

dc9cddae5a50d0b0674b2e5cbac08bfb.ppt
- Количество слайдов: 42
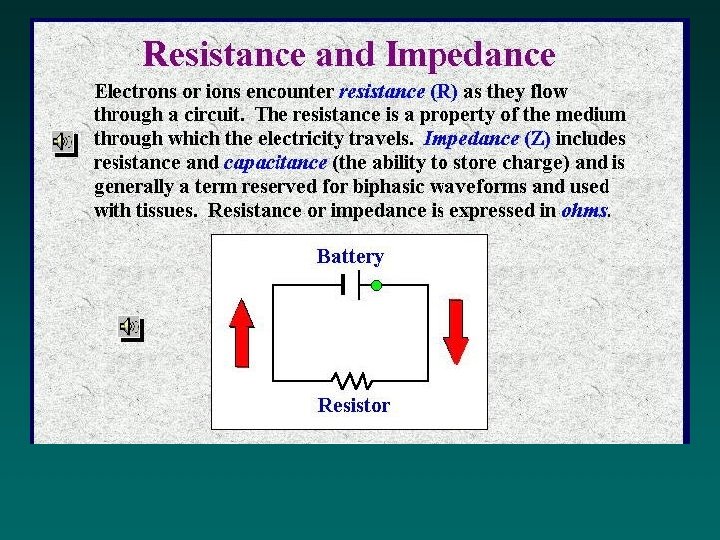
 is the safe and competent use of electrical current") Electrotherapy (aka. clinical electrophysiological intervention) is the safe and competent use of electrical current for a therapeutic purpose.
Electrotherapy (aka. clinical electrophysiological intervention) is the safe and competent use of electrical current for a therapeutic purpose.
 APTA HOUSE OF DELEGATES POLICY APTA website: APTA Leadership; Policies & Bylaws, Section I POSITION ON EXCLUSIVE USE OF PHYSICAL AGENTS / MODALITIES - HOD 06 -95 -29 -18 It is the position of the American Physical Therapy Association (APTA) that physical agents/modalities should be utilized only as a component of patient management. Without documentation which justifies the necessity of the exclusive use of physical agents/modalities, the use of physical agents/modalities, in the absence of other skilled therapeutic or educational interventions, should not be considered physical therapy.
APTA HOUSE OF DELEGATES POLICY APTA website: APTA Leadership; Policies & Bylaws, Section I POSITION ON EXCLUSIVE USE OF PHYSICAL AGENTS / MODALITIES - HOD 06 -95 -29 -18 It is the position of the American Physical Therapy Association (APTA) that physical agents/modalities should be utilized only as a component of patient management. Without documentation which justifies the necessity of the exclusive use of physical agents/modalities, the use of physical agents/modalities, in the absence of other skilled therapeutic or educational interventions, should not be considered physical therapy.
 Electricity Knowledge Map
Electricity Knowledge Map
 Identifying type, form, and descriptive characteristics • Phases: number of; applies to Pulsed Current only • Symmetry: are the phases mirror images? (size and shape) • Balance: is the area under each (+) and (-) phase equal? (eg. amount of charge)
Identifying type, form, and descriptive characteristics • Phases: number of; applies to Pulsed Current only • Symmetry: are the phases mirror images? (size and shape) • Balance: is the area under each (+) and (-) phase equal? (eg. amount of charge)
 Practice using the Descriptive Characteristics of Electrical Pulses
Practice using the Descriptive Characteristics of Electrical Pulses
 Quantitative Characteristics of Pulsed Currents
Quantitative Characteristics of Pulsed Currents
 Effects of changing Amplitude, Width, and Rate
Effects of changing Amplitude, Width, and Rate
 Electrical Stimulation of Tissues • • • Conductivity of tissues Directional flow of current in tissues Excitable tissues in the body and comparable thresholds
Electrical Stimulation of Tissues • • • Conductivity of tissues Directional flow of current in tissues Excitable tissues in the body and comparable thresholds
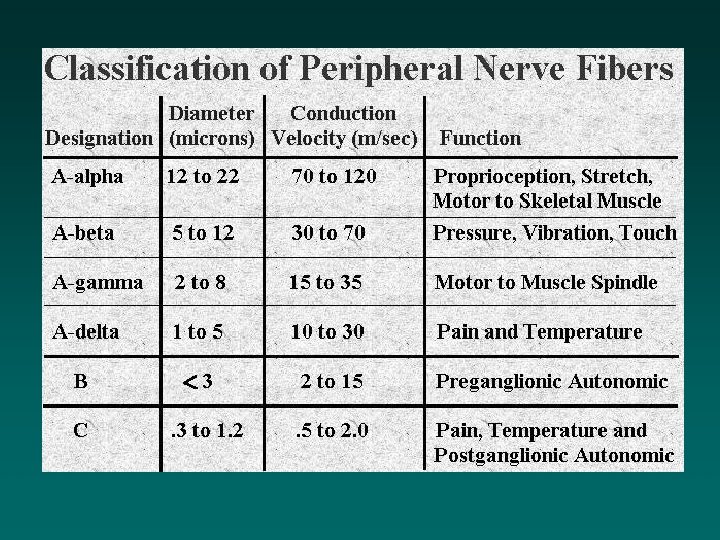
 More. . Classification of peripheral nerve fibers
More. . Classification of peripheral nerve fibers
 and Duration (width)") Strength (amplitude) and Duration (width)
Strength (amplitude) and Duration (width)
 Electrode Arrangement Terminology: Monopolar Placement Bipoloar Placement Quadpolar Placement
Electrode Arrangement Terminology: Monopolar Placement Bipoloar Placement Quadpolar Placement
 Current Density Issues visualize the 3 -D electrical field and how the field-density changes based on these factors: amplitude, width, Hz, electrode size, distance btwn electrodes, electrode contact (pressure) Depth of Current Penetration All else being equal, depth of penetration is Increased by: Increasing the amplitude, Increasing distance between electrodes, or Decreasing pulse duration.
