5b93f897c50a8b768ad0ce9bca55ec1a.ppt
- Количество слайдов: 31



encephalitis Dr. Ibrahim Khasraw Jaf Department of Pediatrics School of Medicine Sulaymani University

Definition : It is inflammatory process of the brain parenchyma , mainly caused by special types of viruses , leading to mortality and morbidity among children due to cerebral dysfunction.

Classification : According to the onset ; Acute: abrupt onset with rapidly developing clinical features , e. g. : enteroviruse , herpes simplex virus encephalitis. Subacute: slower developing symptoms within days to few weeks , e. g. : measles , HIV. Chronic: develop over long period(months) , e. g. : S. S. P. E. , T. B. .
 : According to anatomical site of involvement ; Focal: when")
Classification (continue. . ) : According to anatomical site of involvement ; Focal: when one or more points of the brain lobes involved like , temporal , parietal lobes of the brain , limbic system. Diffuse: (generalized) when whole brain tissues involved.
 : According to pathological process ; Direct: when the infective")
Classification (continue. . ) : According to pathological process ; Direct: when the infective agent itself invade the brain and induce inflammation. Indirect (post infectious) : when the infectious agent , after cure induce immune mediated inflammatory reaction in the brain due to antibody-antigen reaction , e. g. : post , chickenpox crebellitis.

Etiology : Viral : includes these viruses according to the incidence. Enteroviruses : about 50% of cases due to these groups of viruses , e. g. : coxachi & echo viruses (non polio viruses). Herpes virus group : about 10 -20% of cases (herpes simplex virus , Epstein-Barr virus , cytomegalovirus , varicella zoster virus , human herpes viruse 6, 7 ).
 : Other viruses : may be caused by viruses which")
Etiology (continue. . ) : Other viruses : may be caused by viruses which cause systemic diseases rarely as a part of complication they cause encephalitis like influenza virus , measles , mumps , rubella (german measles) , rabies , HIV. Nonviral causes : (mainly bacteria) : like mycoplasma , rickettsia , fungi , parasites , mychobacterium(T. B. ) , collagen tissue , e. g. : S. L. E. . 1/3 rd of cases still no cause could be found.
. - Prodromal phase")
Clinical features : - The onset is sudden or insidious (gradual). - Prodromal phase usually starts with flue-like illness with cough , sore throat , fever. - Headache , nausea , vomiting , blurring of vision , papillodema (due to increase intra cranial pressure). - Disturbance of consciousness , from lethargy to deep coma , covulsion. - Focal neurological signs : according to area involved. - Skin rash & conjunctivitis in special types.

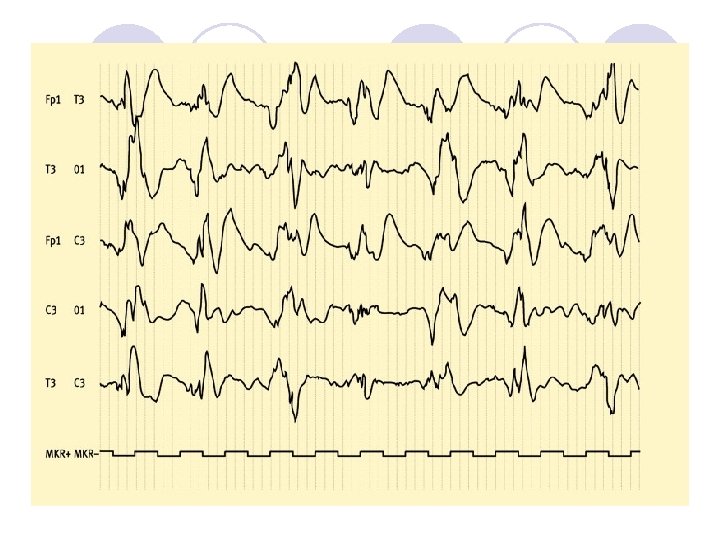
Diagnosis : - - C. S. F. : show lymphocytic pleocytosis , slight increase in protein with normal sugar (only decreased in mumps encephalitis) occasionally may be normal. Very high protein with very low sugar suggestive of tuberculus infection (e. g. : tuberculoma ). - E. E. G. : show diffuse slow wave , focal changes e. g. : temporal lobe abnormal finding highly suggestive of herpes simplex virus.
 : - Neuro imaging : C. T. scan , M.")
Diagnosis (continue. . ) : - Neuro imaging : C. T. scan , M. R. I. may be normal but may show focal lesion according to the site involved or may show diffuse brain swelling. Temporal lobe lesion suggestive of herpes simplex virus(H. S. V. ). - Serology : antibody-antigen reaction test rising of titer against special virus like H. S. V. 4 fold or Igm type significant.
 : - Viral culture of C. S. F. , urine")
Diagnosis (continue. . ) : - Viral culture of C. S. F. , urine , stool , nasopharyngeal swab commonly reveal the virus. - P. C. R. : it is identify the virus through its DNA , it is highly specific and sensitive for C. S. F. , nowadays replaced the brain biopsy. - Brain biopsy : the last and invasive procedure rarely done for special types like T. B. & non infectious causes
. - Hypoglycemia. - Collagen")
Differential diagnosis : - - Reye syndrome(aform of hepatic encephalopathy). - Hypoglycemia. - Collagen vascular disease (C. V. A. ). - Drugs & toxins. - Hypertensive encephalopathy.

