

f42e5013b638dc537792fbdbd3f0c81d.ppt
- Количество слайдов: 117
 Emergency Preparedness Standards for Medicare and Medicaid Participating Providers and Suppliers Kenneth Daily, LNHA, President Elder Care Systems Group kenn@qissurvey. com SD Health Care Association September 2017
Emergency Preparedness Standards for Medicare and Medicaid Participating Providers and Suppliers Kenneth Daily, LNHA, President Elder Care Systems Group kenn@qissurvey. com SD Health Care Association September 2017
 CMS EMERGENCY RULE CMS Actions • On September 2016 CMS released FINAL disaster rule, Emergency Preparedness Standards for Medicare and Medicaid Participating Providers and Suppliers • Providers have one-year to comply and the requirements will be enforced effective beginning November ‘ 17
CMS EMERGENCY RULE CMS Actions • On September 2016 CMS released FINAL disaster rule, Emergency Preparedness Standards for Medicare and Medicaid Participating Providers and Suppliers • Providers have one-year to comply and the requirements will be enforced effective beginning November ‘ 17
 CMS Emergency Preparedness Regulation
CMS Emergency Preparedness Regulation
 “Disaster” Definition • Disaster- dis·as·ter n. a. An occurrence causing widespread destruction and distress; a catastrophe. b. A grave misfortune. c. Informal- A total failure • An emergency becomes a disaster when need exceeds resources! Disaster = Need > Resources Notice that this definition does not specifically deal with medical needs…it may address any category of needs…
“Disaster” Definition • Disaster- dis·as·ter n. a. An occurrence causing widespread destruction and distress; a catastrophe. b. A grave misfortune. c. Informal- A total failure • An emergency becomes a disaster when need exceeds resources! Disaster = Need > Resources Notice that this definition does not specifically deal with medical needs…it may address any category of needs…
 What Are We Preparing For? • Possible hazards for Long Term Care facilities • Natural hazards • Manmade/technological hazards
What Are We Preparing For? • Possible hazards for Long Term Care facilities • Natural hazards • Manmade/technological hazards
 • SNFs serve the medically fragile • Elderly frequently more impacted by disasters • Emergency plans are often outdated • Lack of participation with EMA and community preparedness coalitions • Sheltering-in-place concept critical • Evacuations are very difficult and based upon nature and impact of threat, plus acuity of residents • Lacking tracking systems • Limited security management plan in place Long Term Care Challenge
• SNFs serve the medically fragile • Elderly frequently more impacted by disasters • Emergency plans are often outdated • Lack of participation with EMA and community preparedness coalitions • Sheltering-in-place concept critical • Evacuations are very difficult and based upon nature and impact of threat, plus acuity of residents • Lacking tracking systems • Limited security management plan in place Long Term Care Challenge
 Appendix Z • Because the individual regulations for each specific provider and supplier share a majority of standard provisions, we have developed this Appendix Z to provide consistent interpretive guidance and survey procedures located in a single document • Unless otherwise indicated, the general use of the terms “facility” or “facilities” in this Appendix refers to all provider and suppliers addressed in the Final Rule and in this appendix. Additionally, the term “resident(s)” within this appendix includes residents, residents and clients unless otherwise stated.
Appendix Z • Because the individual regulations for each specific provider and supplier share a majority of standard provisions, we have developed this Appendix Z to provide consistent interpretive guidance and survey procedures located in a single document • Unless otherwise indicated, the general use of the terms “facility” or “facilities” in this Appendix refers to all provider and suppliers addressed in the Final Rule and in this appendix. Additionally, the term “resident(s)” within this appendix includes residents, residents and clients unless otherwise stated.
 follow the standard survey protocols") Survey Protocol • These Conditions of Participation (Co. P) follow the standard survey protocols currently in place and will be assessed during initial, revalidation, recertification and complaint surveys as appropriate. Compliance with the Emergency Preparedness requirements will be determined in conjunction with the existing survey process for health and safety compliance surveys or Life Safety Code (LSC) surveys. • There are 43 surveyor guidelines of which 26 apply to skilled nursing centers.
Survey Protocol • These Conditions of Participation (Co. P) follow the standard survey protocols currently in place and will be assessed during initial, revalidation, recertification and complaint surveys as appropriate. Compliance with the Emergency Preparedness requirements will be determined in conjunction with the existing survey process for health and safety compliance surveys or Life Safety Code (LSC) surveys. • There are 43 surveyor guidelines of which 26 apply to skilled nursing centers.
 Interpretative Guidelines E-001 Emergency Preparedness Program • Under this condition/requirement, facilities are required to develop an emergency preparedness program that meets all of the standards specified within the condition/requirement. • The emergency preparedness program must describe a facility's comprehensive approach to meeting the health, safety, and security needs of their staff and resident population during an emergency or disaster situation. • The program must also address how the facility would coordinate with other healthcare facilities, as well as the whole community during an emergency or disaster (natural, manmade, facility). • The emergency preparedness program must be reviewed annually.
Interpretative Guidelines E-001 Emergency Preparedness Program • Under this condition/requirement, facilities are required to develop an emergency preparedness program that meets all of the standards specified within the condition/requirement. • The emergency preparedness program must describe a facility's comprehensive approach to meeting the health, safety, and security needs of their staff and resident population during an emergency or disaster situation. • The program must also address how the facility would coordinate with other healthcare facilities, as well as the whole community during an emergency or disaster (natural, manmade, facility). • The emergency preparedness program must be reviewed annually.
 E-001 Survey Procedures • Interview the facility leadership and ask him/her/them to describe the facility’s emergency preparedness program. • Review the facility’s written policy and documentation on the emergency preparedness program.
E-001 Survey Procedures • Interview the facility leadership and ask him/her/them to describe the facility’s emergency preparedness program. • Review the facility’s written policy and documentation on the emergency preparedness program.
 Policies Recommended • Program Overview including commitment to addressing situations based on threat to resident population and facility • All hazards approach to emergency preparedness • Communications structure to respond effectively
Policies Recommended • Program Overview including commitment to addressing situations based on threat to resident population and facility • All hazards approach to emergency preparedness • Communications structure to respond effectively
 Interpretative Guidelines E-003 Emergency Preparedness Plan – Review • Facility must comply with all applicable Federal, State and local emergency preparedness requirements. • Facility must develop establish and maintain a comprehensive emergency preparedness program that meets the requirements of this section. • The emergency preparedness program must include: Emergency Plan. Facility must develop and maintain an emergency preparedness plan that must be reviewed and updated at least annually
Interpretative Guidelines E-003 Emergency Preparedness Plan – Review • Facility must comply with all applicable Federal, State and local emergency preparedness requirements. • Facility must develop establish and maintain a comprehensive emergency preparedness program that meets the requirements of this section. • The emergency preparedness program must include: Emergency Plan. Facility must develop and maintain an emergency preparedness plan that must be reviewed and updated at least annually
 Survey Procedures E-003 Emergency Plan • Emergency preparedness plan must include all of the required elements under the standard. The format of the emergency preparedness plan that a facility uses is at its discretion. • The plan provides the framework, which includes conducting facilitybased and community-based risk assessments that will assist a facility in addressing the needs of their resident populations.
Survey Procedures E-003 Emergency Plan • Emergency preparedness plan must include all of the required elements under the standard. The format of the emergency preparedness plan that a facility uses is at its discretion. • The plan provides the framework, which includes conducting facilitybased and community-based risk assessments that will assist a facility in addressing the needs of their resident populations.
 Survey Procedures E-003 Emergency Plan • Approach is specific to the location of the facility and considers particular hazards most likely to occur including, but are not limited to: • Natural disasters • Man-made disasters, • Facility-based disasters that include but are not limited to: ; • Equipment and utility failures, including electricity, sewer, gas water, etc. • Interruptions in communication • Cyber-attacks; • Loss of all or portion of a facility • Interruptions to the normal operations such as weather, missing resident, etc.
Survey Procedures E-003 Emergency Plan • Approach is specific to the location of the facility and considers particular hazards most likely to occur including, but are not limited to: • Natural disasters • Man-made disasters, • Facility-based disasters that include but are not limited to: ; • Equipment and utility failures, including electricity, sewer, gas water, etc. • Interruptions in communication • Cyber-attacks; • Loss of all or portion of a facility • Interruptions to the normal operations such as weather, missing resident, etc.
 Survey Procedures E-003 Survey Protocol • Arrangements or contracts to maintain essential utility services during an emergency should describe the timeframe within which the contractor is required to initiate services • How they will be procured and delivered in the facility’s local area, and that the contractor will continue to supply the essential items throughout and to the end of emergencies of varying duration. • Ask facility leadership to identify the hazards (e. g. natural, man-made, facility, geographic, etc. ) that were identified in the facility’s risk assessment and how the risk assessment was conducted. • Review the plan to verify it contains all of the required elements • Verify that the plan is reviewed and updated annually by looking for documentation of the date of the review and updates that were made to the plan based on the review
Survey Procedures E-003 Survey Protocol • Arrangements or contracts to maintain essential utility services during an emergency should describe the timeframe within which the contractor is required to initiate services • How they will be procured and delivered in the facility’s local area, and that the contractor will continue to supply the essential items throughout and to the end of emergencies of varying duration. • Ask facility leadership to identify the hazards (e. g. natural, man-made, facility, geographic, etc. ) that were identified in the facility’s risk assessment and how the risk assessment was conducted. • Review the plan to verify it contains all of the required elements • Verify that the plan is reviewed and updated annually by looking for documentation of the date of the review and updates that were made to the plan based on the review
 Policies Recommended • Risk management approach using a hazard vulnerability assessment of the specific facility • Will work with local, state and federal authorities • Will comply with any federal 1135 waiver (President declares a disaster or emergency under the Stafford Act or National Emergencies Act and the HHS Secretary declares a public health emergency under Section 319 of the Public Health Service Act)
Policies Recommended • Risk management approach using a hazard vulnerability assessment of the specific facility • Will work with local, state and federal authorities • Will comply with any federal 1135 waiver (President declares a disaster or emergency under the Stafford Act or National Emergencies Act and the HHS Secretary declares a public health emergency under Section 319 of the Public Health Service Act)
 Interpretative Guidelines E-007 Population Served • The emergency plan must specify the population served within the facility and their unique vulnerabilities in the event of an emergency including: • Level of independence/ dependence • Ability to communicate • Transportation needs and abilities • Supervision needed for safety • Medical care/ diagnosis's that may impact resident significantly in emergency
Interpretative Guidelines E-007 Population Served • The emergency plan must specify the population served within the facility and their unique vulnerabilities in the event of an emergency including: • Level of independence/ dependence • Ability to communicate • Transportation needs and abilities • Supervision needed for safety • Medical care/ diagnosis's that may impact resident significantly in emergency
 Interpretative Guidelines E-007 Population Served • In addition to the facility- and community-based risk assessment, continuity of operations planning generally considers elements such as: essential personnel, essential functions, critical resources, vital records and IT data protection, alternate facility identification and location, and financial resources.
