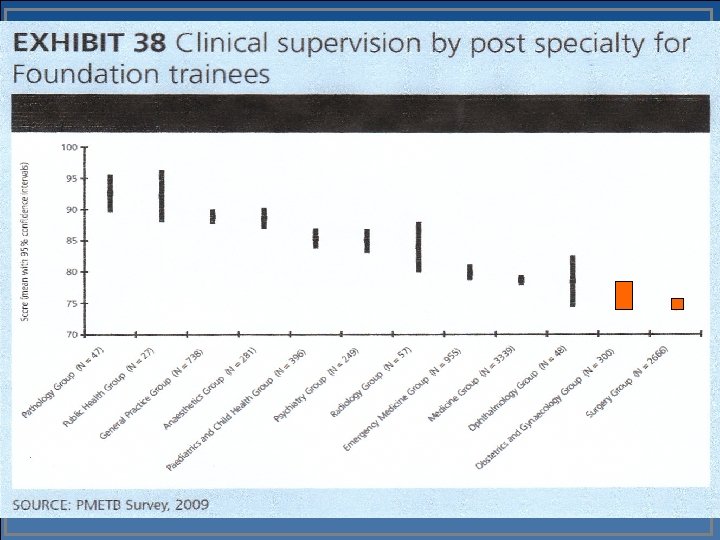
 The effect of service on training
The effect of service on training
 Just how much training is provided in the current working week in the UK? • In a 7 year training programme with 48 hrs/week • There are 15, 000 hours potentially available
Just how much training is provided in the current working week in the UK? • In a 7 year training programme with 48 hrs/week • There are 15, 000 hours potentially available
 Who covers the nights?
Who covers the nights?
 Findings – Consultant Expansion Trainee increases have enabled retention of existing services and configurations
Findings – Consultant Expansion Trainee increases have enabled retention of existing services and configurations
 Findings • Consultant ways of working often support traditional training models • Traditional service and training models waste learning opportunities
Findings • Consultant ways of working often support traditional training models • Traditional service and training models waste learning opportunities
 Comparisons Population • UK Med students Residents 60 m 8, 000 50, 000 • Canada 30 m 3, 500 10, 000
Comparisons Population • UK Med students Residents 60 m 8, 000 50, 000 • Canada 30 m 3, 500 10, 000
 Make every moment count -1 • Training must be; – Planned – Focused Handovers must be; -effective -safe -supervised
Make every moment count -1 • Training must be; – Planned – Focused Handovers must be; -effective -safe -supervised
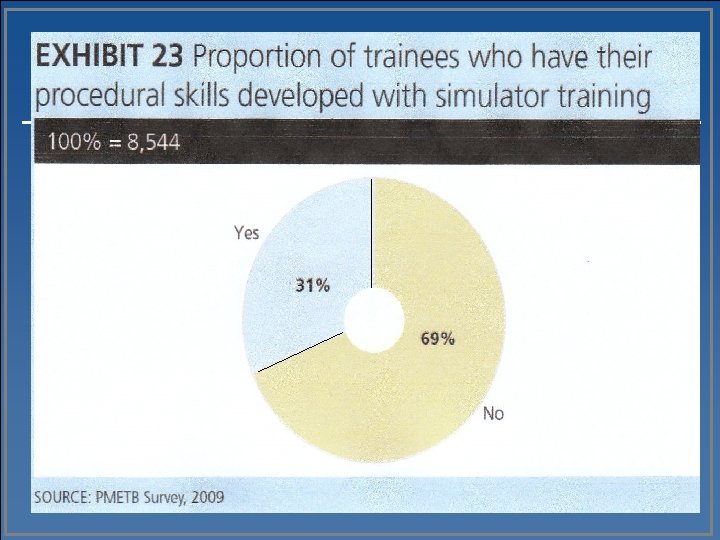
 Make every moment count -2 • Accelerate learning by using: – – Simulation Role play Video consultation Other technologies In controlled environments before practising on patients
Make every moment count -2 • Accelerate learning by using: – – Simulation Role play Video consultation Other technologies In controlled environments before practising on patients
 Skills Lab
Skills Lab
 Use of simulation accelerates the acquisition of skills
Use of simulation accelerates the acquisition of skills
 Effective implementation of EWTD results in – Improved work/life balance – Enhanced supervision – Reduced loss of daytime elective training – Improved handovers This produces safer patient care
Effective implementation of EWTD results in – Improved work/life balance – Enhanced supervision – Reduced loss of daytime elective training – Improved handovers This produces safer patient care
 EWTD can be a catalyst for change • Service reconfiguration • Hospital at Night • Consultant & Trainee contract flexibility • Training simulation and new technologies
EWTD can be a catalyst for change • Service reconfiguration • Hospital at Night • Consultant & Trainee contract flexibility • Training simulation and new technologies
 The case for change • Reliance on trainee doctors to deliver a 24/7 service has to change • Increasing – hours/length of training now will simply maintain the present system
The case for change • Reliance on trainee doctors to deliver a 24/7 service has to change • Increasing – hours/length of training now will simply maintain the present system
 Recommendations - 1 • Implement a consultant delivered service • Service delivery must explicitly support training • Learning must continue to be service based • Make every moment count
Recommendations - 1 • Implement a consultant delivered service • Service delivery must explicitly support training • Learning must continue to be service based • Make every moment count
 Consultant delivered service C T
Consultant delivered service C T
 Readily available Resident Graded supervision CDS Only when service load") Consultant delivered service (CDS) Readily available Resident Graded supervision CDS Only when service load demands) Viable sized teams call) No other duties Service re-organisation (when on
