endometriosis and adenomyosis interns.pptx
- Количество слайдов: 37



ENDOMETRIOSIS & ADENOMYOSIS Dr. OMAR ALDABBAS ASSISTANT PROF. MUTA UNIVERSITY

v Endometriosis: the presence of tissue, Definitions histologically similar to endometrium, outside the uterine cavity. v. The eutopic endometrium is the normally situated endometrium inside the uterus in the presence of ectopic endometrium. v. The ectopic endometrium.

The normal endometrium • Endometrial myometrail inreface basal layer functional layer • Basal layer: Regneration Area from the ednothelial surface to the basal layer <300 mcm

Definitions The basal layer: defined as lying less than 300 µm above the endometrialmyometrial interface (EMI). The functional layer of endometrium defined as the area from the epithelial surface to the basal layer. The endometrial-myometrial interface: the boundary between endometrium and myometrium. It lacks a basement membrane. n n n Endometirum is a unique tissue. In other tissues, there is a basement membrane. Any tissue to bleed 6 days a month and heal rapidly is a unique tissue!!! They drink the menstrual blood in some tribes in north Iraq and some islands in the a. Pacific. This shows the importance of the uterus. . . Ya 3333

• • 1 ST STAGE: increased angiogenesis Ectopic endometrium: behaves like a cancer but is n ot a cacner

• Adhesions:

Superficial Deeply infiltrating Ovarian: Chocolate cyst – Bleeding endometriosis in the ovary

• All are superficial endometriosis • Bladder: beside it is a large cyst. Endometrioma • Any –oma means a swelling:

• • • Commonest sites for endometriosis: the ovary> Cul-de-sac> Uterosacral ligament Next common diagnosis: IBS Cul-de-sac: Syn: rectouterine pouch. [Fr. bottom of a sack] = Pouch of Douglas

PREVALENCE NOT PRECISELY KNOWN— 2 -5% 20 -40% OF WOMEN IN INFERTILE COUPLE RELATIONSHIPS VS 5% OF FERTILE WOMEN BUT ALSO FOUND IN 6 -43% OF WOMEN UNDERGOING LAPAROSCOPIC STERILIZATION =silent 52% OF TEENAGES WITH CPP (Chronic pelvic pain) SYNDROME

Familial association Eight-fold increase risk if close relative Risk to sibs if severe endometriosis– 15 n Source: Oxygen study

Risk factors ﺳﺆﺎﻝ ﺩﺍﺋﻢ Single/ nulliparous: The best treatment is getting pregnant. Early menarche: because it is estrogen dependent disease Non-oral contraception Non-smoker shorter cycle longer duration of flow [Why smoking is protective? Because it works as anti-estrogen].

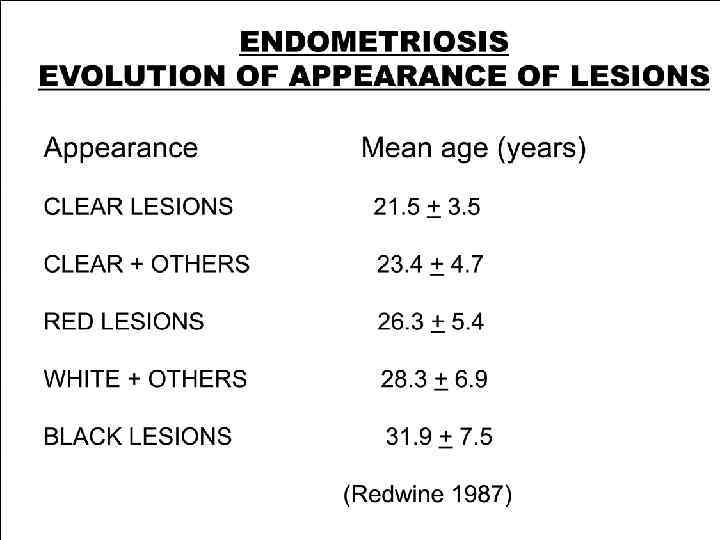
Endometriosis is a progressive disease Disease will progress in 23– 64% of women without therapy and in approximately 20% of women with therapy (Kauppila, 1993; Farquhar /Sutton, 1998). Ectopic lesions appearance & progressiveness of the disease. (Redwine, 1987).