Interpretative Guidelines E-007 Population Served • In addition to the facility- and community-based risk assessment, continuity of operations planning generally considers elements such as: essential personnel, essential functions, critical resources, vital records and IT data protection, alternate facility identification and location, and financial resources.
 Plan Definition • Brief description of the plan • Insurance considerations including the coverage, scope and limitations. • Legal issuances detailing the roles and functions of nursing facilities in managing all phases of emergencies or disasters • Tasks to be performed • Resources to be needed
Plan Definition • Brief description of the plan • Insurance considerations including the coverage, scope and limitations. • Legal issuances detailing the roles and functions of nursing facilities in managing all phases of emergencies or disasters • Tasks to be performed • Resources to be needed
 Policies Recommended • Information about the facility including location, address etc. • Add photo of the facility • Add aerial photo of the facility including evacuation and assess routes (Google Maps)
Policies Recommended • Information about the facility including location, address etc. • Add photo of the facility • Add aerial photo of the facility including evacuation and assess routes (Google Maps)
 Interpretative Guidelines E-007 Facility Leadership • The emergency plan must identify which staff would assume specific roles in another’s absence through succession planning and delegations of authority. • At a minimum, there should be a qualified person who "is authorized in writing to act in the absence of the administrator or person legally responsible for the operations of the facility. "
Interpretative Guidelines E-007 Facility Leadership • The emergency plan must identify which staff would assume specific roles in another’s absence through succession planning and delegations of authority. • At a minimum, there should be a qualified person who "is authorized in writing to act in the absence of the administrator or person legally responsible for the operations of the facility. "
 Survey Procedures E-007 • Interview leadership and ask them to describe the following: • Facility’s resident population that would be at risk • Strategies the facility has put in place to address the needs of at- risk or vulnerable resident populations; • Services the facility would be able to provide during an emergency; • How the facility plans to continue operations during an emergency; • Delegations of authority and succession plans. • Verify that all of the above are included in the written emergency plan.
Survey Procedures E-007 • Interview leadership and ask them to describe the following: • Facility’s resident population that would be at risk • Strategies the facility has put in place to address the needs of at- risk or vulnerable resident populations; • Services the facility would be able to provide during an emergency; • How the facility plans to continue operations during an emergency; • Delegations of authority and succession plans. • Verify that all of the above are included in the written emergency plan.
 Policies Recommended • Organizational chart • List of staff (names or positions that would ’act in the absence of the administrator’ or a secession plan) • Outline typical resident population • Outline transportation needs of resident population • State typical staffing by shift and position
Policies Recommended • Organizational chart • List of staff (names or positions that would ’act in the absence of the administrator’ or a secession plan) • Outline typical resident population • Outline transportation needs of resident population • State typical staffing by shift and position
 Survey Procedures E-006 All-Hazards • Facilities are expected to develop an emergency preparedness plan that is based on the facilitybased and community-based risk assessment using an “all-hazards” approach. • Core response management systems are similar for most disaster types. Capability of responding regardless of the cause or source of the emergency. • Specific event types will have peculiar parameters that staff will address • Summed up - there a variety of hazards or disasters that may occur but the range of possible consequences is limited • Shelter-in-place • Partial evacuation • Evacuation
Survey Procedures E-006 All-Hazards • Facilities are expected to develop an emergency preparedness plan that is based on the facilitybased and community-based risk assessment using an “all-hazards” approach. • Core response management systems are similar for most disaster types. Capability of responding regardless of the cause or source of the emergency. • Specific event types will have peculiar parameters that staff will address • Summed up - there a variety of hazards or disasters that may occur but the range of possible consequences is limited • Shelter-in-place • Partial evacuation • Evacuation
 Interpretative Guidelines E-009 Collaboration • Collaboration with local, tribal, regional, State, and Federal emergency preparedness officials' efforts to maintain an integrated response during a disaster or emergency situation • Facilities must document its efforts to contact these officials to engage in collaborative planning for an integrated emergency response. • Facilities are encouraged to participate in a healthcare coalition as it may provide assistance in planning and addressing broader community needs that may also be supported by local health department and emergency management resources.
Interpretative Guidelines E-009 Collaboration • Collaboration with local, tribal, regional, State, and Federal emergency preparedness officials' efforts to maintain an integrated response during a disaster or emergency situation • Facilities must document its efforts to contact these officials to engage in collaborative planning for an integrated emergency response. • Facilities are encouraged to participate in a healthcare coalition as it may provide assistance in planning and addressing broader community needs that may also be supported by local health department and emergency management resources.
 • Interview facility leadership and ask them to describe their process for ensuring cooperation and collaboration with local, tribal, regional, State, and Federal emergency preparedness officials' efforts to ensure an integrated response during a disaster or emergency situation. • Ask for documentation of the facility's efforts to contact such officials and, when applicable, its participation in collaborative and cooperative planning efforts. Survey Procedures E-009 Collaboration
• Interview facility leadership and ask them to describe their process for ensuring cooperation and collaboration with local, tribal, regional, State, and Federal emergency preparedness officials' efforts to ensure an integrated response during a disaster or emergency situation. • Ask for documentation of the facility's efforts to contact such officials and, when applicable, its participation in collaborative and cooperative planning efforts. Survey Procedures E-009 Collaboration
 Interpretative Guidelines E-006 Risk Assessment • Emergency Plan: • Be based on and include a documented, facilitybased and community-based risk assessment, utilizing an all-hazards approach, including missing residents. • Include strategies for addressing emergency events identified by the risk assessment.
Interpretative Guidelines E-006 Risk Assessment • Emergency Plan: • Be based on and include a documented, facilitybased and community-based risk assessment, utilizing an all-hazards approach, including missing residents. • Include strategies for addressing emergency events identified by the risk assessment.
 • When developing an emergency preparedness plan, facilities are expected") Hazard Vulnerability Assessment (HVA) • When developing an emergency preparedness plan, facilities are expected to consider, among other things, the following: • Identification of all business functions that should be continued during an emergency; • Identification of all risks or emergencies that the facility may reasonably expect to confront; • Consideration of the facility’s location; • Determination of what arrangements may be necessary with other health care facilities, or other entities that might be needed to ensure that essential services could be provided during an emergency.
Hazard Vulnerability Assessment (HVA) • When developing an emergency preparedness plan, facilities are expected to consider, among other things, the following: • Identification of all business functions that should be continued during an emergency; • Identification of all risks or emergencies that the facility may reasonably expect to confront; • Consideration of the facility’s location; • Determination of what arrangements may be necessary with other health care facilities, or other entities that might be needed to ensure that essential services could be provided during an emergency.
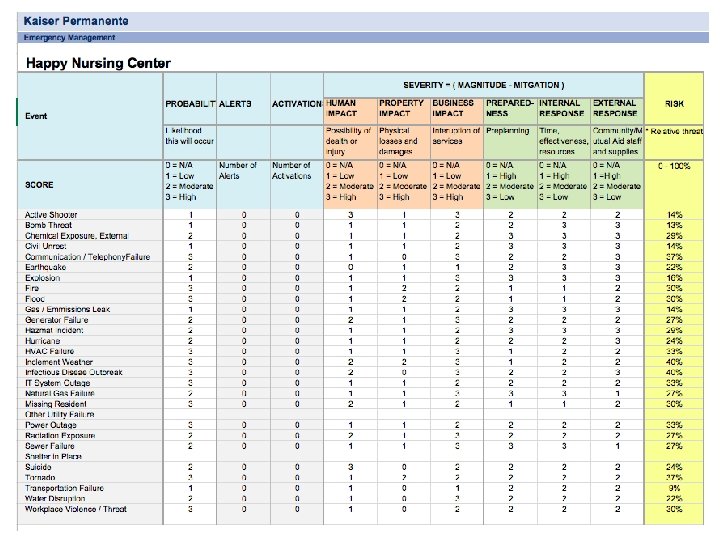
 Hazard Vulnerability Analysis Process of evaluating risk associated with a specific hazard and defined in terms of: § probability & frequency of occurrence § magnitude & severity § exposure & consequences § preparedness Vulnerability equals hazard/threat probability, plus severity minus prepared response V = Pb + S - Pr
Hazard Vulnerability Analysis Process of evaluating risk associated with a specific hazard and defined in terms of: § probability & frequency of occurrence § magnitude & severity § exposure & consequences § preparedness Vulnerability equals hazard/threat probability, plus severity minus prepared response V = Pb + S - Pr
 Kaiser Permanente HVA Tool www. calhospitalprepare. org/hazard-vulnerability-analysis
Kaiser Permanente HVA Tool www. calhospitalprepare. org/hazard-vulnerability-analysis
 Survey Procedures E-006 Risk Assessment • Ask to see the written documentation of the facility’s risk assessments and associated strategies. • Interview the facility leadership and ask which hazards (e. g. natural, man-made, facility, geographic) were included in the facility’s risk assessment, why they were included and how the risk assessment was conducted. • Verify the risk-assessment is based on an all-hazards approach specific to the geographic location of the facility and encompasses potential hazards. • For LTC facilities have written plans and the procedures are required to also include missing residents and clients, respectively, within their emergency plans
Survey Procedures E-006 Risk Assessment • Ask to see the written documentation of the facility’s risk assessments and associated strategies. • Interview the facility leadership and ask which hazards (e. g. natural, man-made, facility, geographic) were included in the facility’s risk assessment, why they were included and how the risk assessment was conducted. • Verify the risk-assessment is based on an all-hazards approach specific to the geographic location of the facility and encompasses potential hazards. • For LTC facilities have written plans and the procedures are required to also include missing residents and clients, respectively, within their emergency plans
 Survey Procedures E-013 Policies and Procedures • Expected to align with the identified hazards within the facility’s risk assessment and the facility’s overall emergency preparedness program. • Review the written policies and procedures which address the facility’s emergency plan and verify the following: • Policies and procedures were developed based on the facility- and community- based risk assessment and communication plan, utilizing an all-hazards approach. • Ask to see documentation that verifies the policies and procedures have been reviewed and updated on an annual basis.
