

7f7b6487571fb56fa4c00541515dde7c.ppt
- Количество слайдов: 84
 Engaging Hard-to-Reach Populations: Inreach May 1, 2013
Engaging Hard-to-Reach Populations: Inreach May 1, 2013
 project Sarah Cook-Raymond, Impact Marketing") Agenda Introduction to SPNS Integrating HIV Innovative Practices (IHIP) project Sarah Cook-Raymond, Impact Marketing + Communications Presentations from SPNS grantees on using data to improve inreach Jane Herwehe & De. Ann Gruber, Louisiana Public Health Information Exchange (La. PHIE) Peter Gordon, New York-Presbyterian Hospital/Columbia University Jesse Thomas, RDE Systems Brief post-Webinar questionnaire Q&A
Agenda Introduction to SPNS Integrating HIV Innovative Practices (IHIP) project Sarah Cook-Raymond, Impact Marketing + Communications Presentations from SPNS grantees on using data to improve inreach Jane Herwehe & De. Ann Gruber, Louisiana Public Health Information Exchange (La. PHIE) Peter Gordon, New York-Presbyterian Hospital/Columbia University Jesse Thomas, RDE Systems Brief post-Webinar questionnaire Q&A
 IHIP Resources on TARGET Center Website www. careacttarget. org/ihip
IHIP Resources on TARGET Center Website www. careacttarget. org/ihip
 IHIP Resources: Innovative Approaches to Engaging Hard-to-Reach Populations Living with HIV/AIDS into Care IHIP Tools on Engaging Hard-to-Reach Populations Training Manual Curriculum Webinar Series Outreach – April 18; archive recording to be up soon! Inreach – May 1 Empowering the Patient - May 15
IHIP Resources: Innovative Approaches to Engaging Hard-to-Reach Populations Living with HIV/AIDS into Care IHIP Tools on Engaging Hard-to-Reach Populations Training Manual Curriculum Webinar Series Outreach – April 18; archive recording to be up soon! Inreach – May 1 Empowering the Patient - May 15
 ENGAGING HARD TO REACH POPULATIONS THRU IN REACH HRSA RYAN WHITE SPNS WEBINAR MAY 1, 2013 DEANN GRUBER, JANE HERWEHE, BETSY SHEPARD, &DEBBIE WENDELL LOUISIANA OFFICE OF PUBLIC HEALTH AND LOUISIANA STATE UNIVERSITY HEALTH CARE SERVICES DIVISION
ENGAGING HARD TO REACH POPULATIONS THRU IN REACH HRSA RYAN WHITE SPNS WEBINAR MAY 1, 2013 DEANN GRUBER, JANE HERWEHE, BETSY SHEPARD, &DEBBIE WENDELL LOUISIANA OFFICE OF PUBLIC HEALTH AND LOUISIANA STATE UNIVERSITY HEALTH CARE SERVICES DIVISION
 A Collaborative Initiative funded in part by: HRSA HIV/AIDS Bureau Office of Science and Policy Special Projects of National Significance Grant # H 9 HA 08476
A Collaborative Initiative funded in part by: HRSA HIV/AIDS Bureau Office of Science and Policy Special Projects of National Significance Grant # H 9 HA 08476
 A carefully designed two-way electronic information exchange Uses OPH surveillance data to generate point of care messages for providers in the LSU HCSD (public hospital) system in Louisiana Targets patients with HIV who have fallen out of care, or never received test results, as well as persons with TB or syphilis who are in need of treatment
A carefully designed two-way electronic information exchange Uses OPH surveillance data to generate point of care messages for providers in the LSU HCSD (public hospital) system in Louisiana Targets patients with HIV who have fallen out of care, or never received test results, as well as persons with TB or syphilis who are in need of treatment
 q HIV Surveillance Database q Laboratory Database Filte r busi ed data se ness rule t after s ap plied Target populations: §Persons considered “not in care” (no record of CD 4/VL in 9* months) §Persons who have not received test results and may be unaware of HIV status §HIV-exposed infants in need of follow-up La. PHIE Server q. La. PHIE Database q. Communication system: MIRTH – open source (behind OPH firewall)
q HIV Surveillance Database q Laboratory Database Filte r busi ed data se ness rule t after s ap plied Target populations: §Persons considered “not in care” (no record of CD 4/VL in 9* months) §Persons who have not received test results and may be unaware of HIV status §HIV-exposed infants in need of follow-up La. PHIE Server q. La. PHIE Database q. Communication system: MIRTH – open source (behind OPH firewall)
 Disease Alert (PPR) Disease Alert Response (PRR) La.") on issi tion Admission Information (ADT) Disease Alert (PPR) Disease Alert Response (PRR) La. PHIE Server In ma for eas Dis eas e. A Registration e. A lert Interface Engine lert Res pon se EMR Office of Public Health Firewall LSUHCSD Firewall
on issi tion Admission Information (ADT) Disease Alert (PPR) Disease Alert Response (PRR) La. PHIE Server In ma for eas Dis eas e. A Registration e. A lert Interface Engine lert Res pon se EMR Office of Public Health Firewall LSUHCSD Firewall
 Physician follows onscreen steps to re-engage patient into care and provide HIV treatment, as appropriate Patient comes to clinic, hospital, or ED for non. HIV service Real time communication with surveillance system alerts physician that patient needs attention for HIV/AIDS HIV clinic 10
Physician follows onscreen steps to re-engage patient into care and provide HIV treatment, as appropriate Patient comes to clinic, hospital, or ED for non. HIV service Real time communication with surveillance system alerts physician that patient needs attention for HIV/AIDS HIV clinic 10
 ü Established partnership, governance and agreements Assessed and modified technical infrastructure ü Designed messaging with iterative prototype process ü Conducted consumer research ü Participated in an ethics review by national experts in biomedical ethics, public health ethics and AIDS privacy ü Requested a legal review of legislation related to sharing of public health information ü Raised community awareness and readiness ü Prioritized open dialogue and established feedback mechanisms
ü Established partnership, governance and agreements Assessed and modified technical infrastructure ü Designed messaging with iterative prototype process ü Conducted consumer research ü Participated in an ethics review by national experts in biomedical ethics, public health ethics and AIDS privacy ü Requested a legal review of legislation related to sharing of public health information ü Raised community awareness and readiness ü Prioritized open dialogue and established feedback mechanisms
 Essential questions: We have the information and the technical ability to inform clinicians about patients in need of care … BUT SHOULD WE? Would this be accepted by patients, providers, and the public? Do state laws and regulations allow the proposed information exchange? Is surveillance data reliable as a basis for clinical interventions? Can we adequately address security/privacy concerns?