Current Density Issues visualize the 3 -D electrical field and how the field-density changes based on these factors: amplitude, width, Hz, electrode size, distance btwn electrodes, electrode contact (pressure) Depth of Current Penetration All else being equal, depth of penetration is Increased by: Increasing the amplitude, Increasing distance between electrodes, or Decreasing pulse duration.
 What’s the target with NMES?
What’s the target with NMES?
 Classic Responses all apply
Classic Responses all apply
 Motor Responses are KEY
Motor Responses are KEY
 Electrode Size & Placement :
Electrode Size & Placement :
 Electrode Placement Figure 12 -05. Electrodes placed over the proximal and distal ends of the quadriceps muscles 20 maximum for efficacy.
Electrode Placement Figure 12 -05. Electrodes placed over the proximal and distal ends of the quadriceps muscles 20 maximum for efficacy.
 Voluntary vs. Electrically Induced Muscle Contractions • 2 main differences related to recruitment: – Order of recruitment of motor nerve fibers and muscle fiber types. SIZE PRINCIPLE – Pattern of recruitment of motor nerve fibers Physiologically initiated contraction Electrically stimulated contraction Muscle fiber type Slow twitch type I first Fast twitch type II first Contraction force Low High Speed of contraction Slow Fast Fatigue resistant Fatigues quickly Atrophy resistant Atrophies quickly Recruitment Asynchronous Synchronous
Voluntary vs. Electrically Induced Muscle Contractions • 2 main differences related to recruitment: – Order of recruitment of motor nerve fibers and muscle fiber types. SIZE PRINCIPLE – Pattern of recruitment of motor nerve fibers Physiologically initiated contraction Electrically stimulated contraction Muscle fiber type Slow twitch type I first Fast twitch type II first Contraction force Low High Speed of contraction Slow Fast Fatigue resistant Fatigues quickly Atrophy resistant Atrophies quickly Recruitment Asynchronous Synchronous
 Clinical Implication & Application of Order or Recruitment Differences • NMES can be more effective at specifically strengthening muscle fibers weakened by disuse. Why? • If possible, patients should perform both stimulated and voluntary exercises to optimize functional integration of strength gains. Why? • Since NMES contractions are more fatiguing than voluntary contractions, long rest times should be provided between contractions.
Clinical Implication & Application of Order or Recruitment Differences • NMES can be more effective at specifically strengthening muscle fibers weakened by disuse. Why? • If possible, patients should perform both stimulated and voluntary exercises to optimize functional integration of strength gains. Why? • Since NMES contractions are more fatiguing than voluntary contractions, long rest times should be provided between contractions.
 Types of pulsed currents approp for NMES Russian Pulsed Current: a strong polyphasic pulse that is balanced & symmetrical. internal frequency of each pulse is 2500 Hz, which only gives one nerve depolarization; It is totally different than Burst on a TENS unit.
Types of pulsed currents approp for NMES Russian Pulsed Current: a strong polyphasic pulse that is balanced & symmetrical. internal frequency of each pulse is 2500 Hz, which only gives one nerve depolarization; It is totally different than Burst on a TENS unit.