Survey Procedures E-013 Policies and Procedures • Expected to align with the identified hazards within the facility’s risk assessment and the facility’s overall emergency preparedness program. • Review the written policies and procedures which address the facility’s emergency plan and verify the following: • Policies and procedures were developed based on the facility- and community- based risk assessment and communication plan, utilizing an all-hazards approach. • Ask to see documentation that verifies the policies and procedures have been reviewed and updated on an annual basis.
 Interpretive Guidelines E-015 Policies and Procedures • Policies and procedures must address alternate sources of energy to maintain the following • Temperatures to protect resident health and safety • Emergency lighting. • Fire detection, extinguishing, and alarm systems. • Sewage and waste disposal • Alternate sources of energy depend on the resources available to a facility, such as battery-operated lights, generator, etc. • CMS does not require facilities to have or install generators • Not required to upgrade their electrical systems. • Facilities must establish policies and procedures that determine how required heating and cooling of their facility will be maintained during an emergency situation.
Interpretive Guidelines E-015 Policies and Procedures • Policies and procedures must address alternate sources of energy to maintain the following • Temperatures to protect resident health and safety • Emergency lighting. • Fire detection, extinguishing, and alarm systems. • Sewage and waste disposal • Alternate sources of energy depend on the resources available to a facility, such as battery-operated lights, generator, etc. • CMS does not require facilities to have or install generators • Not required to upgrade their electrical systems. • Facilities must establish policies and procedures that determine how required heating and cooling of their facility will be maintained during an emergency situation.
 Interpretive Guidelines E-015 Policies and Procedures • Facilities must be able to provide for adequate subsistence for all residents and staff for the duration of an emergency whether they evacuate or shelter in place, including: food, water, medical and pharmaceutical supplies • Facilities have flexibility in identifying their individual subsistence needs that would be required during an emergency as there are no set requirements or standards for the amount of provisions • Additionally, when facilities determine their supply needs, they are expected to consider the possibility that volunteers, visitors, and individuals from the community may arrive at the facility to offer assistance or seek shelter.
Interpretive Guidelines E-015 Policies and Procedures • Facilities must be able to provide for adequate subsistence for all residents and staff for the duration of an emergency whether they evacuate or shelter in place, including: food, water, medical and pharmaceutical supplies • Facilities have flexibility in identifying their individual subsistence needs that would be required during an emergency as there are no set requirements or standards for the amount of provisions • Additionally, when facilities determine their supply needs, they are expected to consider the possibility that volunteers, visitors, and individuals from the community may arrive at the facility to offer assistance or seek shelter.
 Interpretive Guidelines E-015 Policies and Procedures • Facilities are not required to provide onsite treatment of sewage but must make provisions for maintaining necessary services and CMS is not specifying any required provisions regarding treatment of sewage and necessary services but are required to follow their current facility-type requirements which may address these areas. • LTC facilities are already required to meet Food Receiving and Storage provisions at § 483. 35(i) Sanitary Conditions, which contain requirements for keeping food off the floor and clear of ceiling sprinklers, sewer/waste disposal pipes, and vents can also help maintain food quality and prevent contamination.
Interpretive Guidelines E-015 Policies and Procedures • Facilities are not required to provide onsite treatment of sewage but must make provisions for maintaining necessary services and CMS is not specifying any required provisions regarding treatment of sewage and necessary services but are required to follow their current facility-type requirements which may address these areas. • LTC facilities are already required to meet Food Receiving and Storage provisions at § 483. 35(i) Sanitary Conditions, which contain requirements for keeping food off the floor and clear of ceiling sprinklers, sewer/waste disposal pipes, and vents can also help maintain food quality and prevent contamination.
 Policies Recommendations • Facility should address how they indent to meet electric and HVAC needs of residents. • Address utility outages including electric, sewer, water, and internet • Set facility standard for sustaining water, food and medical supplies (meds) • Policy confirming sanitation (F 371 and F 372)
Policies Recommendations • Facility should address how they indent to meet electric and HVAC needs of residents. • Address utility outages including electric, sewer, water, and internet • Set facility standard for sustaining water, food and medical supplies (meds) • Policy confirming sanitation (F 371 and F 372)
 Interpretative Guidelines E-029 Communication Plan • CMS expects facilities to develop and maintain an emergency preparedness communication plan • Patient care must be well-coordinated within the facility, and with state and local public health departments and emergency management agencies • Facilities in rural or remote areas with limited connectivity to communication methodologies such as the Internet, World Wide Web, or cellular capabilities need to ensure their communication plan addresses how they would communicate and comply with this requirement in the absence of these communication methodologies. • Optional communication methods facilities may consider include satellite phones, radios and short wave radios.
Interpretative Guidelines E-029 Communication Plan • CMS expects facilities to develop and maintain an emergency preparedness communication plan • Patient care must be well-coordinated within the facility, and with state and local public health departments and emergency management agencies • Facilities in rural or remote areas with limited connectivity to communication methodologies such as the Internet, World Wide Web, or cellular capabilities need to ensure their communication plan addresses how they would communicate and comply with this requirement in the absence of these communication methodologies. • Optional communication methods facilities may consider include satellite phones, radios and short wave radios.
 Plain Language Announcements FACILITY ALERT RECOMMENDED PLAIN LANGUAGE Evacuation/Relocation Facility Alert + Evacuation + Directions Fire Facility Alert + Fire + Location + Directions Utility/Technology Interruption + Directions Severe Weather Event + Location + Directions Work Place Violence/ Active “Security Alert + Location + Directions Shooter Bomb Threat “Security Alert + Location + Directions Missing Person “Security Alert + Missing Person + Location + Directions Security Assistance “Security Alert + Location + Directions General Alert + + Location + Directions
Plain Language Announcements FACILITY ALERT RECOMMENDED PLAIN LANGUAGE Evacuation/Relocation Facility Alert + Evacuation + Directions Fire Facility Alert + Fire + Location + Directions Utility/Technology Interruption + Directions Severe Weather Event + Location + Directions Work Place Violence/ Active “Security Alert + Location + Directions Shooter Bomb Threat “Security Alert + Location + Directions Missing Person “Security Alert + Missing Person + Location + Directions Security Assistance “Security Alert + Location + Directions General Alert + + Location + Directions
 Interpretative Guidelines E-030 Communications Plan The communication plan must include all of the following: • Names and contact information • Key Staff • Key contractors and vendors • Medical personnel • Other facilities and alternate sites • residents’ physicians Facilities which utilize electronic data storage should be able to provide evidence of data back-up with hard copies or demonstrate capability to reproduce contact lists or access this data during emergencies.
Interpretative Guidelines E-030 Communications Plan The communication plan must include all of the following: • Names and contact information • Key Staff • Key contractors and vendors • Medical personnel • Other facilities and alternate sites • residents’ physicians Facilities which utilize electronic data storage should be able to provide evidence of data back-up with hard copies or demonstrate capability to reproduce contact lists or access this data during emergencies.
 • Verify contacts are included in the communication -list of the contacts and information including key staff, vendors and others. • Verify that all contact information has been reviewed and updated at least annually by asking to see evidence of the annual review. Survey Procedures E-030
• Verify contacts are included in the communication -list of the contacts and information including key staff, vendors and others. • Verify that all contact information has been reviewed and updated at least annually by asking to see evidence of the annual review. Survey Procedures E-030
 Interpretative Guidelines E-031 Required Information Contact information for • Federal, State, regional, or local emergency preparedness staff • The State Licensing and Certification Agency. • The Office of the State Long-Term Care Ombudsman. • Other sources of assistance. Survey Procedures • Verify that all required contacts are included in the communication plan by asking to see a list of the contacts with their contact information. • Verify that all contact information has been reviewed and updated at least annually by asking to see evidence of the annual review.
Interpretative Guidelines E-031 Required Information Contact information for • Federal, State, regional, or local emergency preparedness staff • The State Licensing and Certification Agency. • The Office of the State Long-Term Care Ombudsman. • Other sources of assistance. Survey Procedures • Verify that all required contacts are included in the communication plan by asking to see a list of the contacts with their contact information. • Verify that all contact information has been reviewed and updated at least annually by asking to see evidence of the annual review.
 Interpretative Guidelines E-032 Alternate Communications • Facilities are required to have primary and alternate means of communicating and it is expected that facilities would consider pagers, cellular telephones, radio transceivers (that is, walkietalkies) as well as satellite telephone communications systems. • Facility should register for the National Communication System (NCS) • Government Emergency Telecommunications Services (GETS) • Telecommunications Service Priority (TSP) Program • Wireless Priority Service (WPS)
Interpretative Guidelines E-032 Alternate Communications • Facilities are required to have primary and alternate means of communicating and it is expected that facilities would consider pagers, cellular telephones, radio transceivers (that is, walkietalkies) as well as satellite telephone communications systems. • Facility should register for the National Communication System (NCS) • Government Emergency Telecommunications Services (GETS) • Telecommunications Service Priority (TSP) Program • Wireless Priority Service (WPS)
 • The National Communications System (NCS) was established to protect") National Communications System (NCS) • The National Communications System (NCS) was established to protect the critical telecommunications and electrical infrastructure of the United States in the event of emergencies or catastrophes. • The NCS governs Telecommunications Services Priorities for installation of and/or restoration of services on critical telecommunications circuits and oversees three service programs: the Government Emergency Telecommunications System (GETS), the Wireless Priority Service (WPS), and the Telecommunications Service Priority (TSP) Program.