Essential questions: We have the information and the technical ability to inform clinicians about patients in need of care … BUT SHOULD WE? Would this be accepted by patients, providers, and the public? Do state laws and regulations allow the proposed information exchange? Is surveillance data reliable as a basis for clinical interventions? Can we adequately address security/privacy concerns?
 Legitimate public health purposes Respect rights of individuals and communities § Seek input from those to be impacted § Minimize undue burden Privacy and security standards
Legitimate public health purposes Respect rights of individuals and communities § Seek input from those to be impacted § Minimize undue burden Privacy and security standards
 had any") 547 unduplicated HIV patients had their records alerted in system, 447 (82%) had any action taken 46% <35 years of age Mean age 37. 8 years [sd 11. 4], median age 36 years 87% black/African American 38% female 21% had no prior labs in OPH system 41% had no monitoring for > 18 months Mean time out of care 25 months (sd 21. 0, range 0. 2 -109 months, median 19 months)
547 unduplicated HIV patients had their records alerted in system, 447 (82%) had any action taken 46% <35 years of age Mean age 37. 8 years [sd 11. 4], median age 36 years 87% black/African American 38% female 21% had no prior labs in OPH system 41% had no monitoring for > 18 months Mean time out of care 25 months (sd 21. 0, range 0. 2 -109 months, median 19 months)
 Among 84% with a CD 4 following alert Absolute CD 4 mean 282 (sd 235) 42% < 200 Among 79% with a viral load following alert HIV RNA copies/m. L mean 167, 488 66% HIV RNA copies/m. L > 10, 000 (sd 467, 160)
Among 84% with a CD 4 following alert Absolute CD 4 mean 282 (sd 235) 42% < 200 Among 79% with a viral load following alert HIV RNA copies/m. L mean 167, 488 66% HIV RNA copies/m. L > 10, 000 (sd 467, 160)
 Substantial formative and evaluative work with consumers demonstrated acceptability N=24 qualitative interviews of La. PHIE identified patients Acceptable Positive experience of La. PHIE communication Perception that it is a “good system” System helped re-engage in care No negative calls to OPH hotline Provider ease of use, acceptable Source: Qualitative data
Substantial formative and evaluative work with consumers demonstrated acceptability N=24 qualitative interviews of La. PHIE identified patients Acceptable Positive experience of La. PHIE communication Perception that it is a “good system” System helped re-engage in care No negative calls to OPH hotline Provider ease of use, acceptable Source: Qualitative data
 HIV-infected individuals") Using La. PHIE, we were able to: Identify over 989 (thru 3/31/2013) HIV-infected individuals who had been out of care thereby reducing missed opportunities to intervene Offer clinical services to improve individual- and population-level health Determine that system is acceptable to both patients and providers through feedback processes Confirm that a well developed, stakeholder involved process promotes success in implementing novel approaches in addressing linkage and retention.
Using La. PHIE, we were able to: Identify over 989 (thru 3/31/2013) HIV-infected individuals who had been out of care thereby reducing missed opportunities to intervene Offer clinical services to improve individual- and population-level health Determine that system is acceptable to both patients and providers through feedback processes Confirm that a well developed, stakeholder involved process promotes success in implementing novel approaches in addressing linkage and retention.
 Patient and provider acceptance of the interventions Stakeholder engagement Management of public opinion Importance of data validity Importance of engaging legal experts early on Mission/scope/guiding principles and governance % of hits on persons known HIV+ in the LSU system already - and possibility to intervene in absence of HIE
Patient and provider acceptance of the interventions Stakeholder engagement Management of public opinion Importance of data validity Importance of engaging legal experts early on Mission/scope/guiding principles and governance % of hits on persons known HIV+ in the LSU system already - and possibility to intervene in absence of HIE
 Patients OPH HIV, STD and TB programs LSU/TU clinicians OPH Nurses UH Infection Control OPH Epidemiologists Delta Region AETC LSU SPH Medical Informatics & Telemedicine OPH Disease Intervention Specialists OPH Medical Directors DHH Legal Counsel LPHI HCSD CEO, CMO, CIO/CMIO LIS Core Group HCSD Programming Support