 Types of pulsed currents approp for NMES Biphasic Pulsed Current: same as what we used with TENS; now we will increase the pulse width to 250 us and greater. Common current used on battery operated NMES units
Types of pulsed currents approp for NMES Biphasic Pulsed Current: same as what we used with TENS; now we will increase the pulse width to 250 us and greater. Common current used on battery operated NMES units
 Timing Modes for NMES parameters
Timing Modes for NMES parameters
 Ramp-Surge Mode: Parameters
Ramp-Surge Mode: Parameters
 Ramp-Surge Mode: Parameters
Ramp-Surge Mode: Parameters
 Physiologic Effects of NMES • Increasing vascular flow via ms. pump • Decreasing painful muscle spasm / guarding • Muscle re-education (facilitating innervated ms with impaired motor control); improve motor control • Muscle strengthening or to slow the rate of muscle atrophy • Maintain or increase joint range of motion • Temporarily reduce muscle spasticity / hypertonicity • Act as an orthotic device to improve function at a moveable area. (Functional Electrical Stimulation [FES] ) – State the impairment and treatment goal
Physiologic Effects of NMES • Increasing vascular flow via ms. pump • Decreasing painful muscle spasm / guarding • Muscle re-education (facilitating innervated ms with impaired motor control); improve motor control • Muscle strengthening or to slow the rate of muscle atrophy • Maintain or increase joint range of motion • Temporarily reduce muscle spasticity / hypertonicity • Act as an orthotic device to improve function at a moveable area. (Functional Electrical Stimulation [FES] ) – State the impairment and treatment goal
 Example NMES setups
Example NMES setups
 Example NMES setups
Example NMES setups
 Example NMES setups
Example NMES setups
 Example NMES setups
Example NMES setups
 Example NMES setups
Example NMES setups
 Relating Muscle Fatigue and NMES Parameters
Relating Muscle Fatigue and NMES Parameters
 NMES summary Rx chart
NMES summary Rx chart
 Cameron’s NMES summary Rx chart
Cameron’s NMES summary Rx chart
 Discussion of NMES • Strengthening muscle with NMES • NMES for Muscle Facilitation / Re-education. – To Strengthen or Re-educate, that is often the Question. • NMES for Temporary reduction/fatigue of muscle spasticity (hypertonicity) due to upper motor neuron lesion • Additional advanced uses of NMES
Discussion of NMES • Strengthening muscle with NMES • NMES for Muscle Facilitation / Re-education. – To Strengthen or Re-educate, that is often the Question. • NMES for Temporary reduction/fatigue of muscle spasticity (hypertonicity) due to upper motor neuron lesion • Additional advanced uses of NMES
 US / E-stim Combo
US / E-stim Combo
 CASE: Patient is a 36 yo male with thoracic & lumbar back pain bilaterally (rated 3/10); worse with movement (rated 6/10). Onset 4 days ago from a MVA. Erector spinae muscle spasms are tender to palpation bilaterally from ~T 8 to L 4 and trunk motion is limited. There is some pain also thru the right buttock and down the right proximal posterior thigh. Score on the Modified Oswestry is 22/50 (44/100). Rx: NMES? ?
CASE: Patient is a 36 yo male with thoracic & lumbar back pain bilaterally (rated 3/10); worse with movement (rated 6/10). Onset 4 days ago from a MVA. Erector spinae muscle spasms are tender to palpation bilaterally from ~T 8 to L 4 and trunk motion is limited. There is some pain also thru the right buttock and down the right proximal posterior thigh. Score on the Modified Oswestry is 22/50 (44/100). Rx: NMES? ?
 CASE: Patient is a 22 yo male who was in a motorcycle accident 3 days ago which severely damaged the soft tissue of the R foot (from malleoli down) and fractured ribs and wrist on the left. No fractures of the foot appeared on plain film radiographs; foot lacerations were sutured and severe abrasions are bandaged. Motions of the toes and ankle are limited and painful. The foot and ankle region is significantly swollen. Patient is brought to OP PT for wound care and Rx for all impairments. VAS rating of the foot pain is 8/10. He says the entire foot hurts. Rx: NMES ? ?
CASE: Patient is a 22 yo male who was in a motorcycle accident 3 days ago which severely damaged the soft tissue of the R foot (from malleoli down) and fractured ribs and wrist on the left. No fractures of the foot appeared on plain film radiographs; foot lacerations were sutured and severe abrasions are bandaged. Motions of the toes and ankle are limited and painful. The foot and ankle region is significantly swollen. Patient is brought to OP PT for wound care and Rx for all impairments. VAS rating of the foot pain is 8/10. He says the entire foot hurts. Rx: NMES ? ?