d25fdbcad543f4444c8d225e411a76db.ppt
- Количество слайдов: 47



ENTEROVIRAL INFECTIONS Dr. B. Boyle Copyright©breida

ENTEROVIRAL INFECTIONS Contents of Lecture l ENTEROVIRUSES l Also Discuss , Viruses that cause Gastroenteritis l ROTAVIRUS l SMALL ROUND STRUCTURED VIRUSES e. g Norwalk virus, Novovirus etc. Copyright©breida

ROTAVIRUS Copyright©breida

ROTAVIRUS l l l l Description Epidemiology Pathogenesis Clinical Features Diagnosis Treatment The Future Copyright©breida

ROTAVIRUS l First described in 1973 by electron microscopy from duodenal biopsy specimens l Causes 40 -60% of cases of diarrhoea in cooler months in infants and children < 2 years Copyright©breida

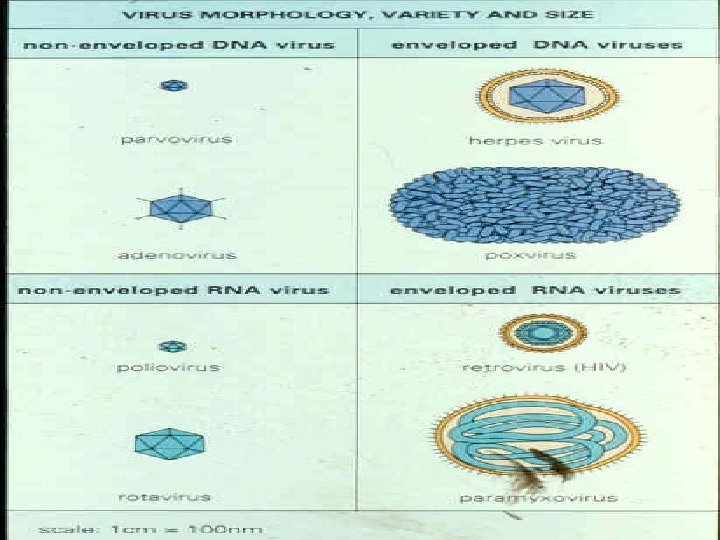
Morphology-Rotaviruses Reoviridae Family l Non-enveloped icosahedral structure, 70 nm l EM: Wheel shape l Capsid: Outer(VP 7 and 4) and Inner(VP 6) proteins l Core encloses 11 segments of DS RNA Genome encoded Structural proteins VP 17 and NSP 1 -5, NSP 4 has enterotoxinlike activity l Copyright©breida

Epidemiology of Rotavirus l l l Incubation period : 2 -4 days Those affected : 4 -24 month old infants, infection before and reinfection after this usually asymptomatic (Breastfeeding results in milder disease) Spread within families and institutions Most common cause of noscomial diarrhoea Human to human, faecal-oral route Found on fomites in childcare Copyright©breida

Epidemiology of Rotavirus l l l l Main cause of severe diarrhoea in children < 5 years 130 million episodes per year in the world Between 600, 000 -870, 000 deaths, mostly in the developing world Rate of hospitalisation in developed world 2. 5% Seasonal pattern Most persons infected by 3 years of age Group A predominates Copyright©breida

Classfication-Rotavirus Groups, Subgroups and serotypes depending on the antigenic properties of the capsid proteins l Group-VP 6, seven exist A-G, 2 subgroups 1 -2 l Groups A, B, C cause human infection l Copyright©breida
 Villous Atrophy Compensatory Repopulation by")
Rotavirus-Pathogensis Infects Mature Enterocytes(on tips of Small Intestine villi) Villous Atrophy Compensatory Repopulation by immature Secretor cells and secondary hyperplasia Copyright©breida

Mechanism of diarrhoea? Villous epithelium in relation To secretory capacity of Crypt cells Enteric nervous system stimulates Induction Of intestinal Water And electrolyte secretion Loss of permeability to Macromolecules e. g Lactose, Due to loss of disaccharideases Copyright©breida

Immune Response to Rotavirus Localised Immune response protects against severe subsequent infections l NSP 4 protein results in cell mediated immunity l Copyright©breida

Outcome of Infection with Viruses Lysis of cells e. g Influenza or polio l Persistent infection e. g. cell remains alive and continues to release virus particles e. g. Hepatitis B , CHRONIC CARRIER STATE l Latent Infection , no replication – Varicella Zoster or retrovirues , if triggered leads to lysis l Transformation of host cells e. g. warts or papovaviruses, HTLV 1 and 2 l Copyright©breida

Clinical Presentation. Rotavirus Abrupt onset of vomiting followed within hours by watery, brown copious diarrhoea, often lasts 3 -8 days l If Severe Dehydration and death or hospitalisation l Copyright©breida

DIAGNOSIS Clinically l Latex agglutination Kit testing for Group A Rv antigen in stool Enzyme Immunoassay Group A Rv antigen in stool Less common EM and molecular methods l Pos and neg Copyright©breida