Patients OPH HIV, STD and TB programs LSU/TU clinicians OPH Nurses UH Infection Control OPH Epidemiologists Delta Region AETC LSU SPH Medical Informatics & Telemedicine OPH Disease Intervention Specialists OPH Medical Directors DHH Legal Counsel LPHI HCSD CEO, CMO, CIO/CMIO LIS Core Group HCSD Programming Support
 Louisiana DHH OPH STD/HIV Program De. Ann Gruber, Ph. D Administrative Director deann. gruber@la. gov 504 -568 -7474 LSU Health Care Services Division Jane Herwehe, MPH Project Coordinator jherwe@lsuhsc. edu 504 -903 -3089
Louisiana DHH OPH STD/HIV Program De. Ann Gruber, Ph. D Administrative Director deann. gruber@la. gov 504 -568 -7474 LSU Health Care Services Division Jane Herwehe, MPH Project Coordinator jherwe@lsuhsc. edu 504 -903 -3089
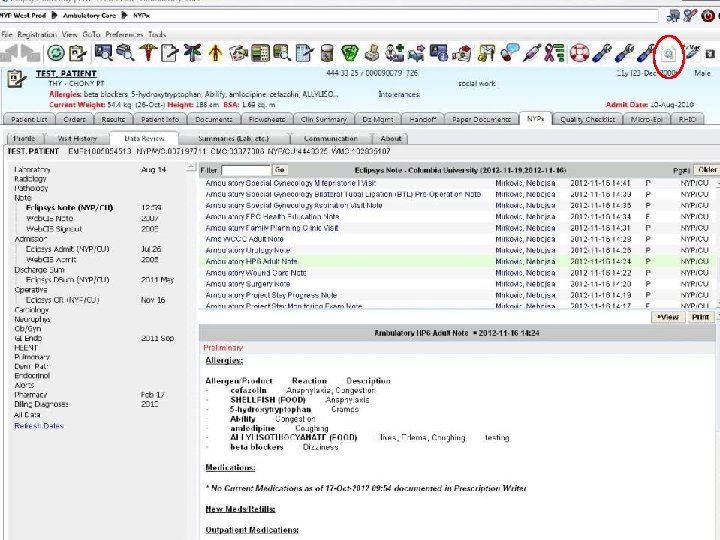
 Using Data and Innovative HIT to In-Reach and Out-Reach to Difficult to Engage Populations Peter Gordon, MD Medical Director, CHP NYP/Columbia
Using Data and Innovative HIT to In-Reach and Out-Reach to Difficult to Engage Populations Peter Gordon, MD Medical Director, CHP NYP/Columbia
 Using Data and Innovative HIT to In-Reach and Out-Reach to Difficult to Engage Populations The Problem: The HIV care cascade illustrates the falloff that occurs between being ‘linked’ and retained in care, and between ‘receiving’ care and adequately suppressed viral loads. Why are we not doing better? Ø We generally have poor tools to effect group or population management ØMultiple IT systems that: • Do not ‘talk’ to each other • Cannot ‘extract’ information easily • Result in ‘shadow’ processes that result in duplicative work ØDivert critical personnel manpower from service provision to data abstraction
Using Data and Innovative HIT to In-Reach and Out-Reach to Difficult to Engage Populations The Problem: The HIV care cascade illustrates the falloff that occurs between being ‘linked’ and retained in care, and between ‘receiving’ care and adequately suppressed viral loads. Why are we not doing better? Ø We generally have poor tools to effect group or population management ØMultiple IT systems that: • Do not ‘talk’ to each other • Cannot ‘extract’ information easily • Result in ‘shadow’ processes that result in duplicative work ØDivert critical personnel manpower from service provision to data abstraction
 The ACA and Health Homes • The Affordable Care Act of 2010 created an optional Medicaid State Plan benefit for states to establish Health Homes to coordinate care for people with Medicaid who have chronic conditions. CMS expects states health home providers to operate under a “whole-person” philosophy. Health Homes providers will integrate and coordinate all primary, acute, behavioral health, and long-term services and supports to treat the whole person. Health Home Services • Comprehensive care management • Care coordination • Health promotion • Comprehensive transitional care/follow -up • Patient & family support • Referral to community & social support services
The ACA and Health Homes • The Affordable Care Act of 2010 created an optional Medicaid State Plan benefit for states to establish Health Homes to coordinate care for people with Medicaid who have chronic conditions. CMS expects states health home providers to operate under a “whole-person” philosophy. Health Homes providers will integrate and coordinate all primary, acute, behavioral health, and long-term services and supports to treat the whole person. Health Home Services • Comprehensive care management • Care coordination • Health promotion • Comprehensive transitional care/follow -up • Patient & family support • Referral to community & social support services
 So how can we use innovative IT tools to harvest, process, and better utilize all of this very important data that we already collect as part of care provision and care coordination activities?
So how can we use innovative IT tools to harvest, process, and better utilize all of this very important data that we already collect as part of care provision and care coordination activities?
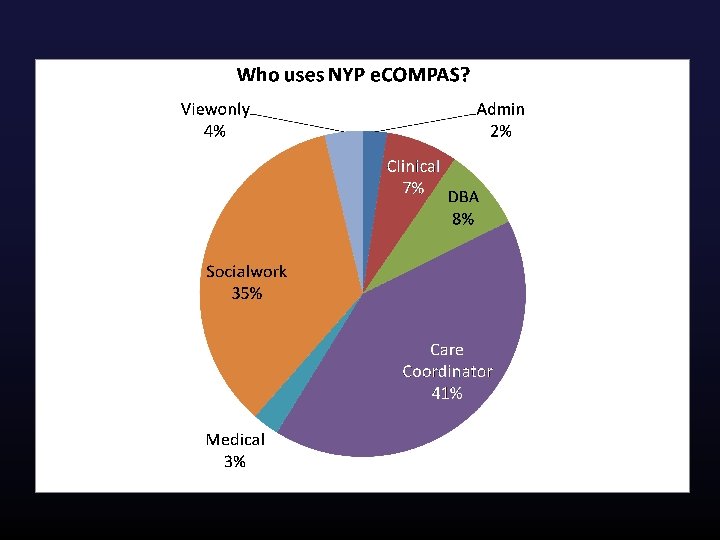
 How much data? Ø NYP/Columbia must track and manage over 800, 000 data elements annually for grant and regulatory reporting purposes: • HRSA, NYC DOHMH, AIDS Institute, CDC • RSR, AIRS, e. SHARE • 95 ‘users’ who need to contribute, add, manage, and export data
How much data? Ø NYP/Columbia must track and manage over 800, 000 data elements annually for grant and regulatory reporting purposes: • HRSA, NYC DOHMH, AIDS Institute, CDC • RSR, AIRS, e. SHARE • 95 ‘users’ who need to contribute, add, manage, and export data
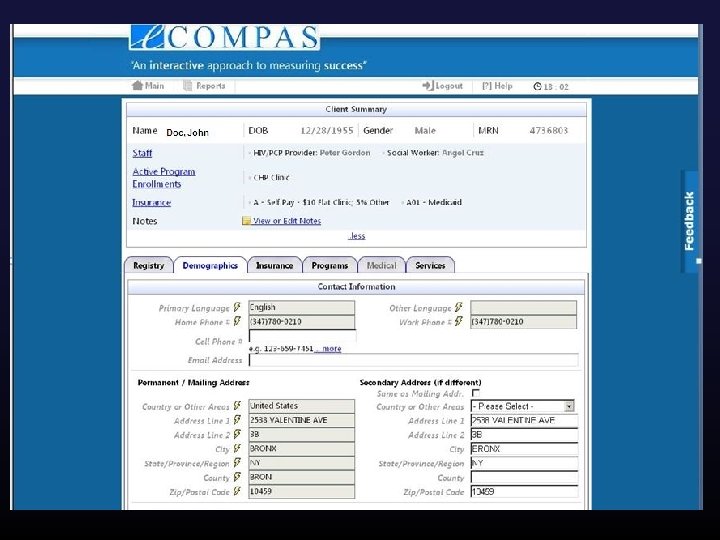
 So one approach is to ‘tap’ into the ‘Medical Record’ , which in many institutions is typically an amalgamation of multiple electronic systems, tied together by an IT network that exchanges information.