National Communications System (NCS) • The National Communications System (NCS) was established to protect the critical telecommunications and electrical infrastructure of the United States in the event of emergencies or catastrophes. • The NCS governs Telecommunications Services Priorities for installation of and/or restoration of services on critical telecommunications circuits and oversees three service programs: the Government Emergency Telecommunications System (GETS), the Wireless Priority Service (WPS), and the Telecommunications Service Priority (TSP) Program.
 • Telecommunications Service Priority (TSP) is a program that authorizes") Telecommunications Service Priority (TSP) • Telecommunications Service Priority (TSP) is a program that authorizes national security and emergency preparedness (NS/EP) organizations to receive priority treatment for vital voice and data circuits. • The TSP program provides service vendors a FCC mandate to prioritize requests by identifying those critical services • TSP assignment ensures that it will receive priority attention by the service vendor before any non-TSP service. • For information on TSP and all Priority Telecommunications programs, contact the DHS Priority Telecommunications Service Center at 866 -627 -2255 or support@priority-info. com.
Telecommunications Service Priority (TSP) • Telecommunications Service Priority (TSP) is a program that authorizes national security and emergency preparedness (NS/EP) organizations to receive priority treatment for vital voice and data circuits. • The TSP program provides service vendors a FCC mandate to prioritize requests by identifying those critical services • TSP assignment ensures that it will receive priority attention by the service vendor before any non-TSP service. • For information on TSP and all Priority Telecommunications programs, contact the DHS Priority Telecommunications Service Center at 866 -627 -2255 or support@priority-info. com.
 • Wireless Priority Service (WPS) is intended to be used") Wireless Priority Service (WPS) • Wireless Priority Service (WPS) is intended to be used in an emergency or crisis situation when the wireless network is congested and the probability of completing a normal call is reduced. • Typical WPS users are responsible for the command control functions critical to management of and response to national security and emergency situations, particularly during the first 24 to 72 hours following an event. • WPS is widely available from AT&T, Sprint, T-Mobile, U. S. Cellular, and Verizon Wireless. • For information on WPS and all Priority Telecommunications programs, contact the DHS Priority Telecommunications Service center at 866 -627 -2255 or support@priority-info. com
Wireless Priority Service (WPS) • Wireless Priority Service (WPS) is intended to be used in an emergency or crisis situation when the wireless network is congested and the probability of completing a normal call is reduced. • Typical WPS users are responsible for the command control functions critical to management of and response to national security and emergency situations, particularly during the first 24 to 72 hours following an event. • WPS is widely available from AT&T, Sprint, T-Mobile, U. S. Cellular, and Verizon Wireless. • For information on WPS and all Priority Telecommunications programs, contact the DHS Priority Telecommunications Service center at 866 -627 -2255 or support@priority-info. com
 • The Government Emergency Telecommunications Service (GETS) supports first") Government Emergency Telecommunications Service (GETS) • The Government Emergency Telecommunications Service (GETS) supports first responders; and other authorized national security and emergency preparedness users. It is intended to be used in an emergency or crisis situation when the landline network is congested and the probability of completing a normal call is reduced. • The Office of Emergency Communications recommends that individuals requesting WPS also request a GETS card. The registration process will allow you to request both services at the same time. • For information on GETS and all DHS Office of Emergency Communications Priority Telecommunications programs, contact the DHS Priority Telecommunications Service Center at 866 -627 -2255 or support@priorityinfo. com.
Government Emergency Telecommunications Service (GETS) • The Government Emergency Telecommunications Service (GETS) supports first responders; and other authorized national security and emergency preparedness users. It is intended to be used in an emergency or crisis situation when the landline network is congested and the probability of completing a normal call is reduced. • The Office of Emergency Communications recommends that individuals requesting WPS also request a GETS card. The registration process will allow you to request both services at the same time. • For information on GETS and all DHS Office of Emergency Communications Priority Telecommunications programs, contact the DHS Priority Telecommunications Service Center at 866 -627 -2255 or support@priorityinfo. com.
 Media Plan • Identify a spokes person • Task the spokesperson with gathering information about an emergency and to answer basic questions from the media • To do this properly, and expeditiously, the spokesperson should: • Know basic statistics about the organization, number of residents, census data (number of beds, units, etc. ), the number of employees, and a general outline of the company and its mission statement. • Social media • Twitter • Face Book • Instagram
Media Plan • Identify a spokes person • Task the spokesperson with gathering information about an emergency and to answer basic questions from the media • To do this properly, and expeditiously, the spokesperson should: • Know basic statistics about the organization, number of residents, census data (number of beds, units, etc. ), the number of employees, and a general outline of the company and its mission statement. • Social media • Twitter • Face Book • Instagram
 Interpretative Guidelines E-035 Resident & Family Information • Required to share emergency preparedness plans and policies with family members and residents • Facilities may provide a quick “Fact Sheet” or informational brochure to the family members and residents or which may highlight the major sections of the emergency plan and policies and procedures deemed appropriate by the facility.
Interpretative Guidelines E-035 Resident & Family Information • Required to share emergency preparedness plans and policies with family members and residents • Facilities may provide a quick “Fact Sheet” or informational brochure to the family members and residents or which may highlight the major sections of the emergency plan and policies and procedures deemed appropriate by the facility.
 Survey Procedures E-035 Resident & Family Information • Ask staff to demonstrate the method the facility has developed for sharing the emergency plan with residents or clients and their families or representatives. • Interview residents or clients and their families or representatives and ask them if they have been given information regarding the facility’s emergency plan. • Verify the communication plan includes a method for sharing information from the emergency plan, and that the facility has determined it is appropriate with residents or clients and their families or representatives by reviewing the plan.
Survey Procedures E-035 Resident & Family Information • Ask staff to demonstrate the method the facility has developed for sharing the emergency plan with residents or clients and their families or representatives. • Interview residents or clients and their families or representatives and ask them if they have been given information regarding the facility’s emergency plan. • Verify the communication plan includes a method for sharing information from the emergency plan, and that the facility has determined it is appropriate with residents or clients and their families or representatives by reviewing the plan.
 Survey Procedures • Verify the communication plan includes primary and alternate means for communicating with facility staff, Federal, State, tribal, regional and local emergency management agencies by reviewing the communication plan. • Ask to see the communications equipment or communication systems listed in the plan.
Survey Procedures • Verify the communication plan includes primary and alternate means for communicating with facility staff, Federal, State, tribal, regional and local emergency management agencies by reviewing the communication plan. • Ask to see the communications equipment or communication systems listed in the plan.
 Policies Recommended • Comprehensive communication structure including the use of various pieces of infrastructure i. e. landlines, cell, radios, etc. • Participation with NPS – GETs, WPS, TSP • Family-Resident fact sheet • List of key staff, vendors, etc. • Media plan including social media aspects utilized by facility
Policies Recommended • Comprehensive communication structure including the use of various pieces of infrastructure i. e. landlines, cell, radios, etc. • Participation with NPS – GETs, WPS, TSP • Family-Resident fact sheet • List of key staff, vendors, etc. • Media plan including social media aspects utilized by facility
 Interpretative Guidelines E-033 Sharing Information • Facilities are required to develop a method for sharing information and medical care documentation for residents under the facility's care, as necessary, with other health care providers to maintain continuity of care. • Facilities must have a communication system in place capable of generating timely, accurate information that could be disseminated to family members and others. Facilities have the flexibility to develop and maintain their own system in a manner that best meets its needs.
Interpretative Guidelines E-033 Sharing Information • Facilities are required to develop a method for sharing information and medical care documentation for residents under the facility's care, as necessary, with other health care providers to maintain continuity of care. • Facilities must have a communication system in place capable of generating timely, accurate information that could be disseminated to family members and others. Facilities have the flexibility to develop and maintain their own system in a manner that best meets its needs.
 Survey Procedures E-033 Sharing Information • Verify the communication plan includes a method for sharing information and medical documentation for residents under the facility's care, • Verify the means the facility will use to release resident information to include the general condition and location of residents by reviewing the communication plan
Survey Procedures E-033 Sharing Information • Verify the communication plan includes a method for sharing information and medical documentation for residents under the facility's care, • Verify the means the facility will use to release resident information to include the general condition and location of residents by reviewing the communication plan
 Interpretive Guidelines E-023 Resident Record • A system of medical documentation that preserves patient information, protects confidentiality of patient information, and secures and maintains availability of records. • Ensure that patient records are secure and readily available to support continuity of care during emergency. Survey Procedures • Ask to see a copy of the policies and procedures that documents the medical record documentation system the facility has developed to preserves patient information, protects confidentiality of patient information, and secures and maintains availability of records.
Interpretive Guidelines E-023 Resident Record • A system of medical documentation that preserves patient information, protects confidentiality of patient information, and secures and maintains availability of records. • Ensure that patient records are secure and readily available to support continuity of care during emergency. Survey Procedures • Ask to see a copy of the policies and procedures that documents the medical record documentation system the facility has developed to preserves patient information, protects confidentiality of patient information, and secures and maintains availability of records.
 AHCA Red Envelope • “Resident Evacuation Documents, ” which was developed by AHCA’s Disaster Planning Committee • The RED envelope is pre-printed with the basic information that should go with a resident in an evacuation, e. g. , allergies, photo, facilities emergency contact. In addition it is waterproof • Simple and effective tool for evacuation preparation
AHCA Red Envelope • “Resident Evacuation Documents, ” which was developed by AHCA’s Disaster Planning Committee • The RED envelope is pre-printed with the basic information that should go with a resident in an evacuation, e. g. , allergies, photo, facilities emergency contact. In addition it is waterproof • Simple and effective tool for evacuation preparation
 Interpretative Guidelines E-018 Tracking Resident and Staff • A system to track the location of on-duty staff and sheltered residents in the care during an emergency. If on-duty staff and sheltered residents are relocated during the emergency, the facility must document the specific name and location of the receiving facility or other location. Survey Procedures • Ask staff to describe and/or demonstrate the tracking system used to document locations of residents and staff. • Verify that the tracking system is documented as part of the facilities’ emergency plan policies and procedures.