Delay in diagnosis • In average 6 -7 years. Why? • • Normalization of symptoms It is 8 X more if you have a first-degree relative with it, she consults her mother, “I had it for years”. • This delay is longest among young age group. • Factors: • • • Doctors. Families. Diagnostic means: • • US: Ovarian MRI: Bowel CA-125: Does not work as a follow-up Laparascopy: Operator-dependent

Diagnostic tools Laparoscopy: The Gold standard Clinical examination: n n n Tenderness in vaginal wall Non moveable uterus Palpable ovaries = Endometrioma Serum markers: n CA 125 - not diagnostic, helpful in follow up n Proteomics n Cytokines: IL-6, IL 7, they studay many of them!!! Endometrial markers: endometrial nerve fibres (Al-Jefout et al, 2007, 2009) n top 10 discoveries in gynecoloigy in the past 10 years Imaging: n TVU- only for endometriomas n MRI- for deep and bowel endometriosis n Multi slice CT scan- for bowel endometriosis

Presentation Pain: n n n Dysmenorrhoea. Deep Dyspareunia. Chronic pelvic pain. Dyschesia Dysuria Infertility: n n There is association between infertility and endometriosis but there is no causal relationship Smoking and lung cancer: association but not causal relationship. If it is a causal relationship, then this means that every one who smoke will get lung cancer; but this is not the case!!! Others

Variability of endometriosis presentation High levels of variability in: n n n n Age of onset of symptoms Constellation of presenting symptoms Types and severity of pain Site and extent of pathology Coexistence of other pathologies: With PCOS and adenomyosis Response to treatment: One responds to aspirin, another needs three types of progesterone. The goal of treatment is to relieve symptoms. Rate of recurrence of symptoms and disease

Clinical endometriosis: a highly variable symptom complex (Markham et al, endometriosis cases: n = 529; controls: n = 208) Pain (92%); no pain (6– 8%) Extreme lethargy (97%) Gastrointestinal symptoms (96%) Urinary tract symptoms (44%) Low resistance to infection (43%) Low grade fever (42%) Increased predisposition to autoimmune conditions Genital tract bleeding: heavy menstrual bleeding (65%); premenstrual spotting (63%)

Pain is the Central Challenge! Pelvic pain is universally recognized as the key symptom in endometriosis. It is the primary reason why the patient consults her doctor. Some will have infertility + pain. Restriction to common triad of dysmenorrhoea, deep dyspareunia and pain with a bowel motion by GPs or some Gynaecologists.
")
Only diagnostic method is laparascopy with histopatholgoy (to show endometrial glands)
. In addition to")
Treatment principle objective Is symptom-relief management (Chwalisz et al. , 2002). In addition to relieving pain, the goals of treatment for patients with endometriosis are to: n n prevent or delay disease progression by reducing endometriotic implants through surgical treatment or medically induced atrophy of the implants (Rice, 2002; Valle et al. , 2003).

Infertility mechanisms Adhesions Increased PGs Cell mediated gamete inj Defective folliculogenisis Chronic salpingitis Activated macrophag Increased prev. ABs LUFFS (Luteinized Unrupturef) Altered tubal motility Cytokines Fertilization failure hyperprolactinae mia Impaired oocyte pick up Sperm phagocytosed Early spon abortion Luteal phase deficiency Now, the best treatment: Surgical management + IVF
")
FIRST – A FEW QUESTIONS! IS TREATMENT ALWAYS REQUIRED? WHO NEEDS TREATMENT? Pain (symptomatic) and infertile DOES ANY TREATMENT REALLY WORK? We still try DOES TREATMENT IN YOUNG WOMEN PREVENT INFERTILITY AND PROGRESSION? yes

