4593c7b1985f3c78c9de067b436f413e.ppt
- Количество слайдов: 45



Esophageal and Swallowing Disorders Brenda Beckett, PA-C UNE PA Program

We’ll Cover n Dysphagia – Obstructive disorders • Schatzki Ring • Esophageal Web – Motility disorders • Achalasia • Diffuse Esophageal Spasm n GERD n Diverticula n Mallory Weiss Syndrome n Esophageal varices n Esophageal rupture

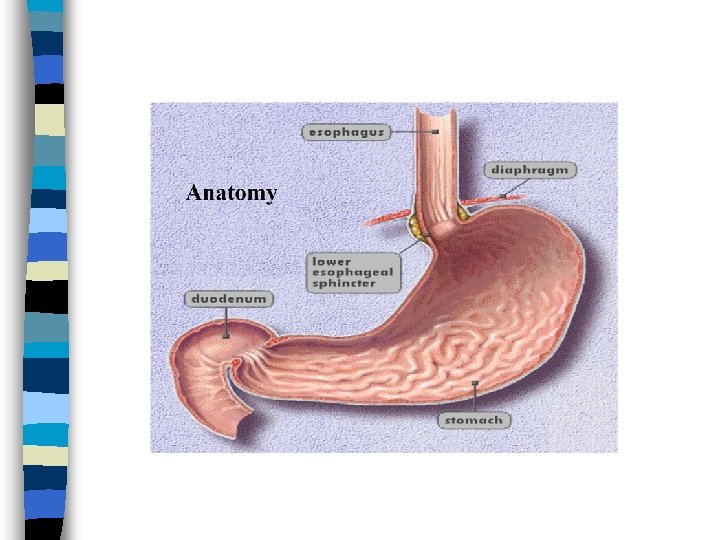
Esophagus n Muscular tube about 25 cm long extending from the hypopharynx to the stomach. n Lies posterior to the trachea and heart. n Passes through the mediastinum and the hiatus in its descent from the thoracic to the abdominal cavity. n Terminates at cardia or LES
: Substernal")
Symptoms n Dysphagia: Difficulty swallowing n Odynophagia: Pain with swallowing n Heartburn (pyrosis): Substernal burning, can radiate to neck

Diagnostic Studies n Upper endoscopy: Study of choice for many esophageal disorders. Visualization and biopsy n Barium Esophagography: Differentiate mechanical from motility n Esophageal Manometry: Pressure. n p. H recording: Reflux

Dysphagia Difficulty swallowing. “Food gets stuck” n Oropharyngeal dysphagia- abnl function proximal to esophagus n – Neuro or muscular etiology, ie: Parkinsons, MS, MD, MG n Esophageal dysphagia- difficulty passing food down esophagus due to either – Mechanical obstruction – Motility disorder

Obstructive Disorders n Dysphagia to solids – Bread and meat especially n Lower Esophageal Ring n Esophageal Web n Neoplasms (covered in separate lecture)

Lower Esophageal Ring n Schatzki’s Ring n 2 -4 mm mucosal stricture, usually congenital n Causes circumferential narrowing at squamocolumnar junction at distal esophagus n Severity of sx based on lumen size

Schatzki Ring n Assoc with hiatal hernia n Dx: endoscopy or barium esophagography n Tx: – Chew thoroughly – Endoscopic dilation

Esophageal Web n Thin mucosal membrane across lumen of upper esophagus n Dysphagia to solids n Seen with severe iron deficiency anemia (as part of Plummer-Vinson) n Dx and tx by endoscopy, also will resolve with tx of Fe-deficiency anemia

Achalasia n Neurogenic esophageal motility disorder characterized by: -impaired esophageal peristalsis -lack of lower esophageal sphincter relaxation during swallowing -elevation of lower esophageal sphincter resting pressure

Achalasia n Onset age 20 -40 n Progressive dysphagia – Both liquids and solids n Nocturnal regurgitation of undigested foods in 1/3 of patients

Etiology n? Perhaps viral? n Can be secondary to mechanical obstruction or paraneoplastic process n Loss of ganglion cells in mesenteric plexus of esophagus n Leads to denervation of esophageal musculature