TREATMENT l REHYRATE, oral and if severe parenteral l Some studies in immunocompromised persons showing the use of Human Immunoglobulin results in a reduction in the duration of symptoms and decreases viral sheeding l ISOLATION of patient in hospital with contact prescautions Copyright©breida

MANAGEMENT l In Home: Washing of surfaces with soap and water which may be contaminated with Rotavirus l 70% ethanol solution will kill the virus on environmental surfaces Copyright©breida

FAMILY: PICORNAVIRIDAE ENTEROVIRUSES Over 72+ RHINOVIRUS Type 1 -100+ Cardiovirus Aphthousvirus etc POLIO virus type 1, 2, 3 COXSACKIE A virus type 1 -22, 24 COXSACKIE B virus type 1 -6 E. C. H. O virus type 1 -7, 11 -27, 29 -34 Numbered ENTEROVIRUSES type 68 -71, 73 Since 1967 -all new ones are numbered E. C. H. O = enteric cytopathic human orphan Copyright©breida
 icosahedral capsid enclosing postive sense single")
Characteristics VIRON= naked , small (25 -30 nm) icosahedral capsid enclosing postive sense single stranded RNA l Enteroviruses are resistant to p H 3 -9, Heat, Mild sewage treatment and detergents, conditions in GIT = FACILATES faecal oral spread l Copyright©breida

Characteristics l l l Rhinovirus labile to acidic p H Genome of Enteroviruses is m RNA Naked genome is sufficient for infection Replication in cytoplasm Cytolytic viruses Copyright©breida
 Neurological: e. g Poliomyelitis, Aseptic meningitis and encephalitis")
Clinical Manifestations of EV Infections(Mostly Children) Neurological: e. g Poliomyelitis, Aseptic meningitis and encephalitis l Neonate: neonatal sepsis EV 11 l Non-specific febrile illness l Hepatitis gi etc l Haemorrhagic conjunctivitis, COX A 24 and EV 71 l l l l Respiratory Symptoms e. g colds, herangina Skin Exanthem with meningitis Myocarditis Those associated with Coxsackie viruses Spread: Faecal oral route , respiratory route and peripartum mother to infant or fomite transmission IP: 3 -6 DAYS Copyright©breida

COXSACKIE VIRUSES l 29+ immunogenic types l Divided into A and B on the basis of different pathogenic potential for mice l Result in a number of different clinical presentations Copyright©breida

COXSACKIE VIRUSES l l l Herangina Summer minor illness Aseptic meningitis Neonatal Disease Colds Hand , Foot and mouth illness l Myocarditis l ? Diabetes mellitus l Epidemic myalgia (Bornholm Disease) l Copyright©breida

ECHO Viruses l General properties similar to other enteroviruses l 30+ antigenic types l Results in: - 1. Aseptic meningitis 2. Rash 3. Conjunctivits 4. Upper Respiratory Tract Infection Copyright©breida

Management l l l Supportive Capsid function inhibitors: Pleconaril, broad spectrum, potent to Rhino and enteroviruses, good oral bioavailibility This compound binds to the floor of a VP 1 and VP 3 canyon floor , prevents binding to receptor on cells Used in cases of meningoencephalitis shown to be effective As humoral immunity is the body`s defence for enteroviruses, those who have deficiencies (congenital –or acquired)are given Intravenous Copyright©breida Immunoglobulin

POLIO VIRUS Copyright©breida

Polioviruses are RNA , ENTEROVIRUSES l 3 Serotypes 1, 2 , 3 l Major cause of paralytic poliomyelitis and now seeing post polio syndrome l Global Eradication Programme of WHO l Copyright©breida

EPIDEMIOLOGY l l l Human host Spread: Faecal or Respiratory routes More common in infants and young children, but risk of paralytic disease increases with age No indigeous wild type polio in U. S since 1979, imported in 1993, last wild type case in Ireland 1984 Vaccine Associated Paralytic Polio(VAPP) WHEN ORAL POLIO VACCINE (OPV) was in use( Reversion to wild type) now inactivated polio vaccine used(IPV) used in Ireland since 2001 Copyright©breida

EPIDEMIOLOGY l Risk of VAPP is one case per 2. 5 million doses, greatest risk with first dose l If using OPV strict hygiene after nappy changing or toileting should be observed for 6 weeks Copyright©breida

PRESENT VACCINE SCHEDULE At birth- 1 month BCG *At 2 months Diphtheria Whooping Cough Tetanus Hib Inactivated Polio + Meningococcal C *At 4 months Diphtheria Whooping Cough Tetanus Hib Inactivated Polio + Meningococcal C Usually in maternity hospitals 5 -in-1(G. P) Copyright©breida

PRESENT SCHEDULE *At 6 months *At 12 - 15 months Diphtheria Whooping Cough Tetanus Hib Inactivated Polio + Meningococcal C Measles Mumps Rubella, Hib 1 5 -in-1(G. P) MMR Hib 1 Copyright©breida