Interpretative Guidelines E-018 Tracking Resident and Staff • A system to track the location of on-duty staff and sheltered residents in the care during an emergency. If on-duty staff and sheltered residents are relocated during the emergency, the facility must document the specific name and location of the receiving facility or other location. Survey Procedures • Ask staff to describe and/or demonstrate the tracking system used to document locations of residents and staff. • Verify that the tracking system is documented as part of the facilities’ emergency plan policies and procedures.
 Policies Recommended • Policy on what facility believes is minimum medical information is necessary to transfer with the resident in a relocation. • Method of how the facility will transfer information • Staff and resident tracking policy, procedure and form
Policies Recommended • Policy on what facility believes is minimum medical information is necessary to transfer with the resident in a relocation. • Method of how the facility will transfer information • Staff and resident tracking policy, procedure and form
 Interpretative Guidelines E-034 Nursing Home Incident Command A means of providing information about the facility occupancy, needs, and its ability to provide assistance, to a the Incident Command Center • Incident Command System is a management system designed to enable effective and efficient incident management by integrating a combination of facilities, equipment, personnel, procedures, and communications operating within a common organizational structure. Survey Procedures • Verify the communication plan includes a means of providing information about the facility’s needs, and its ability to provide assistance
Interpretative Guidelines E-034 Nursing Home Incident Command A means of providing information about the facility occupancy, needs, and its ability to provide assistance, to a the Incident Command Center • Incident Command System is a management system designed to enable effective and efficient incident management by integrating a combination of facilities, equipment, personnel, procedures, and communications operating within a common organizational structure. Survey Procedures • Verify the communication plan includes a means of providing information about the facility’s needs, and its ability to provide assistance
 Incident Management • Many incidents will be so large or complex as to require multi -organizational responses • All partners share a common goal, yet retain their unique responsibilities • Fire/EMS • Law Enforcement • Public Health and Medical • Community stakeholders
Incident Management • Many incidents will be so large or complex as to require multi -organizational responses • All partners share a common goal, yet retain their unique responsibilities • Fire/EMS • Law Enforcement • Public Health and Medical • Community stakeholders
 Activation of Emergency Response • Once notified of event the highest ranking facility staff member assumes role of Incident Commander position • Incident Commander has the responsibility at that moment to declare the emergency and put facility plans in motion • Pre-designated staff will report to command post • All staff must know chair of command who to notify • Remember most staff will continue to preform their normal duties
Activation of Emergency Response • Once notified of event the highest ranking facility staff member assumes role of Incident Commander position • Incident Commander has the responsibility at that moment to declare the emergency and put facility plans in motion • Pre-designated staff will report to command post • All staff must know chair of command who to notify • Remember most staff will continue to preform their normal duties
: Leads the response, appoints section") Basic NHICS Job Action Overview • Incident Commander (Leader): Leads the response, appoints section leaders, approves plans and key actions • Operations Section (Doers): Handles key actions including first aid, search and rescue, fire suppression, securing the site • Planning Section (Planners): Gathers information, thinks ahead, makes and revises action plans and keeps all team members informed and communicating. • Logistics Section(Getters): Finds, distributes and stores all necessary resources • Finance Section ($): Tracks all expenses, claims, activities and personnel time and is the record keeper for the incident
Basic NHICS Job Action Overview • Incident Commander (Leader): Leads the response, appoints section leaders, approves plans and key actions • Operations Section (Doers): Handles key actions including first aid, search and rescue, fire suppression, securing the site • Planning Section (Planners): Gathers information, thinks ahead, makes and revises action plans and keeps all team members informed and communicating. • Logistics Section(Getters): Finds, distributes and stores all necessary resources • Finance Section ($): Tracks all expenses, claims, activities and personnel time and is the record keeper for the incident
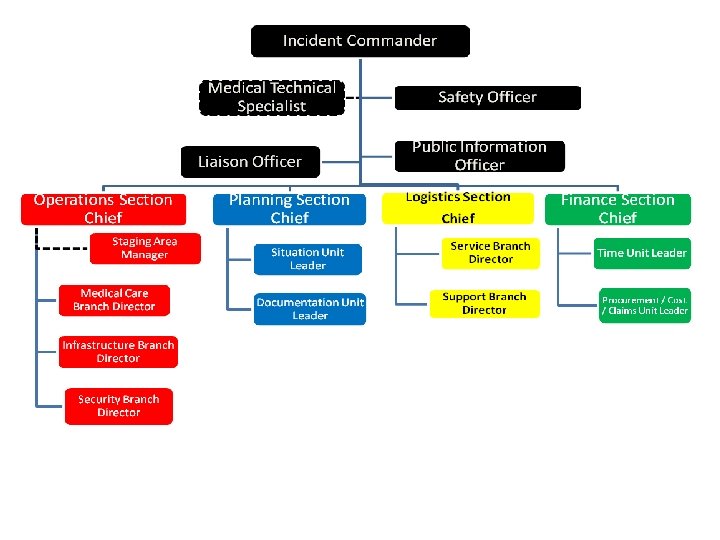
 Basic NHICS Structure INCIDENT COMMANDER Medical Tech Officer Liaison Officer LOGISTICS SECTION PLANNING SECTION Safety Officer FINANCE SECTION OPERATIONS SECTION
Basic NHICS Structure INCIDENT COMMANDER Medical Tech Officer Liaison Officer LOGISTICS SECTION PLANNING SECTION Safety Officer FINANCE SECTION OPERATIONS SECTION
 Incident Commander • Only position always staffed • Provides overall leadership for incident response • Initial IC holds post until they delegate the post to another qualified/more qualified person • Demonstrates initiative by taking action • Motivates responders • Communicates specific instructions/ feedback • Supervises the scene • Delegates authority • Understands and accepts the need to be flexible, modify plans
Incident Commander • Only position always staffed • Provides overall leadership for incident response • Initial IC holds post until they delegate the post to another qualified/more qualified person • Demonstrates initiative by taking action • Motivates responders • Communicates specific instructions/ feedback • Supervises the scene • Delegates authority • Understands and accepts the need to be flexible, modify plans
: • Planning Section (Planners) • Logistics Section(Getters) • Finance") • Operations Section (Doers): • Planning Section (Planners) • Logistics Section(Getters) • Finance Section ($) Job Action Overview
• Operations Section (Doers): • Planning Section (Planners) • Logistics Section(Getters) • Finance Section ($) Job Action Overview
 Operations Section • Direct and coordinate all operations • Carries out the plan using defined objectives • Request resources through the IC • Keep the IC informed of the situation and resource status within operations Operations Section Chief Staging Area Manager Medical Care Branch Director Infrastructure Branch Director Security Branch Director
Operations Section • Direct and coordinate all operations • Carries out the plan using defined objectives • Request resources through the IC • Keep the IC informed of the situation and resource status within operations Operations Section Chief Staging Area Manager Medical Care Branch Director Infrastructure Branch Director Security Branch Director
 Planning Section • Collection, evaluation, dissemination and use of information about the development of the incident and status of resources • Maintains resource status • Maintains documentation for incident reports • Incident Action Plan- defines response activities and resource utilization for a specified time period Planning Section Chief Situation Unit Leader Documentation Unit Leader
Planning Section • Collection, evaluation, dissemination and use of information about the development of the incident and status of resources • Maintains resource status • Maintains documentation for incident reports • Incident Action Plan- defines response activities and resource utilization for a specified time period Planning Section Chief Situation Unit Leader Documentation Unit Leader
 Logistics Section • Responsible for providing facilities, services, and materials, including personnel to operate the requested equipment for the incident • Provides support, resources, and other essential services to meet the operational objectives • Great significance in longterm or extended operations Logistics Section Chief Service Branch Director Support Branch Director
Logistics Section • Responsible for providing facilities, services, and materials, including personnel to operate the requested equipment for the incident • Provides support, resources, and other essential services to meet the operational objectives • Great significance in longterm or extended operations Logistics Section Chief Service Branch Director Support Branch Director
 Finance Section • The Finance Section Chief tracks costs, personnel records, requisitions, and administrates procurement contracts required by Logistics. • Monitors costs related to the incident • Providing accounting, procurement, time recording, and cost analyses
Finance Section • The Finance Section Chief tracks costs, personnel records, requisitions, and administrates procurement contracts required by Logistics. • Monitors costs related to the incident • Providing accounting, procurement, time recording, and cost analyses
 Job Action Sheet • One JAS for each position • Focused objective • Concise mission statement • Prioritized activities • May to be customized (except for title and mission)
Job Action Sheet • One JAS for each position • Focused objective • Concise mission statement • Prioritized activities • May to be customized (except for title and mission)
 Single vs. Unified Command Single command • One organization and single Incident commander has complete responsibility for incident Unified command • Multiple agencies / organizations share responsibility • Collective / collaborative approach • Single set of objectives for multiple agencies • Improved information flow and coordination • Agencies understand joint priorities and restrictions • Single IAP
Single vs. Unified Command Single command • One organization and single Incident commander has complete responsibility for incident Unified command • Multiple agencies / organizations share responsibility • Collective / collaborative approach • Single set of objectives for multiple agencies • Improved information flow and coordination • Agencies understand joint priorities and restrictions • Single IAP
 Implementation • Appoint someone to be in charge of the implementation effort • Convene a work group • Read the NHICS Guidebook for background assistance • Be clear on final approval process • Outline the activities to complete • Set up a work schedule • Consider developing the program with other community SNFs for standardization and mutual aid assistance • Invite Fire/EMS/Public Health/EMA/ and nursing facilities to participate where appropriate
Implementation • Appoint someone to be in charge of the implementation effort • Convene a work group • Read the NHICS Guidebook for background assistance • Be clear on final approval process • Outline the activities to complete • Set up a work schedule • Consider developing the program with other community SNFs for standardization and mutual aid assistance • Invite Fire/EMS/Public Health/EMA/ and nursing facilities to participate where appropriate
 Determine Your IMT • Review the three NHICS IMT charts • Determine what adjustments in the command positions you want to make • Determine who can assume each role • Choose multiple persons (2 -3) for each position • Limit number times person can be listed
Determine Your IMT • Review the three NHICS IMT charts • Determine what adjustments in the command positions you want to make • Determine who can assume each role • Choose multiple persons (2 -3) for each position • Limit number times person can be listed
 Develop a Command Kit • Determine what you want to assemble into a kit for each position –IMT chart/vest –JAS for the position(s) –Forms for the position to complete –Other tools – radio/directories/paper/pens • Put them together –Place in labeled gym bag or box • Place in a secure location • Check on them periodically
Develop a Command Kit • Determine what you want to assemble into a kit for each position –IMT chart/vest –JAS for the position(s) –Forms for the position to complete –Other tools – radio/directories/paper/pens • Put them together –Place in labeled gym bag or box • Place in a secure location • Check on them periodically
 • Where your key command personnel work") Identify a Nursing Home Command Center (NHCC) • Where your key command personnel work • Adequate in size to accommodate personnel – Accessible /safe/secure – Sufficient room for the assigned personnel • Access to needed technology – Phones – Radios that work in the room – Fax – Printers – Computers • Close to bathrooms/food • Arrange for maintenance during an incident
Identify a Nursing Home Command Center (NHCC) • Where your key command personnel work • Adequate in size to accommodate personnel – Accessible /safe/secure – Sufficient room for the assigned personnel • Access to needed technology – Phones – Radios that work in the room – Fax – Printers – Computers • Close to bathrooms/food • Arrange for maintenance during an incident
 California Health Care Facilities Disaster Website http: //www. cahfdisasterprep. com
California Health Care Facilities Disaster Website http: //www. cahfdisasterprep. com
 Policies Recommended • The commitment to use and implement Nursing Home Incident Command • How the facility will respond to emergencies • Basic structure of NHICS • Who will be the Incident Management Team • How the facility Incident Commander will work with local, state and federal officials (unified command)
Policies Recommended • The commitment to use and implement Nursing Home Incident Command • How the facility will respond to emergencies • Basic structure of NHICS • Who will be the Incident Management Team • How the facility Incident Commander will work with local, state and federal officials (unified command)
 Interpretative Guidelines E-020 Evacuation • Evacuation from the facility, which includes consideration of care and treatment needs of evacuees; staff responsibilities; transportation; identification of evacuation location(s); and primary and alternate means of communication • Facilities must consider what designated transportation services would be most appropriate • Landline telephone services to contact transportation companies for evacuation or reporting evacuation needs to emergency officials; whereas alternate means account for loss of power or telephone services in the local area. In this event, alternate means may include satellite phones for contacting evacuation assistance.