Achalasia Dx n Barium studies: – Absence of progressive peristaltic contractions during swallowing – Significant esoph dilation – Narrowed “birds beak” distal esoph (at LES) n Manometry: – Lack of peristalsis, lack of relaxation of LES

Achalasia

Complications n Nocturnal regurgitation n Cough n Aspiration – pnemonitis

Achalasia Treatment n There is no treatment to restore peristalsis n Goal: decrease LES pressure – Balloon dilation of LES, may repeat – Drugs: Nitrates, CCB, Botox n Surgery: Heller myotomy

Diffuse Esophageal Spasm n Non-productive esophageal contractions n Hyperdynamic contractions n Increased LES pressure

Esoph Spasm Sx n Substernal squeezing chest pain – With dysphagia for liquids and solids n May occur with exertion n May occur with esoph temp extremes n Sound familiar? ? Can be indistinguishable from angina pectoris or myocardial infarction n Dysphagia uncommon sx

Esoph Spasm Dx n Rule out coronary ischemia n Barium swallow: – Poor progression of bolus – Disordered, simultaneous contractions n Esophageal manometry – Simultaneous, prolonged, high amplitude contractions – “Nutcracker esophagus” – pressure so high it can crack a nut

Treatment n CCBs n Botox n Nitrates n Others

Esophageal Diverticula n Outpouching of mucosa through the muscular layer of the esophagus n Asymptomatic or dysphagia and regurgitation

Zenker’s diverticulum n Posterior outpouchings of mucosa and submucosa through the cricopharyngeal muscle n Likely results from an incoordination between pharyngeal propulsion and cricopharyngeal relaxation n SX: Regurg, choking, protrusion in neck n TRT: surgery, stapling

Zenker’s Diverticulum

GERD n Gastroesophageal reflux disease – Reflux of stomach contents causing symptoms n Incompetent LES from: – General loss of intrinsic sphincter tone – Recurrent inappropriate relaxations triggered by gastric stretch Allows reflux of gastric contents into esophagus n Frequent in infants (also GER) n

Factors contributing to LES Competence Angle of cardioesophageal junction n Action of diaphragm n Gravity n

GERD & Hiatal Hernia n Hiatal hernia occurs when the LES, upper part of the stomach moves up into the chest through a small opening in the diaphragm (diaphragmatic hiatus). n The diaphragmatic hiatus acts as an additional sphincter around the lower end of the esophagus

Factors Contributing to Reflux n n n n Weight gain Fatty foods Caffeine Carbonated beverages Eto. H Tobacco Increased intrabdominal pressure Drugs: anticholinergics, antihistamines, TCAs, CCBs, nitrates, progesterone

Symptoms n Heartburn – Substernal burning – Regurgitation (I think I just threw up in my mouth…) n Hypersalivation (from smoking as well) n Belching, nausea n Dysphagia, odynophagia n *Cough, wheezing, hoarseness, asthma

Complications n Esophagitis n Peptic esophageal ulcer n Esophageal stricture n Barrett’s esophagus

GERD Dx n Detailed history n Typical symptoms get trial treatment n Work-up reserved for: – Longstanding sx – Symptoms of complications – Pts who fail empiric tx n Endoscopy with biopsy
 n NO: n – – –")
GERD Tx HOB 6 inches (not just pillows) n NO: n – – – Eating within 3 hours of bedtime, large meals Acidic foods(coffee, citrus, tomatoes, etc) Drugs (see list of contributors to sx) Smoking (hyposalivation) Foods that weaken LES (fatty foods, alcohol, chocolate, peppermint) Meds: PPI x 8 -12 weeks (better than H 2 blockers, antacids or pro-motility meds) n Weight loss n Surgical: Fundoplication n

Nissen Fundoplication
 n Pill esophagitis – Direct erosive effects n Radiation")
Esophagitis n GERD (Most common) n Pill esophagitis – Direct erosive effects n Radiation esophagitis n Infectious esophagitis – Usually in immunocompromised pts – Candida, CMV, HSV

Esophagitis n Symptoms – Odynophagia. Pain on swallowing – Dysphagia – Chest pain: substernal – Signs of infection