Treatment : - Non specific : measures to be taken like admission to I. C. U. then A, B, C, D. Control convulsions by phenobarbiton. Decrease intra cranial pressure by dexametasone and or mannitol. Pay attention to fluid & electrolytes.
 : Specific : intra venous acyclovir for H. S. V")
Treatment (continue. . ) : Specific : intra venous acyclovir for H. S. V , V. Z. V. they are only viruses susceptible to drug therapy , otherwise there is no specific treatment for other viral encephalitis. Antibiotics for bacterial causes , e. g. : mycoplasma (erythromycin) , T. B. (anti T. B. ). Others according to the cause , e. g. steroid for S. L. E. .

Complication : Happen when there was no recovery within 2 -3 weeks and they are common in spite of proper treatment like ; - Death : generally occur in about 5% of cases. - Paresis , spasticity , ataxia. - Cognitive impairment. - Epilepsy due to recurrent seizures.

Prevention : Only two viral forms of encephalitis could be prevented by vaccination against them , they are influenza virus and rabies virus vaccines done for whom they are liable to get them.

Figure : EBV encephalitis. a Axial FLAIR image demonstrates abnormal T 2 -W signal in the bilateral frontal cortex and subcortical white matter. This is a typical pattern for viral encephalitis. The multiple vascular territories involved make ischemia unlikely. Additionally, a child presenting with multifocal strokes of this magnitude would have a profound clinical presentation with fixed neurologic deficits. b, c Axial (b) and coronal (c) FLAIR images demonstrate increased signal in the bilateral basal ganglia reflecting the unique tropism of EBV for this area

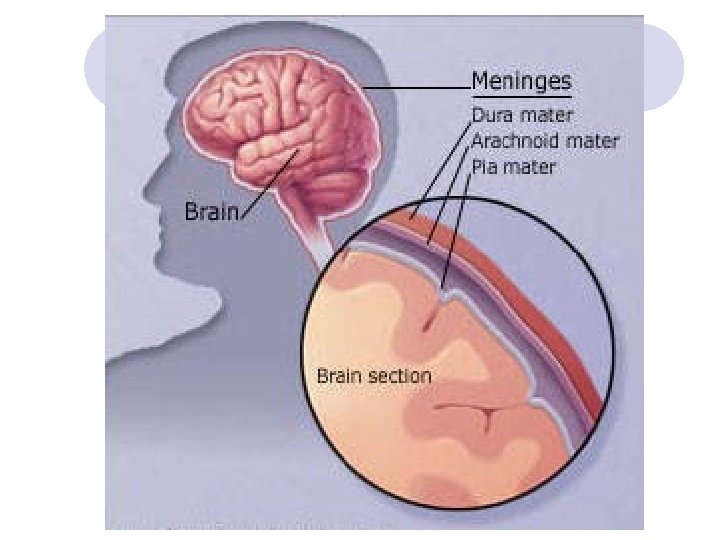
Meningitis: Definition : It’s inflammation of leptomeninges caused by pathogenic microorganisms: Bacteria: -strept. pneumoniae , H. infleunzae , meningococus Viruses: - H. S. V, H. I. V, C. M. V, Mumps, enterovirus, HLCM. Fungi: -coccidiomycosis, Histoplasmosis, Uncommon: -Lyme disease , catscratch dis. , T. B. , Toxoplasmosis, Entameba: Acanthomeba
meningitis: Bacteriology: - Strept. pn. , nowadays commonest one - H. infleunzae,")
: Acute bacterial(septic)meningitis: Bacteriology: - Strept. pn. , nowadays commonest one - H. infleunzae, about 5% of cases(b. of vaccination. ) - Meningococcus (Niserea meningitidis). rare but most serious and Weakest bacterium. - Staph. aureas, common in post-surgical cases&penetrated wounds. - Pneunococcus: in fracture base of skull &C. S. F leak