Interpretative Guidelines E-020 Evacuation • Evacuation from the facility, which includes consideration of care and treatment needs of evacuees; staff responsibilities; transportation; identification of evacuation location(s); and primary and alternate means of communication • Facilities must consider what designated transportation services would be most appropriate • Landline telephone services to contact transportation companies for evacuation or reporting evacuation needs to emergency officials; whereas alternate means account for loss of power or telephone services in the local area. In this event, alternate means may include satellite phones for contacting evacuation assistance.
 Key Considerations
Key Considerations
 Alternate Care Site? • A location that is not currently providing healthcare services and will be converted to enable the provision of healthcare services • Alternate Care Site locations: ØRoadway Access and Security ØBuilding Size Considerations ØBuilding Security ØClinical Considerations ØPhysical Configuration Alternate Care Sites Ø Churches Ø Arenas Ø Schools Ø Stadiums
Alternate Care Site? • A location that is not currently providing healthcare services and will be converted to enable the provision of healthcare services • Alternate Care Site locations: ØRoadway Access and Security ØBuilding Size Considerations ØBuilding Security ØClinical Considerations ØPhysical Configuration Alternate Care Sites Ø Churches Ø Arenas Ø Schools Ø Stadiums
 Evacuation – Complete or Partial • Partial evacuation – Maybe the evacuation of a subset of facility patients – this may involve patients requiring specialized care that can no longer be safety delivered at the affected facility (intensive care, dialysis) • Or within the facility from a compromised compartment to safe one • Complete evacuation – complete evacuation of a facility due to an unsafe environment of care – usually will involve facility shutdown actions
Evacuation – Complete or Partial • Partial evacuation – Maybe the evacuation of a subset of facility patients – this may involve patients requiring specialized care that can no longer be safety delivered at the affected facility (intensive care, dialysis) • Or within the facility from a compromised compartment to safe one • Complete evacuation – complete evacuation of a facility due to an unsafe environment of care – usually will involve facility shutdown actions
 Relocation Movement of residents to an area/ compartment that is relative safety in response to a given threat or movement to staging area in preparation for evacuation. Horizontal - movement to a safe location on the same floor, preferably nearer to an emergency exit Vertical - movement of individuals to a safe location on a different floor when a horizontal evacuation cannot meet the service or safety needs of the patients or is unsafe
Relocation Movement of residents to an area/ compartment that is relative safety in response to a given threat or movement to staging area in preparation for evacuation. Horizontal - movement to a safe location on the same floor, preferably nearer to an emergency exit Vertical - movement of individuals to a safe location on a different floor when a horizontal evacuation cannot meet the service or safety needs of the patients or is unsafe
 Policies Recommended • Evacuation and relocation procedures including how the decision is determined • Transportation to address evacuation (based on facility population) • Staff responsibilities during an evacuation • Transfer of resident information • Locations for evacuation including other nursing centers and alternate site (non-certified) • Alternate cite • Is available and capable of house safely the facility residents • Mutual aid agreements (MOU)
Policies Recommended • Evacuation and relocation procedures including how the decision is determined • Transportation to address evacuation (based on facility population) • Staff responsibilities during an evacuation • Transfer of resident information • Locations for evacuation including other nursing centers and alternate site (non-certified) • Alternate cite • Is available and capable of house safely the facility residents • Mutual aid agreements (MOU)
 Recommended Documentation • Identify facility layout, type, description and key features (include a photo of facility) • Identify evacuation routes • Vendor Contact Information is readily available for medical, water, food, & transportation • Mutual aid agreements (MOU) are signed ahead of time with other critical partners • Staffing needs at Alternate Care Sites, hospitals or other LTC facilities as identified
Recommended Documentation • Identify facility layout, type, description and key features (include a photo of facility) • Identify evacuation routes • Vendor Contact Information is readily available for medical, water, food, & transportation • Mutual aid agreements (MOU) are signed ahead of time with other critical partners • Staffing needs at Alternate Care Sites, hospitals or other LTC facilities as identified
 Survey Procedures E-020 Evacuation • Review the emergency plan to verify it includes policies and procedures for safe evacuation from the facility and that it includes all of the required elements.
Survey Procedures E-020 Evacuation • Review the emergency plan to verify it includes policies and procedures for safe evacuation from the facility and that it includes all of the required elements.
 Interpretative Guidelines E-022 Shelter in Place Plan • Emergency plans must include a means for sheltering all residents , staff, and volunteers who remain in the facility in the event that an evacuation cannot be executed. • In certain disaster situations (such as tornadoes) , sheltering in place may be more appropriate as opposed to evacuation and would require a facility to have a means to shelter in place for such emergencies. Therefore, facilities are required to have policies and procedures for sheltering in place which align with the facility’s risk assessment.
Interpretative Guidelines E-022 Shelter in Place Plan • Emergency plans must include a means for sheltering all residents , staff, and volunteers who remain in the facility in the event that an evacuation cannot be executed. • In certain disaster situations (such as tornadoes) , sheltering in place may be more appropriate as opposed to evacuation and would require a facility to have a means to shelter in place for such emergencies. Therefore, facilities are required to have policies and procedures for sheltering in place which align with the facility’s risk assessment.
") Interpretive Guidance E-022 Shelter in Place Plan • Consider the ability of their building(s) to survive a disaster and what proactive steps they could take prior to an emergency to facilitate sheltering in place • The plan should take into account the appropriate facilities in the community to which residents could be transferred in the event of an emergency. Facilities must determine their policies based on the type of emergency and the types of residents , staff, volunteers and visitors that may be present during an emergency. • Based on its emergency plan, a facility could decide to have various approaches to sheltering some or all of its residents and staff.
Interpretive Guidance E-022 Shelter in Place Plan • Consider the ability of their building(s) to survive a disaster and what proactive steps they could take prior to an emergency to facilitate sheltering in place • The plan should take into account the appropriate facilities in the community to which residents could be transferred in the event of an emergency. Facilities must determine their policies based on the type of emergency and the types of residents , staff, volunteers and visitors that may be present during an emergency. • Based on its emergency plan, a facility could decide to have various approaches to sheltering some or all of its residents and staff.
 Survey Procedures E-022 Shelter in Place Plan • Verify the emergency plan includes policies and procedures for how it will provide a means to shelter in place for residents , staff and volunteers who remain in a facility. • Review the policies and procedures for sheltering in place and evaluate if they aligned with the facility’s emergency plan and risk assessment.
Survey Procedures E-022 Shelter in Place Plan • Verify the emergency plan includes policies and procedures for how it will provide a means to shelter in place for residents , staff and volunteers who remain in a facility. • Review the policies and procedures for sheltering in place and evaluate if they aligned with the facility’s emergency plan and risk assessment.
 Sheltering in Place • Definition: to take immediate shelter - usually for just a few hours or for less than 24 hours. Local authorities may instruct facilities to "shelter-in-place" if there were a chemical or radiological contaminants released into the environment. • Shelter-in-place is the preferred option, unless the decision is made by the facility administrator or supervisor, usually in coordination with response agencies, to evacuate, consider the circumstances of the incident, internally or externally and what is best for clients, staff and visitors.
Sheltering in Place • Definition: to take immediate shelter - usually for just a few hours or for less than 24 hours. Local authorities may instruct facilities to "shelter-in-place" if there were a chemical or radiological contaminants released into the environment. • Shelter-in-place is the preferred option, unless the decision is made by the facility administrator or supervisor, usually in coordination with response agencies, to evacuate, consider the circumstances of the incident, internally or externally and what is best for clients, staff and visitors.