Consultant delivered service (CDS) Readily available Resident Graded supervision CDS Only when service load demands) Viable sized teams call) No other duties Service re-organisation (when on
 Consultant delivered service • Lead to closer supervision by consultants; – Increase learning opportunities – Improve, diagnosis & treatment – Enhance patient safety And reduced patient costs
Consultant delivered service • Lead to closer supervision by consultants; – Increase learning opportunities – Improve, diagnosis & treatment – Enhance patient safety And reduced patient costs
 What is a fully Trained Doctor? • Completed a training programme • Certificate of Completion of Training (CCT) • Appointed to a Consultant position in NHS
What is a fully Trained Doctor? • Completed a training programme • Certificate of Completion of Training (CCT) • Appointed to a Consultant position in NHS
 Consultant delivered service – Trainee programme 7 yrs – Consultant 25 -30 yrs Consultant: trainee alignment – Consultant : Trainee 3: 1
Consultant delivered service – Trainee programme 7 yrs – Consultant 25 -30 yrs Consultant: trainee alignment – Consultant : Trainee 3: 1
 Consultant delivered service Action > Consultants Service Ø < Trainees Teaching Not all consultants or services will have trainees
Consultant delivered service Action > Consultants Service Ø < Trainees Teaching Not all consultants or services will have trainees
 Consultant delivered service • 24 hr presence or ready availability for direct patient care • More flexible working of the consultant contract • Multi disciplinary Team - not ‘Firm’ approach • Mentoring of all consultants
Consultant delivered service • 24 hr presence or ready availability for direct patient care • More flexible working of the consultant contract • Multi disciplinary Team - not ‘Firm’ approach • Mentoring of all consultants
 Recommendations - 2, 3 & 4 • Some service redesign is necessary • Recognise, develop and reward training • Training excellence requires regular planning and monitoring
Recommendations - 2, 3 & 4 • Some service redesign is necessary • Recognise, develop and reward training • Training excellence requires regular planning and monitoring
 Public Expectation Right Healthcare ; - • is always supervised, • and is usually delivered by trained doctors
Public Expectation Right Healthcare ; - • is always supervised, • and is usually delivered by trained doctors
 High quality training can be delivered in 48 hrs • To achieve this the NHS needs: – – – Fundamental changes to training & service Clear Leadership An explicit implementation plan Action is needed now
High quality training can be delivered in 48 hrs • To achieve this the NHS needs: – – – Fundamental changes to training & service Clear Leadership An explicit implementation plan Action is needed now
 ‘Training today is patient safety for the next 25 -30 years’ • We must produce Competent, confident and safe doctors who will embrace life long learning.
‘Training today is patient safety for the next 25 -30 years’ • We must produce Competent, confident and safe doctors who will embrace life long learning.
 EWTD – the fine points • Introduced • Full implementation – 48 hrs – 1/8/09 • Working time includes – on the job training on call at the workplace • Junior doctors are not classed as night workers • Simap & Jaegar rulings 1998
EWTD – the fine points • Introduced • Full implementation – 48 hrs – 1/8/09 • Working time includes – on the job training on call at the workplace • Junior doctors are not classed as night workers • Simap & Jaegar rulings 1998
 Time for Training A review of the impact of the European Working Time Directive on the quality of training Professor Sir John Temple
Time for Training A review of the impact of the European Working Time Directive on the quality of training Professor Sir John Temple