So one approach is to ‘tap’ into the ‘Medical Record’ , which in many institutions is typically an amalgamation of multiple electronic systems, tied together by an IT network that exchanges information.
 What is the data? Ø Often duplicative and derived from common sources NYC DOHMH MCM Program RW Part D WICY Program
What is the data? Ø Often duplicative and derived from common sources NYC DOHMH MCM Program RW Part D WICY Program
 So one approach is to find a trusted IT partner, ‘think’ interoperability, and utilize IT tools made available by HRSA and others…
So one approach is to find a trusted IT partner, ‘think’ interoperability, and utilize IT tools made available by HRSA and others…
 To develop an IT system and approach that utilizes the critical individual information already routinely collected and provides tools for group or population management
To develop an IT system and approach that utilizes the critical individual information already routinely collected and provides tools for group or population management
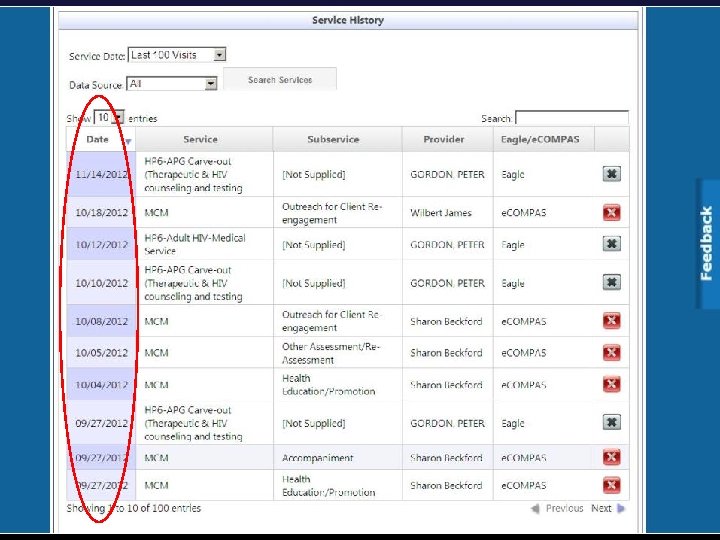
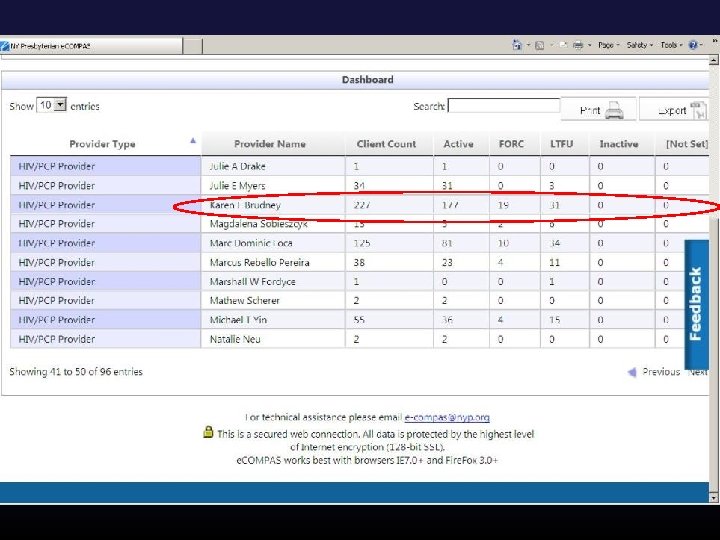
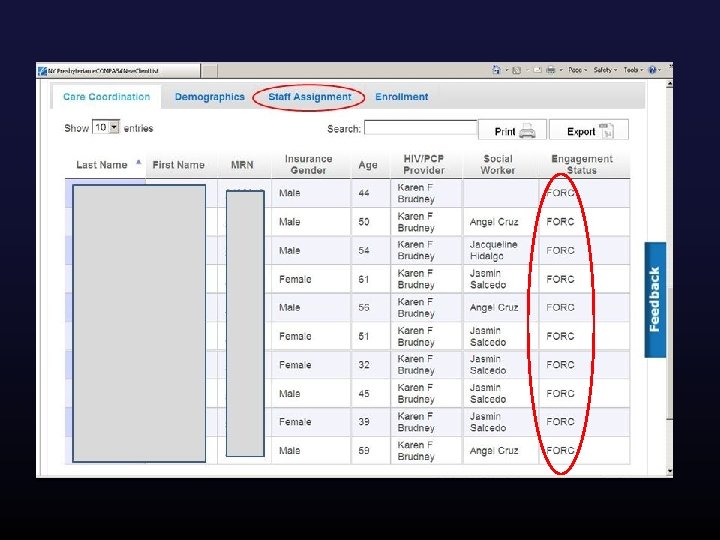
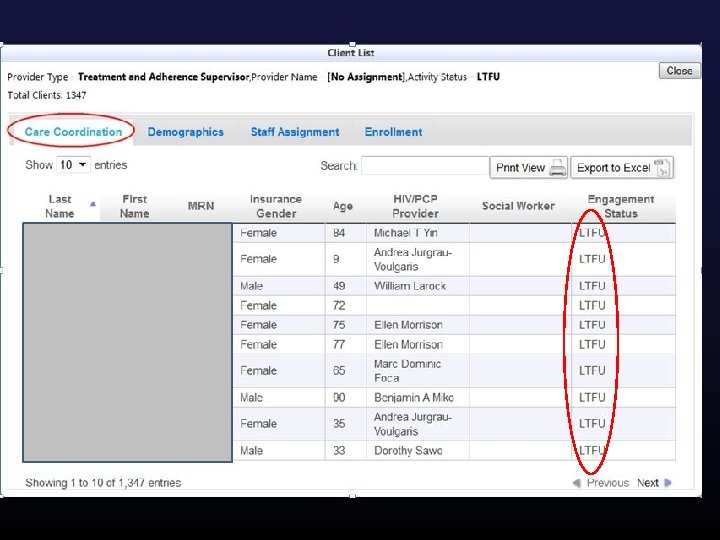
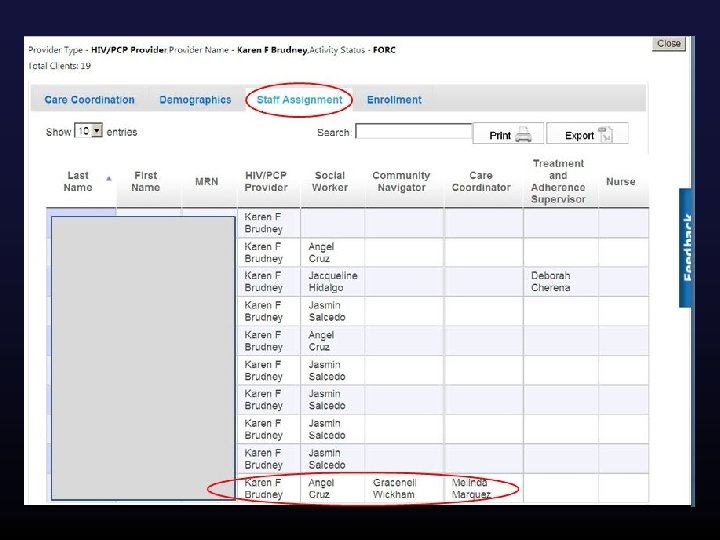
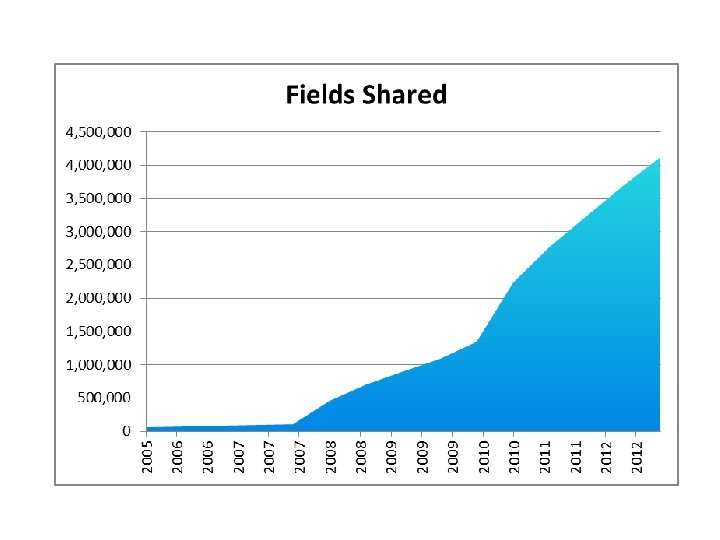
 Once you have the data what can you do with it? Ø Automated data transfer (HIE) § 398, 000 data elements updated/added via HIE since March 2012 (demographics, visits/services, staff assignment) Ø PCP and Care Coordinator Assignment § Calculated from HIE visit feeds, highly accurate, no evolutionary divergence ØCare Engagement and Population Management § Calculated from HIE visit feeds, FORC and LTFU derived, enables care coordination team to generate population level care engagement work lists
Once you have the data what can you do with it? Ø Automated data transfer (HIE) § 398, 000 data elements updated/added via HIE since March 2012 (demographics, visits/services, staff assignment) Ø PCP and Care Coordinator Assignment § Calculated from HIE visit feeds, highly accurate, no evolutionary divergence ØCare Engagement and Population Management § Calculated from HIE visit feeds, FORC and LTFU derived, enables care coordination team to generate population level care engagement work lists