 Facility Notification to Shelter in Place • Reverse 911 recorded message • Emergency Alert System (EAS) through the radio or television • Community Sirens • News media • Weather Radios such as NOAA
Facility Notification to Shelter in Place • Reverse 911 recorded message • Emergency Alert System (EAS) through the radio or television • Community Sirens • News media • Weather Radios such as NOAA
 Interpretative Guidelines E-024 Use of Volunteers • The use of volunteers in an emergency including the process and role for integration of State and Federally designated health care professionals to address surge needs during an emergency. • Facilities are expected to include in its emergency plan a method for contacting off-duty staff during an emergency and procedures to address other contingencies in the event staff are not able to report to duty which may include, but are not limited to, utilizing staff from other facilities and state or federallydesignated health professionals. Survey Procedures • Verify the facility has included policies and procedures for the use of volunteers and other staffing strategies in its emergency plan.
Interpretative Guidelines E-024 Use of Volunteers • The use of volunteers in an emergency including the process and role for integration of State and Federally designated health care professionals to address surge needs during an emergency. • Facilities are expected to include in its emergency plan a method for contacting off-duty staff during an emergency and procedures to address other contingencies in the event staff are not able to report to duty which may include, but are not limited to, utilizing staff from other facilities and state or federallydesignated health professionals. Survey Procedures • Verify the facility has included policies and procedures for the use of volunteers and other staffing strategies in its emergency plan.
 Policies Recommeded • Shelter in Place Policy • Policy on the use of volunteers • Lockdown Procedure for all doors and windows • Facility notification • Assess Staffing Needs for next X hours • On-going assessment of situation and possible relocations within facility due to hazards to interior rooms or off-site
Policies Recommeded • Shelter in Place Policy • Policy on the use of volunteers • Lockdown Procedure for all doors and windows • Facility notification • Assess Staffing Needs for next X hours • On-going assessment of situation and possible relocations within facility due to hazards to interior rooms or off-site
 Interpretative Guidelines E-025 MOU/Transfer Agreements • Facilities are required to have policies and procedures which include prearranged agreements with other facilities and providers to receive residents • Additionally, the policies and procedures and facility agreements should include pre-arranged agreements for transportation between the facilities. • The arrangements should be in writing, such as Memorandums of Understanding (MOUs) and Transfer Agreements, in order to demonstrate compliance.
Interpretative Guidelines E-025 MOU/Transfer Agreements • Facilities are required to have policies and procedures which include prearranged agreements with other facilities and providers to receive residents • Additionally, the policies and procedures and facility agreements should include pre-arranged agreements for transportation between the facilities. • The arrangements should be in writing, such as Memorandums of Understanding (MOUs) and Transfer Agreements, in order to demonstrate compliance.
 MOUs Recommended • Local hospitals for patient transfer, supplies, equipment, pharmaceuticals and personnel. • Local nurse registry agencies, temporary agencies, and security personnel providers • Other local healthcare providers including clinics and long term care facilities for personnel, supplies, equipment and transportation • Vendors and suppliers for healthcare and non-health care resources including linen and fuel • County government for services including transportation and security; for supplies; and for assistance in managing the treatment and transportation of staff and patients.
MOUs Recommended • Local hospitals for patient transfer, supplies, equipment, pharmaceuticals and personnel. • Local nurse registry agencies, temporary agencies, and security personnel providers • Other local healthcare providers including clinics and long term care facilities for personnel, supplies, equipment and transportation • Vendors and suppliers for healthcare and non-health care resources including linen and fuel • County government for services including transportation and security; for supplies; and for assistance in managing the treatment and transportation of staff and patients.
 Survey Procedures E-025 MOU/Transfer Agreements • Ask to see copies of the arrangements and/or any agreements the facility has with other facilities to receive residents in the event the facility is not able to care for them during an emergency. • Ask facility leadership to explain the arrangements in place for transportation in the event of an evacuation.
Survey Procedures E-025 MOU/Transfer Agreements • Ask to see copies of the arrangements and/or any agreements the facility has with other facilities to receive residents in the event the facility is not able to care for them during an emergency. • Ask facility leadership to explain the arrangements in place for transportation in the event of an evacuation.
 CMS Emerge Life Safety ncy Code 2012 Preparedness Healthcare Code 2012
CMS Emerge Life Safety ncy Code 2012 Preparedness Healthcare Code 2012
 Interpretative Guidelines E-041 Emergency Power System Must implement the emergency power system inspection, testing, and maintenance requirements found in the NFPA 99 Health Care Facilities Code, NFPA 110, and Life Safety Code Emergency and standby power systems • An EES includes an alternate source of power, distribution system, and associated equipment. The EES alternate source of power for these facility types is typically a generator. • Emergency preparedness policies and procedures. • NFPA 99 contains emergency power requirements for emergency lighting, fire detection systems, extinguishing systems, and alarm systems.
Interpretative Guidelines E-041 Emergency Power System Must implement the emergency power system inspection, testing, and maintenance requirements found in the NFPA 99 Health Care Facilities Code, NFPA 110, and Life Safety Code Emergency and standby power systems • An EES includes an alternate source of power, distribution system, and associated equipment. The EES alternate source of power for these facility types is typically a generator. • Emergency preparedness policies and procedures. • NFPA 99 contains emergency power requirements for emergency lighting, fire detection systems, extinguishing systems, and alarm systems.
 Survey Procedures E-041 Emergency generator location • NFPA 110 contains minimum requirements and considerations for the installation and environmental conditions that may have an effect equipment, including, building type, classification of occupancy, hazard of contents, and geographic location. NFPA 110 requires that EPSS equipment, including generators, to be designed and located to minimize damage (e. g. , flooding). Emergency generator inspection and testing • NFPA 110 contains routine maintenance and operational testing requirements for emergency and standby power systems, including generators. Emergency generators required by NFPA 99 and the Emergency Preparedness Final Rule must be maintained and tested in accordance with NFPA 110 requirements, which are based on manufacture recommendations
Survey Procedures E-041 Emergency generator location • NFPA 110 contains minimum requirements and considerations for the installation and environmental conditions that may have an effect equipment, including, building type, classification of occupancy, hazard of contents, and geographic location. NFPA 110 requires that EPSS equipment, including generators, to be designed and located to minimize damage (e. g. , flooding). Emergency generator inspection and testing • NFPA 110 contains routine maintenance and operational testing requirements for emergency and standby power systems, including generators. Emergency generators required by NFPA 99 and the Emergency Preparedness Final Rule must be maintained and tested in accordance with NFPA 110 requirements, which are based on manufacture recommendations
 Survey Procedures E-041 Emergency generator fuel • Generators required by NFPA 99 are designated by Class, which defines the minimum time, in hours, that an EES is designed to operate at its rated load without having to be refueled Survey Procedures • Verify that the facility has the required emergency and standby power systems to meet the requirements of the facility’s emergency plan and corresponding policies and procedures • Verify that the onsite fuel source maintains for their generator, and have a plan for how to keep the generator operational during an emergency, unless they plan to evacuate.
Survey Procedures E-041 Emergency generator fuel • Generators required by NFPA 99 are designated by Class, which defines the minimum time, in hours, that an EES is designed to operate at its rated load without having to be refueled Survey Procedures • Verify that the facility has the required emergency and standby power systems to meet the requirements of the facility’s emergency plan and corresponding policies and procedures • Verify that the onsite fuel source maintains for their generator, and have a plan for how to keep the generator operational during an emergency, unless they plan to evacuate.
 LSC Documentation Facility Layout Features of fire protection - sprinklers and doors NFPA 99 Risk Assessment Emergency Battery Lighting • Monthly 30 sec. test • Annual 90 min. test Fire/Smoke Dampers • Test and lube every 4 yrs. Fire Door Inspection – Annual Electrical Equipment – Annual PM Fire Alarm • Monthly Fire Alarm Inspection • Quarterly, semi-annual and annual testing • Batteries every 4 yrs.
LSC Documentation Facility Layout Features of fire protection - sprinklers and doors NFPA 99 Risk Assessment Emergency Battery Lighting • Monthly 30 sec. test • Annual 90 min. test Fire/Smoke Dampers • Test and lube every 4 yrs. Fire Door Inspection – Annual Electrical Equipment – Annual PM Fire Alarm • Monthly Fire Alarm Inspection • Quarterly, semi-annual and annual testing • Batteries every 4 yrs.
 Fire Pump •") LSC Documentation Fire Drills • Monthly (one/month, per shift, per quarter) Fire Pump • Weekly, Monthly, Annual Generator • Weekly • Monthly • Load Bank (if necessary) • 36 month exercise Non-Hospital Grade Electrical Plug Inspection Annual Hood Suppression • Monthly inspection • Semi-annual Circuit Breaker ITM In-services -Annual
LSC Documentation Fire Drills • Monthly (one/month, per shift, per quarter) Fire Pump • Weekly, Monthly, Annual Generator • Weekly • Monthly • Load Bank (if necessary) • 36 month exercise Non-Hospital Grade Electrical Plug Inspection Annual Hood Suppression • Monthly inspection • Semi-annual Circuit Breaker ITM In-services -Annual
 LSC Documentation Sprinkler System Misc. Items • Pressure gauges readings • Elevator state certificate/ recorded weekly/dry Annual PM • Pressure gauges readings • Boiler certificate monthly/wet • Fire hydrant • Quarterly and Annual • HVAC Annual PM • Annual head inspection • 5 yr. internal inspection Facility Policies Smoke detectors • Fire - Evacuation • At install, year and every 2 • Fire Drill - Procedures years • Fire Watch • Smoking
LSC Documentation Sprinkler System Misc. Items • Pressure gauges readings • Elevator state certificate/ recorded weekly/dry Annual PM • Pressure gauges readings • Boiler certificate monthly/wet • Fire hydrant • Quarterly and Annual • HVAC Annual PM • Annual head inspection • 5 yr. internal inspection Facility Policies Smoke detectors • Fire - Evacuation • At install, year and every 2 • Fire Drill - Procedures years • Fire Watch • Smoking
 Training and Testing • CMS is requiring that a facility develop and maintain an emergency preparedness training and testing program. • The training program must include initial training for new staff as well as on-going training for existing staff in emergency preparedness • Facilities must offer annual emergency preparedness training so that staff can demonstrate knowledge of emergency procedures. • Facilities must also conduct drills and exercises to test the emergency plan to identify gaps and areas for improvement.