PRESENT SCHEDULE **4 -5 YEARS **11 -12 YEARS Diphtheria Whooping Cough Tetanus Inactivated Polio + Measles Mumps Rubella 4 -in-1 MMR Omit if 2 previous doses have been given Copyright©breida
 **10 -14 years if not")
PRESENT SCHEDULE **11 -14 years Tetanus Diphtheria (low dose) **10 -14 years if not protected(immune) BCG 2 (AN INTERVAL OF 4 WEEKS AFTER MMR) Under 23 years(Colleges etc) Meningococcal C Td Copyright©breida • From Family Doctor 1: A single dose of Hib vaccine if child presents after 13 months and has no previous Hib vaccine 2: Only those known to be tuberculin negative and have no previous BCG **These immunizations are generally administered in schools by Health Boards

Clinical Presentations of Poliovirus Infection l l l Approx. 95% of infections are ASYMPTOMATIC Minor illness in 4 -8% of lowgrade fever, sore throat Aseptic Meninigits in 1 -5% Asymmetrical acute flaccid paralysis with areflexia of limbs involved in 0. 1%-2% of infections (Respiratory Muscles may be involved) Residual Paralytic Diease in 2/3 of these Some develop Post-Polio syndrome 30 -40 years post infection with return of muscle pain and Copyright©breida weakness

Pathogenesis of Enteroviral Infection Evades Virus Replicates in Binds Enterocytes Nasopharnyx Acidic PH Receptor coded by Ch 19 Minor Viraemia, Replication in organs Major Viraemia + Trophism + Virulence Skeletal Muscle Neuromuscular Endplate Endocytosed , replication in Peyer`s patches Ascends along Motor Nerves Anterior Motor Neuron horn cells To CNS* Copyright©breida

Communciability This is greatest shortly before and after onset of clinical illness when virus in the throat and it is excreted in high concentrations in faeces l For OPV RECIPIENTS, VIRUS IN THE THROAT 1 -2 WEEKS AND FAECES FOR SEVERAL WEEKS USUALLY MAX 6 -8 WEEKS IN NORMAL IMMUNOCOMPOTENT INDIVIDUAL. l Copyright©breida

Surveillance l For Acute flaccid paralysis l Since September 1998 l Two faecal specimens 24 -48 hours apart for viral culture as soon as possible after onset of acute flaccid paralysis l Faeces most likely to yield virus Copyright©breida

TREATMENT/PREVENTION l Supportive l Prevention is by Vaccination. l Global Eradiation Programme l Part of Routine immunisation schedule and travellers to endemic areas should be vaccinated Copyright©breida

SLV-Novovirus. Calciviruses Family: Calciviridae l Single Stranded RNA, ps l Consists of Single Structural Capsid protein with icosahedric symmetry but has 32 cup -shaped depressions on the axes of the Icosahedron hence the name calyx l Multiple antigenic types l Copyright©breida

Pathogenesis of Disease l l l Not fully understood although some evidence suggesting it may be simliar to Rotavirus Causes delayed gastric emptying Immunity: infection induces specific IG G/A/M even if there is previous exposure 2 weeks post infection there is ⇧ in jejunal Ig A , resistance to reinfection lasts 4 -6 months, NO LONG TERM PROTECTION Accounts for >85% of non-bacterial outbreaks of gastroenteritis Copyright©breida

EPIDEMIOLOGY l l l Sporadic cases however causes epidemic outbreaks Examples: on cruise ships, hotels, Institutions and hospitals Spread: Person to person via faecal oral route or through contaminated food or water or fomites Incubation Period: 12 -72 hours Vomitus /Faeces infectious

CLINICAL FEATURES l l l DIARRHOEA VOMITING Commonly accompanied by fever, malaise, myalgia and abdominal cramps Symptoms last 1 day to 2 weeks Virus excreted 5 to 7 days after the onset of symptoms in half of people although may last 13 days Copyright©breida
 Electron Microscopy l Labour intense l Relatively insensitive l Used in Sporadacic")
Diagnosis(sample: stool) Electron Microscopy l Labour intense l Relatively insensitive l Used in Sporadacic cases l Reverse Transcriptase Polymerase chain reaction (RT-PCR) l Used in outbreaks as large numbers can be processed efficiently l Copyright©breida

Treatment l Supportive therapy: rehydration, electrolyte replacement l Isolation of Hospitalised patient l Control Measures: Standard and Contact precautions l No Vaccine Copyright©breida

Control Measures in Hospital Outbreaks l l l l Isolation or Cohort Contact Precautionsdisposable plastic apron/ gloves, Hand Hygiene Close Ward to Admissions Non-essential personnel excluded Avoid Transfers If Staff unwell not return to work until free from symptoms 72 hours Increase frequency of ward cleaning l l l Vomit/Faeces to be cleaned and disinfected promptly Hypochlorite(0. 1%) used to disinfect surfaces Cohort Staff Movement unaffected to affected area Ward not reopened until 72 hours after last new case or after last vomiting/diarrhoea Terminal cleaning Copyright©breida

The Future l Plasmidic DNA and Antigen Vaccines l Interrrupt Transmission l Supportive Therapy Copyright©breida
d25fdbcad543f4444c8d225e411a76db.ppt