 How much is automated vs. manual?
How much is automated vs. manual?
 Data Feed 2 Data Feed 3 Data Feed 1 e. COMPAS Interface Engine 6. 3 million HL 7 Messages Ø Direct Data Integration 398, 000 Data Elements Automated Data Transformation Engine Master Database 1, 000 est. hours saved each year! Automated Data Transformation Ø PCP and Care Coordinator Assignment Ø Care Engagement and Population Management
Data Feed 2 Data Feed 3 Data Feed 1 e. COMPAS Interface Engine 6. 3 million HL 7 Messages Ø Direct Data Integration 398, 000 Data Elements Automated Data Transformation Engine Master Database 1, 000 est. hours saved each year! Automated Data Transformation Ø PCP and Care Coordinator Assignment Ø Care Engagement and Population Management
 Summary Ø Using innovative HIT tools and approaches can transform a program’s ability to practice group or population management Ø Effective, sustainable program inreach or out-reach efforts require such tools Ø The diffusion of effective HIT tools need to accelerate if the important goals of the NAS and ACA are to be met Ø Find good partners, collaborate, innovate, share
Summary Ø Using innovative HIT tools and approaches can transform a program’s ability to practice group or population management Ø Effective, sustainable program inreach or out-reach efforts require such tools Ø The diffusion of effective HIT tools need to accelerate if the important goals of the NAS and ACA are to be met Ø Find good partners, collaborate, innovate, share
 And special thanks…. . to SPNS! Especially, Adan Cajina Chief, Demonstration and Evaluation Branch
And special thanks…. . to SPNS! Especially, Adan Cajina Chief, Demonstration and Evaluation Branch
 Two Stories of SPNS-Supported In- Reach Innovation 1. SPNS in Hawaii (Part B + Part C) 2. SPNS in New Jersey (Part A) (The very definition of SPNS replication and adaptation working in very different regions!)