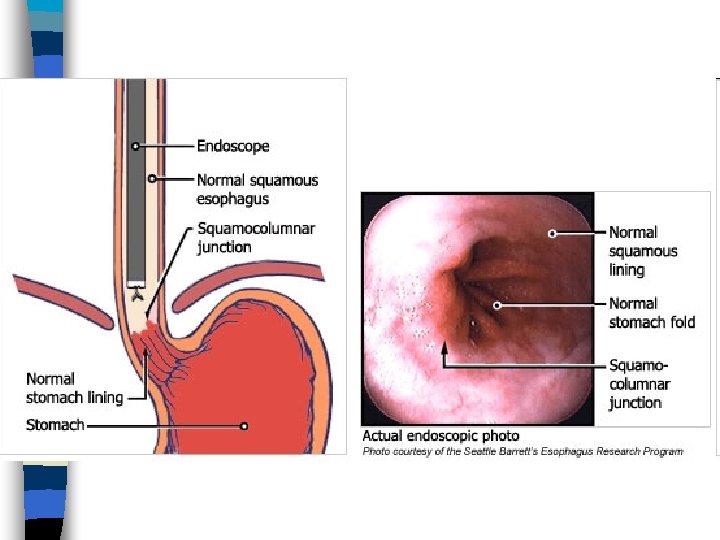
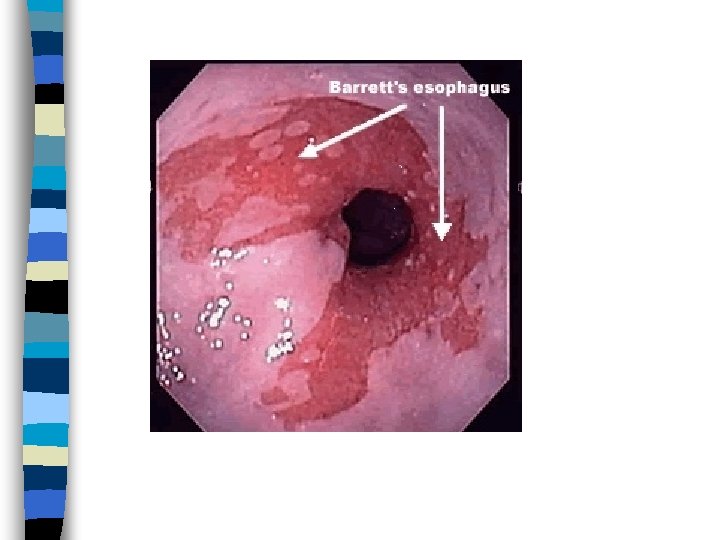
Barrett’s Esophagitis n Normal stratified squamous epithelium of distal esophagus replaced by: – Metaplastic, columnar, glandular intestinelike mucosa n Can give rise to adenocarcinoma n Warrants frequent surveillance by endoscopy

Esophageal varices Usually caused by portal hypertension secondary to cirrhosis n Can cause painless, sometimes massive upper GI bleed n Bright red hematemesis n – NOT coffee-ground emesis First, stabilize the pt: fluid resuscitation, blood transfusion, etc n Then endoscopic/surgical repair n

Mallory-Weiss Syndrome Non-penetrating mucosal laceration of distal esoph/proximal stomach n Caused by vomiting, retching, hiccupping n Often seen in alcoholics, but any forceful vomiting will do n Can cause significant bleeds n – Most stop spontaneously – 10% require transfusion – May need cauterization

Esophageal Rupture n Iatrogenic – ie: during endoscopy n Spontaneous – Boerhaave Syndrome (usu vomiting, so not truly spontaneous, but differentiates from iatro)

Esoph Rupture n MC site distal esophagus, L side n Acid and stomach contents cause fulminant medistinitis, pneumomediastinum, shock. n Bad.

Esoph rupture S/S n Sx: chest, abd, thoracic pain, hematemesis, shock n Did I say BAD? n Subcutaneous emphysema palpable in 30% n Hamman’s sign- mediastinal crunch – Crackling synchronous with heartbeat. – Cool

Rupture Dx & Tx n Imaging – Mediastinal air & widening, pleural effusion n Confirm with esophagography with water soluble contrast dye n Broad spectrum abx, fluid resuscitation, surgical repair. n High mortality
4593c7b1985f3c78c9de067b436f413e.ppt