Surgical Rx Ablation: laser, cauterisation Excision. Stripping of endometrioma. ﺑﻘﺸﺮ Conservative Extensive. ﺑﺸﻴﻞ ﺍﻟﺠﻤﻞ ﺑﻤﺎ ﺣﻤﻞ Other organs involvement: n Bowel resection: segmental or disc resection
 Because neither medical nor surgical treatments")
Medical Vs Surgical treatment (Al-Jefout et al, 2010) Because neither medical nor surgical treatments have been proven to improve fertility rates substantially in women with endometriosis in its early stages, the focus of treatment is on the relief of pain symptoms (Shaw, 2003). Long-term or repeated courses of medical therapy are required to control these symptoms (Schweppe, 2001). Surgery is an invasive therapeutic option that is far from ideal, because 20% of cases do not respond (Abbott et al. , 2004). The recurrence rate is still high after surgery (Milingos et al. , 2003).

META-ANALYSIS MIN/MILD ENDOMETRIOSIS PREG RATE NO TREAT 44% DRUG THERAPY SURGERY IVF n 235 FOLLOWUP 0. 5 -3 41% 418 1 - 5 65% 912 1 -6 20 257

Recurrence of symptoms after surgery RCTs reported that 51% of women experienced a recurrence of symptoms sufficient to require additional medication for pain within 1 year of surgery (Hornstein et al. , 1997). Other reports have indicated that 40 -50% of patients experience recurrence of pain symptoms within 5 years (Valle et al. , 2003). Studies of laser surgical treatment also suggest increasing recurrence of symptoms with time (e. g. recurrence occurred in 23% of patients at 1 year and 31% of patients at 2 years in one study cohort of 106 patients (Shaw, 2003).

General considerations. No correlation bet’n disease severity and symptoms Age of the patient, Patient’s needs. complete amennorhic ﻭﺣﺪﺓ ﺑﺪﻫﺎ ﺗﺤﻤﻞ ﻣﺎ ﺑﺼﻴﺮ ﺗﻜﻮﻥ Extent of disease, Duration of the infertility, Severity of symptoms. The patient's reproductive plans should also be taken into account. Correct diagnosis

Conclusions Medical treatment for endometriosis is mainly for pain symptoms. All hormonal drugs studied are equally effective, although their side-effects and cost profiles differ. Medical treatment for infertility purposes has no benefit or may even delay pregnancy, ‘more harm than good can be done by drug treatment, because of side effects and the lost opportunity to conceive’. so surgery +ivf is the best It seems to be that a combined medical and conservative surgical approach is beneficial for most women with endometriosis associated pelvic pain.

Adenomyosis

Definition • Adenomyosis is a benign disease of the uterus characterized by ectopic endometrial glands and stroma within the myometrium more than 2 cm from EMI (endometrial myometrail interface) • It is associated with myometrial hypertrophy and may be either diffuse or focal.
. • Both")
Definition • Adenomyoma describes a focus of adenomyosis within a leiomyoma (fibroid). • Both conditions are common so it is not surprising that this overlap condition may occur.

The typical symptoms include Pelvic pain, Dysmenorrhoea, And menorrhagia unresponsive to hormonal therapy or uterine curettage. Subfertility and pregnancy termination.

Pelvic pain In studies of chronic pelvic pain in which women had hysterectomies, the incidence of adenomyosis is about 15% to 25%

Diagnosis • The diagnosis can only be proven by the • • pathologists: Histopathology Clinical exmination: The uterus is bulky; either diffusely or nodularly (symmetrical and assymetrical): Tender Biopsy MRI TVU

MANEGMENT The only definitive treatment for adenomyosis is total hysterectomy, with or without ovarian conservation.
endometriosis and adenomyosis interns.pptx