Two Stories of SPNS-Supported In- Reach Innovation 1. SPNS in Hawaii (Part B + Part C) 2. SPNS in New Jersey (Part A) (The very definition of SPNS replication and adaptation working in very different regions!)
 Population 1, 288, 198
Population 1, 288, 198
 Network Data Sharing Model • HOPWA • Rent Subsidies • Dr. Visits • CD 4/Viral Load Counts • Other Clinical Indicators Housing ADAP / COBRA • Participation Status • Online Enrollment Medical / Clinical Case Management • Demographic Data • Insurance Data • Ryan White Eligibility
Network Data Sharing Model • HOPWA • Rent Subsidies • Dr. Visits • CD 4/Viral Load Counts • Other Clinical Indicators Housing ADAP / COBRA • Participation Status • Online Enrollment Medical / Clinical Case Management • Demographic Data • Insurance Data • Ryan White Eligibility
 SPNS Helps State Part B via Part C Data Exchange Initiative
SPNS Helps State Part B via Part C Data Exchange Initiative
 Data Sharing Combined with Web-Based Analytical Tools…
Data Sharing Combined with Web-Based Analytical Tools…
 Tools • Visual Analytics
Tools • Visual Analytics
 Outcomes
Outcomes
 “Life Foundation case managers use e 2 for in-reach and engaging hard to reach population by viewing client’s visits to doctors at Spencer Clinic or Waikiki Health Center and lab entry in the service entry sections. ” --HIV Care Services Director
“Life Foundation case managers use e 2 for in-reach and engaging hard to reach population by viewing client’s visits to doctors at Spencer Clinic or Waikiki Health Center and lab entry in the service entry sections. ” --HIV Care Services Director
 Total of 5, 659 Hours Saved by e 2 Hawaii Each Year An additional 2, 000 hours of savings is projected by the Waikiki Health Center based on the e 2 Hawaii Electronic Health Record Data Exchange Module developed by RDE Systems for a total of 5, 659 hours saved per year.
Total of 5, 659 Hours Saved by e 2 Hawaii Each Year An additional 2, 000 hours of savings is projected by the Waikiki Health Center based on the e 2 Hawaii Electronic Health Record Data Exchange Module developed by RDE Systems for a total of 5, 659 hours saved per year.
 Has e 2 Hawaii helped users view clients’ past treatment history before planning and providing services to consumers prior to each visit? e 2 Hawaii vs Reggie - Do you view client's past treatment history before planning and providing services to consumers prior to each visit? 80. 0% 160% Improvement 70. 0% 60. 0% 50. 0% e 2 Hawaii 40. 0% Reggie 30. 0% 20. 0% 10. 0% e 2 Hawaii Reggie
Has e 2 Hawaii helped users view clients’ past treatment history before planning and providing services to consumers prior to each visit? e 2 Hawaii vs Reggie - Do you view client's past treatment history before planning and providing services to consumers prior to each visit? 80. 0% 160% Improvement 70. 0% 60. 0% 50. 0% e 2 Hawaii 40. 0% Reggie 30. 0% 20. 0% 10. 0% e 2 Hawaii Reggie
 “Also, the case managers can also see if clients are accessing Gregory House or Food Baskets in the service entries section. With that information, the case managers are aware that the client is accessing services and… we can follow-up with the providers. ”--HIV Care Services Director
“Also, the case managers can also see if clients are accessing Gregory House or Food Baskets in the service entries section. With that information, the case managers are aware that the client is accessing services and… we can follow-up with the providers. ”--HIV Care Services Director
 City of Paterson Part A: A Case Study in SPNS Innovation Interactive Reports + Data Sharing + Proactive Alerts City of Paterson
City of Paterson Part A: A Case Study in SPNS Innovation Interactive Reports + Data Sharing + Proactive Alerts City of Paterson