Training and Testing • CMS is requiring that a facility develop and maintain an emergency preparedness training and testing program. • The training program must include initial training for new staff as well as on-going training for existing staff in emergency preparedness • Facilities must offer annual emergency preparedness training so that staff can demonstrate knowledge of emergency procedures. • Facilities must also conduct drills and exercises to test the emergency plan to identify gaps and areas for improvement.
 CMS Training and Testing – Definitions • Facility-Based: When discussing the terms “all-hazards approach” and facility-based risk assessments, we consider the term “facility-based” to mean that the emergency preparedness program is specific to the facility. • Full-Scale Exercise: A full scale exercise is a multi-agency, multijurisdictional, multi-discipline exercise involving functional (for example, joint field office, emergency operation centers, etc. ) and/or ‘‘boots on the ground’’ response (for example, firefighters decontaminating mock victims). • Table-top Exercise (TTX): A table-top exercise is a group discussion led by a facilitator, using narrated, clinically- relevant emergency scenario, and a set of problem statements, directed messages, or prepared questions designed to challenge an emergency plan. It involves key personnel discussing simulated scenarios. TTXs can be used to assess plans, policies, and procedures.
CMS Training and Testing – Definitions • Facility-Based: When discussing the terms “all-hazards approach” and facility-based risk assessments, we consider the term “facility-based” to mean that the emergency preparedness program is specific to the facility. • Full-Scale Exercise: A full scale exercise is a multi-agency, multijurisdictional, multi-discipline exercise involving functional (for example, joint field office, emergency operation centers, etc. ) and/or ‘‘boots on the ground’’ response (for example, firefighters decontaminating mock victims). • Table-top Exercise (TTX): A table-top exercise is a group discussion led by a facilitator, using narrated, clinically- relevant emergency scenario, and a set of problem statements, directed messages, or prepared questions designed to challenge an emergency plan. It involves key personnel discussing simulated scenarios. TTXs can be used to assess plans, policies, and procedures.
 Interpretative Guidelines E-036 Training and Testing Program Preparedness training and testing program must reflect the risks identified in the facility’s risk assessment and be included in their emergency plan. Training refers education and instruction to staff, contractors, and facility volunteers to ensure all individuals are aware of the emergency preparedness program. Survey Procedures • Verify that the facility has a written training and testing program • Verify the program has been reviewed and updated on, at least, an annual basis
Interpretative Guidelines E-036 Training and Testing Program Preparedness training and testing program must reflect the risks identified in the facility’s risk assessment and be included in their emergency plan. Training refers education and instruction to staff, contractors, and facility volunteers to ensure all individuals are aware of the emergency preparedness program. Survey Procedures • Verify that the facility has a written training and testing program • Verify the program has been reviewed and updated on, at least, an annual basis
 Interpretative Guidelines E-037 Training and Exercises • Provide initial training for new and existing staff, individuals providing services and volunteers. This includes agency nursing staff and any other individuals who provide services on an intermittent basis. Facilities should provide initial emergency training during orientation. • Facilities must maintain documentation of the annual training for all staff. The method chosen is likely based on the training delivery method. For example: computer-based or printed self- learning packets may contain a test to demonstrate knowledge. If facilities choose instructor-led training, a question and answer session could follow the training.
Interpretative Guidelines E-037 Training and Exercises • Provide initial training for new and existing staff, individuals providing services and volunteers. This includes agency nursing staff and any other individuals who provide services on an intermittent basis. Facilities should provide initial emergency training during orientation. • Facilities must maintain documentation of the annual training for all staff. The method chosen is likely based on the training delivery method. For example: computer-based or printed self- learning packets may contain a test to demonstrate knowledge. If facilities choose instructor-led training, a question and answer session could follow the training.
 Survey Procedures E-037 Training and Exercises • Ask for copies of the facility’s initial emergency preparedness training and annual emergency preparedness training offerings. • Interview various staff and ask questions regarding the facility’s initial and annual training course, to verify staff knowledge of emergency procedures. • Review a sample of staff training files to verify staff have received initial and annual emergency preparedness training.
Survey Procedures E-037 Training and Exercises • Ask for copies of the facility’s initial emergency preparedness training and annual emergency preparedness training offerings. • Interview various staff and ask questions regarding the facility’s initial and annual training course, to verify staff knowledge of emergency procedures. • Review a sample of staff training files to verify staff have received initial and annual emergency preparedness training.
 Interpretative Guidelines E-039 Training and Exercises • Conduct exercises to test the emergency plan at least annually • May include unannounced drills using the emergency procedures. • Participate in a exercises that are either community-based or facility-based. • A tabletop exercise that includes a group discussion led by a facilitator, using a narrated, clinically-relevant emergency scenario, and a set of problem statements, directed messages, or prepared questions designed to challenge an emergency plan.
Interpretative Guidelines E-039 Training and Exercises • Conduct exercises to test the emergency plan at least annually • May include unannounced drills using the emergency procedures. • Participate in a exercises that are either community-based or facility-based. • A tabletop exercise that includes a group discussion led by a facilitator, using a narrated, clinically-relevant emergency scenario, and a set of problem statements, directed messages, or prepared questions designed to challenge an emergency plan.
 Interpretative Guidelines E-039 • This means facilities are expected to have completed the following by 11/15/17: • Conduct an additional exercise that may include, but is not limited to the following: • A full-scare exercise that is a multi-agency, multijurisdictional, multi-discipline exercise involving functional and/or ‘‘boots on the ground’’ response • A second full-scale exercise that is individual, facility- based OR • A tabletop exercise that includes a group discussion led by a facilitator, using a narrated, clinically-relevant emergency scenario, and a set of problem statements, directed messages, or prepared questions designed to challenge an emergency plan.
Interpretative Guidelines E-039 • This means facilities are expected to have completed the following by 11/15/17: • Conduct an additional exercise that may include, but is not limited to the following: • A full-scare exercise that is a multi-agency, multijurisdictional, multi-discipline exercise involving functional and/or ‘‘boots on the ground’’ response • A second full-scale exercise that is individual, facility- based OR • A tabletop exercise that includes a group discussion led by a facilitator, using a narrated, clinically-relevant emergency scenario, and a set of problem statements, directed messages, or prepared questions designed to challenge an emergency plan.
 Interpretative Guidelines E-039 • Complete an after action review process to help them develop an actionable after action report (AAR). The process includes a ‘hot wash’ (roundtable discussion) can identify and document lessons learned and necessary improvements in an official AAR. • The AAR, at a minimum, should determine • What happened • What was supposed to happen; • What went well • What didn’t • What the facility can do differently or improve upon • Draft plan with timelines for incorporating necessary improvement. • Actual emergency event or response meets the annual exercise requirements and exempts the facility for engaging in
Interpretative Guidelines E-039 • Complete an after action review process to help them develop an actionable after action report (AAR). The process includes a ‘hot wash’ (roundtable discussion) can identify and document lessons learned and necessary improvements in an official AAR. • The AAR, at a minimum, should determine • What happened • What was supposed to happen; • What went well • What didn’t • What the facility can do differently or improve upon • Draft plan with timelines for incorporating necessary improvement. • Actual emergency event or response meets the annual exercise requirements and exempts the facility for engaging in
 Survey Procedures E-039 Drills/ Exercises • Documentation of the annual drills and exercises including tabletops and full scale exercises (which may include, but is not limited to, the exercise plan, the AAR, and any additional documentation used by the facility to support the exercise. • Documentation of the facility’s efforts to identify a fullscale community based exercise if they did not participate in one (i. e. date and personnel and agencies contacted and the reasons for the inability to participate in a community based exercise). • Documentation of the facility’s analysis and response and how the facility updated its emergency program based on this analysis.
Survey Procedures E-039 Drills/ Exercises • Documentation of the annual drills and exercises including tabletops and full scale exercises (which may include, but is not limited to, the exercise plan, the AAR, and any additional documentation used by the facility to support the exercise. • Documentation of the facility’s efforts to identify a fullscale community based exercise if they did not participate in one (i. e. date and personnel and agencies contacted and the reasons for the inability to participate in a community based exercise). • Documentation of the facility’s analysis and response and how the facility updated its emergency program based on this analysis.
 Policies Needed • What organization is the facility working with such as EMA, Coalition or Collaborative • Policy for training staff (orientation and on-going) • Evidence that staff have been trained • Evidence that facility has conducted or participated in two or more full scale exercises (either with other entities or on-site) or table top exercise. • Exercises must have documentation that includes after such things as hot wash discussion and an after action report
Policies Needed • What organization is the facility working with such as EMA, Coalition or Collaborative • Policy for training staff (orientation and on-going) • Evidence that staff have been trained • Evidence that facility has conducted or participated in two or more full scale exercises (either with other entities or on-site) or table top exercise. • Exercises must have documentation that includes after such things as hot wash discussion and an after action report
 Train and Prepare • Start now!! • Be realistic about your preparations • Write it down • Ensure everyone knows it • Communication is key • Shelter-in-Place Plan • Fire Drills • Evacuation • Missing Resident • Severe weather • Specific emergencies
Train and Prepare • Start now!! • Be realistic about your preparations • Write it down • Ensure everyone knows it • Communication is key • Shelter-in-Place Plan • Fire Drills • Evacuation • Missing Resident • Severe weather • Specific emergencies
 All Hazards means ALL Hazards!
All Hazards means ALL Hazards!
 Kenneth Daily, LNHA Elder Care Systems Group kenn@qissurvey. com • Consulting and education firm focusing mainly on quality improvement, survey compliance, disaster preparation and facility management. • Disaster preparedness planning • Mock surveys and audits • FSES • Policy and procedure development • Professional development and training
Kenneth Daily, LNHA Elder Care Systems Group kenn@qissurvey. com • Consulting and education firm focusing mainly on quality improvement, survey compliance, disaster preparation and facility management. • Disaster preparedness planning • Mock surveys and audits • FSES • Policy and procedure development • Professional development and training