Clinical features: *It’s variable according to the age of the patient: -Neonates and infants: *Fever or hypothermia, drowsiness' or irritability *Tense anterior fontanel, convulsion, unexplained *Repeated vomitting, lethargy, relactant to feed. -Older aged children: *headache , repeated vomiting , meningisim , toxicity (neck stiffness , kerning&brudzinesky signs. )
")
C. F. continue: Skin rash in form of purpura , called purpura Fulminance(in meningococcemia) Adrenal hemorrhag: shock state called (water house fridrichsen syndrom) -Signs of increase intracranial pressure (hypertention, bradycardia , irregular respiration). -Focal nearological signs: ptosis , 6 th N. pulsy, anisocoria Usually there's no papilodema.

Diagnosis: - C. B. P. : Shows neutrophil leukocytosis, with picture ofacute bacterial inf. - Positive acute phase reactants: high E. S. R. , +Ve C. R. P - Blood culture &sensitivity may be +ve in about 90% of cases. - L. P for C. S. F. examination: us. show increase preasure, cell count, (majority are neutrophils), protein, &decrease sugar, coloure may be turbid. - Signs of consumptive coageolopathy. or D. I. C. in meningococcemia.

Contraindications of L. P. : *Cardiopulmonary instability *Infection in the site of L. P. * Bleeding tendency. *Papillodema. ( absolute C. I. )

Normal C. S. F. parameter: *Colure : clear *pressure: <160 mm. H 2 O *Cell count: 0 -5 Lymphocytes, No Neutrophils *Protein: 15 -35 mg/dl *Sugar: 50 -80 mg/dl(or 2/3 rd of blood sugar) *Culture: -ve. But normal C. S. F. doesn't exclude meningitis.

D. Dx: *Encephalitis *Intracranial hemorrhage. *Encephalopathy. *Posterior fossa tumore.

Treatment: -Its one of ped. Top medical emergensy. -Admission to hospital &in special isolated word. -Control convulsion. -Give I. V. fluid 2/3 red of the daily requirement(to pre -vent S. I. A. D. H). -biotics : Empirical choice is combination of vancomycine +one of third genration cephalosporins (cefotaxime or ceftriaxon) double of the simple dose. - -Steroid: Dexamethasone twice daily for two days.

Comlications: *Early : Sub-dural effusion, Hydrocephalus, c. v. a. Cerebral herniaition , D. I. C, Adrenl hemorrhage (water-house fridrichsen syndrome) *Late : cerebral abscess , cerebral pulsy, mental retardation, epilepsy, deafness, blindness.

Prevention: *Meningococcal vaccine for overcrowded areas al vaccine: for Immune mpromised children. *Chemoprophylaxis. : Rifampicin 10 mg/kg/dos 2 hourly for 2 days for contacts with meningoco- Ccemia. &10 mg/kg/day single dose for 4 days in H. infl. -single inj. Of ceftriaxon , oral ciprofloxacine are Ulternatives.

HE END THANKS
5b93f897c50a8b768ad0ce9bca55ec1a.ppt