 St. Mary’s Hospital PCC Paterson Counseling HUMC Non-SPNS Providers Paterson Testing Bergen County Testing
St. Mary’s Hospital PCC Paterson Counseling HUMC Non-SPNS Providers Paterson Testing Bergen County Testing
 “…we have used the Cross Collaborative reports and RSR to achieve same goal of gathering information in order to send letters/make calls and get persons back in care. ” --Program Coordinator
“…we have used the Cross Collaborative reports and RSR to achieve same goal of gathering information in order to send letters/make calls and get persons back in care. ” --Program Coordinator
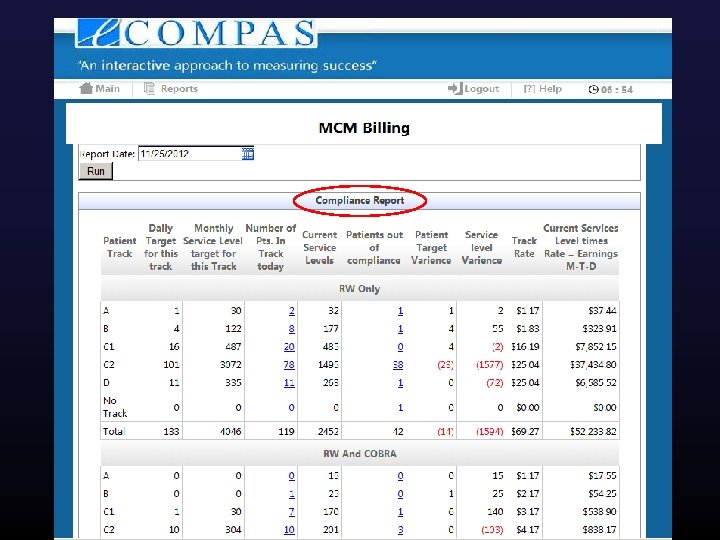
 e. COMPAS Retention Reporting “In regards to retention, we have used the retention tab as a guide to see which patients needed to be sent letters or make calls to remind them to come in for overdue labs, missed appointments. ”– Program Coordinator
e. COMPAS Retention Reporting “In regards to retention, we have used the retention tab as a guide to see which patients needed to be sent letters or make calls to remind them to come in for overdue labs, missed appointments. ”– Program Coordinator
 Outcomes
Outcomes
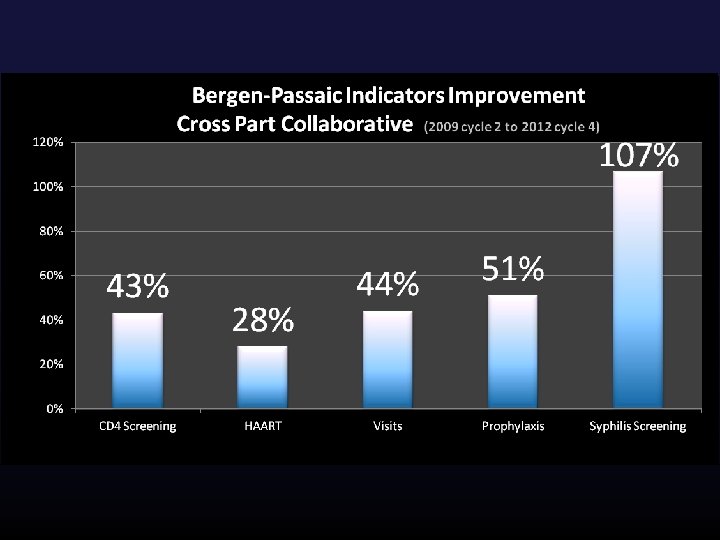
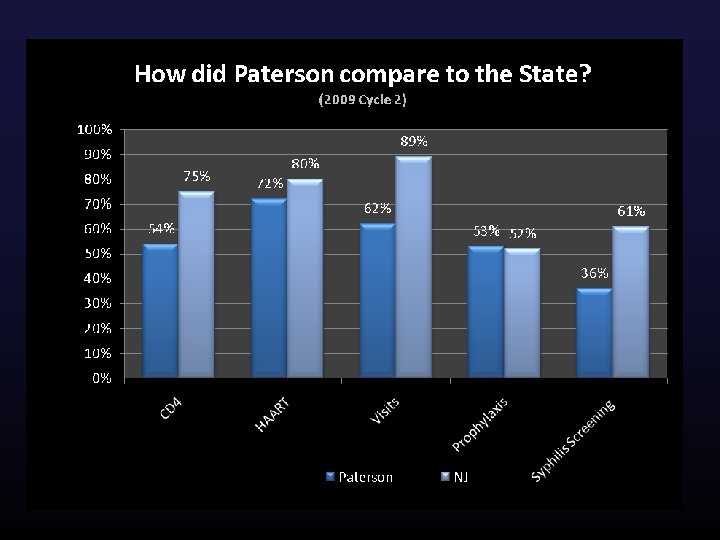
 Comparative Benchmarks Spur Healthy Competition
Comparative Benchmarks Spur Healthy Competition
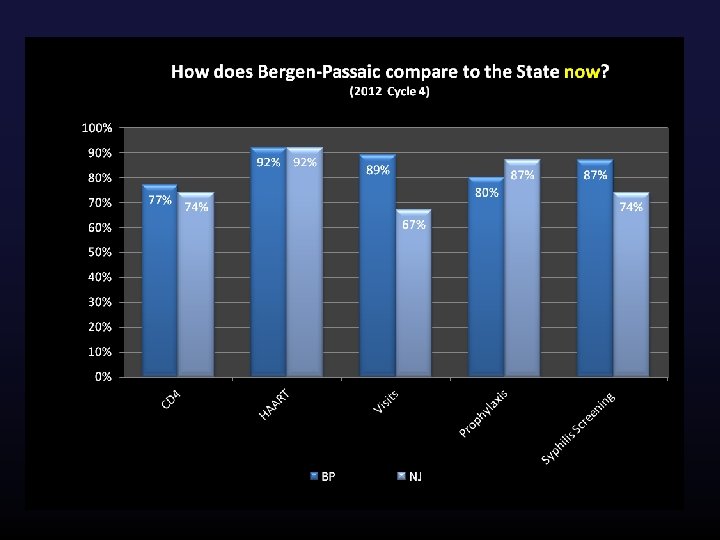
 Statewide Recognition of Bergen-Passaic Providers Bergen-Passaic e. COMPAS SPNS Agencies
Statewide Recognition of Bergen-Passaic Providers Bergen-Passaic e. COMPAS SPNS Agencies
 Launching Now: in+care e. COMPAS Dashboard • • • At-a-glance Visual Red/Green Populations Region vs. Provider • Drilldown
Launching Now: in+care e. COMPAS Dashboard • • • At-a-glance Visual Red/Green Populations Region vs. Provider • Drilldown
 Agency Alerts “We have used the QM tab - summary of current alerts (categories such as Active clients who have not received any services in the past 6 months, missing labs and missed appointment) in order to flag these patients and send reminder letters or make reminder phone calls. We have used the alerts emailed to us to also gather this information and improve retention”-- Program Coordinator
Agency Alerts “We have used the QM tab - summary of current alerts (categories such as Active clients who have not received any services in the past 6 months, missing labs and missed appointment) in order to flag these patients and send reminder letters or make reminder phone calls. We have used the alerts emailed to us to also gather this information and improve retention”-- Program Coordinator
 Agency Alerts Drilldown
Agency Alerts Drilldown
 Email Alerts • Proactive, regular, push notification • Supervisors are more likely to read email
Email Alerts • Proactive, regular, push notification • Supervisors are more likely to read email
 Outcomes
Outcomes
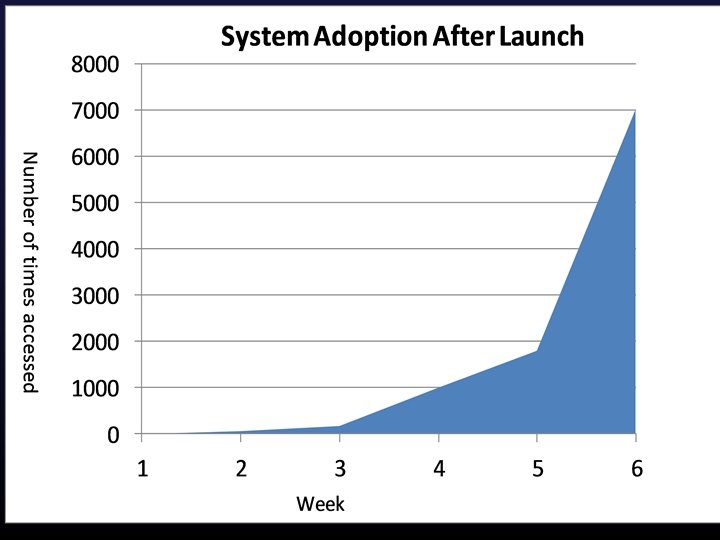
 Usage of Alerts Makes a Difference
Usage of Alerts Makes a Difference
 Data entry + charts SPNS QM + Alerts Undetectable VL improved 38. 6% 2006 -2007 prior to SPNS, all medical patients
Data entry + charts SPNS QM + Alerts Undetectable VL improved 38. 6% 2006 -2007 prior to SPNS, all medical patients
 International Journal of Medical Informatics, October 2012
International Journal of Medical Informatics, October 2012
 Consumers who access their key care information personally… are by definition more engaged in their own healthcare…
Consumers who access their key care information personally… are by definition more engaged in their own healthcare…
 With My. Health. Profile. . . …you can securely access your health information on-the-go …on any device, anywhere. © 2013 RDE Systems LLC. All rights reserved.
With My. Health. Profile. . . …you can securely access your health information on-the-go …on any device, anywhere. © 2013 RDE Systems LLC. All rights reserved.
 Care Information. All of your critical medical history is just one click away Comprehensive summary designed to help you understand your medical information without feeling overwhelmed © 2013 RDE Systems LLC. All rights reserved.
Care Information. All of your critical medical history is just one click away Comprehensive summary designed to help you understand your medical information without feeling overwhelmed © 2013 RDE Systems LLC. All rights reserved.
 Alerts & Reminders. Never miss an appointment again, with the easy to use To-Do list. Alerts help you better manage your health © 2013 RDE Systems LLC. All rights reserved.
Alerts & Reminders. Never miss an appointment again, with the easy to use To-Do list. Alerts help you better manage your health © 2013 RDE Systems LLC. All rights reserved.
 Emergency Cards. With My. Health. Profile, you can easily create and print temporary emergency cards, so that your …so that your information can be accessed when you need it the most. Peter Gordon, MD New. York-Presbyterian / Columbia University Medical Center © 2013 RDE Systems LLC. All rights reserved.
Emergency Cards. With My. Health. Profile, you can easily create and print temporary emergency cards, so that your …so that your information can be accessed when you need it the most. Peter Gordon, MD New. York-Presbyterian / Columbia University Medical Center © 2013 RDE Systems LLC. All rights reserved.
 Critical Success Factors v Involvement v Responsive and User-friendly Platform v Organic process v Collaboration The platform and culture facilitates continuous quality improvement through a direct relation between the system, the process and the people.
Critical Success Factors v Involvement v Responsive and User-friendly Platform v Organic process v Collaboration The platform and culture facilitates continuous quality improvement through a direct relation between the system, the process and the people.
 Process over Product Leadership People Process Technology
Process over Product Leadership People Process Technology
 Thank you from all of us on the Paterson SPNS Team… (from left to right) Denise Coba, Pat Virga, Jesse Thomas, Millie Izquierdo, Jimease Green, Maria Cordova, Doug Mendez, Pricilla Moschella, Jerry Dillard, Ellen Mc. Namara, Larry Rodgers, Blanca Roman, Anthony Fazzinga, Sandra Murillo, Maryann Collins, Irene Panagiotis, Serge Virodov, Chantia Douglas, Kathy Lebron.
Thank you from all of us on the Paterson SPNS Team… (from left to right) Denise Coba, Pat Virga, Jesse Thomas, Millie Izquierdo, Jimease Green, Maria Cordova, Doug Mendez, Pricilla Moschella, Jerry Dillard, Ellen Mc. Namara, Larry Rodgers, Blanca Roman, Anthony Fazzinga, Sandra Murillo, Maryann Collins, Irene Panagiotis, Serge Virodov, Chantia Douglas, Kathy Lebron.
 Q&A To be informed when these upcoming IHIP resources are ready, keep an eye out for HRSA announcements or sign up for the IMC newsletter email scook@impactmc. net. Connect with Us Sarah Cook-Raymond, Managing Director |Impact Marketing + Communications | Twitter: @impactmc 1| Facebook: Impact. Mar. Com |www. impactmc. net | 202 -588 -0300
Q&A To be informed when these upcoming IHIP resources are ready, keep an eye out for HRSA announcements or sign up for the IMC newsletter email scook@impactmc. net. Connect with Us Sarah Cook-Raymond, Managing Director |Impact Marketing + Communications | Twitter: @impactmc 1| Facebook: Impact. Mar. Com |www. impactmc. net | 202 -588 -0300