

ed295448c133de678902cdef9f65ed4c.ppt
- Количество слайдов: 104
 Echo Essentials for TAVI Steven A. Goldstein, MD Director, Noninvasive Cardiology Washington Hospital Center Sunday, February 27, 2011
Echo Essentials for TAVI Steven A. Goldstein, MD Director, Noninvasive Cardiology Washington Hospital Center Sunday, February 27, 2011
 DISCLOSURE I have N O relevant financial relationships
DISCLOSURE I have N O relevant financial relationships
 Severe Aortic Stenosis One of the most lethal of all cardiovascular diseases
Severe Aortic Stenosis One of the most lethal of all cardiovascular diseases
 Percutaneous/Transapical AVR Team Approach • Interventional cardiologist • Imaging cardiologist • Vascular surgeons • Cardiac surgeons • Anesthesiologists
Percutaneous/Transapical AVR Team Approach • Interventional cardiologist • Imaging cardiologist • Vascular surgeons • Cardiac surgeons • Anesthesiologists
 TEE in Cath Lab: Set-up O 2 SUCTION Nurse Operator Tech Echocardiographer Monitors
TEE in Cath Lab: Set-up O 2 SUCTION Nurse Operator Tech Echocardiographer Monitors
 Percutaneous AV Replacement Role of Pre-Procedure Echo • Determine severity of aortic stenosis • Assess aortic valve morphology • Estimate annular size • Distance from valve to L-main orifice • Discovery of severe aortic atheroma (may mandate transapical approach)
Percutaneous AV Replacement Role of Pre-Procedure Echo • Determine severity of aortic stenosis • Assess aortic valve morphology • Estimate annular size • Distance from valve to L-main orifice • Discovery of severe aortic atheroma (may mandate transapical approach)
 Percutaneous AV Replacement Role of On-Line TEE • Reassess annular diameter critical for sizing • Monitor deployment of valve (verify correct positioning) co-axial alignment (detect impingement on coronaries) • Assess severity and location of AR • Assess leaflet motion of the deployed valve • Measure gradients (transgastric views) • Detect new regional WMAs • Detection of complications
Percutaneous AV Replacement Role of On-Line TEE • Reassess annular diameter critical for sizing • Monitor deployment of valve (verify correct positioning) co-axial alignment (detect impingement on coronaries) • Assess severity and location of AR • Assess leaflet motion of the deployed valve • Measure gradients (transgastric views) • Detect new regional WMAs • Detection of complications
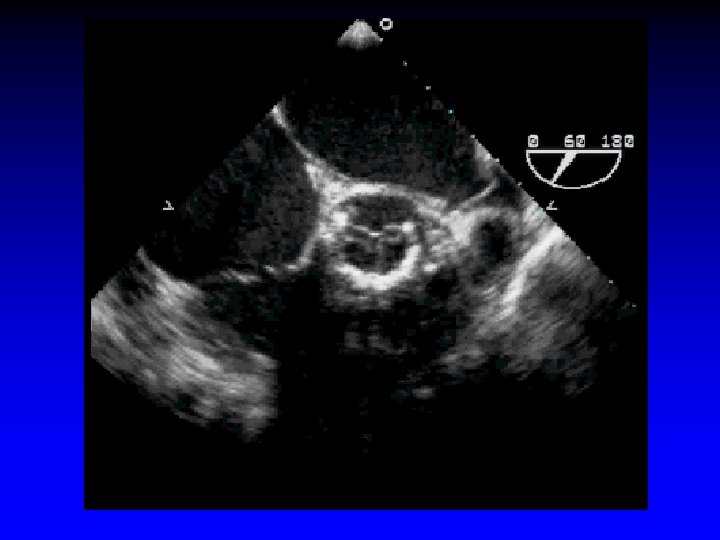
 1. 8 cm Measurement of aortic annulus
1. 8 cm Measurement of aortic annulus
 1. 8 cm Measurement of aortic annulus
1. 8 cm Measurement of aortic annulus
 Percutaneous AV Replacement Role of On-Line TEE • Reassess annular diameter critical for sizing • Monitor deployment of valve (verify correct positioning) co-axial alignment (detect impingement on coronaries) • Assess severity and location of AR • Assess leaflet motion of the deployed valve • Measure gradients (transgastric views) • Detect new regional WMAs • Detection of complications
Percutaneous AV Replacement Role of On-Line TEE • Reassess annular diameter critical for sizing • Monitor deployment of valve (verify correct positioning) co-axial alignment (detect impingement on coronaries) • Assess severity and location of AR • Assess leaflet motion of the deployed valve • Measure gradients (transgastric views) • Detect new regional WMAs • Detection of complications
 Percutaneous AV Replacement Complications • Vascular complications • Stroke • Dislodgement of aortic atheroma • Thrombus formation of catheters, wires, etc • Valve migration • Myocardial ischemia from coronary obstruction • Damage to mitral valve • AV block
Percutaneous AV Replacement Complications • Vascular complications • Stroke • Dislodgement of aortic atheroma • Thrombus formation of catheters, wires, etc • Valve migration • Myocardial ischemia from coronary obstruction • Damage to mitral valve • AV block
 Percutaneous AV Replacement Role of On-Line TEE Additional Miscellaneous Issues • Sigmoid septum • MV structure, function, calcification • LV apical thrombus • Occurrence of thrombi on catheters • Wire not through mitral apparatus
Percutaneous AV Replacement Role of On-Line TEE Additional Miscellaneous Issues • Sigmoid septum • MV structure, function, calcification • LV apical thrombus • Occurrence of thrombi on catheters • Wire not through mitral apparatus
 Case 1
Case 1
 95 year-old man mentally clear 2 years ago bowling and yard work Since then, progressive effort angina and dyspnea “Burning” and pressure with exertion Now NYHA class III-IV
95 year-old man mentally clear 2 years ago bowling and yard work Since then, progressive effort angina and dyspnea “Burning” and pressure with exertion Now NYHA class III-IV

 Vmax = 4. 3 m/s peak instantaneous gradient = 74 mm Hg
Vmax = 4. 3 m/s peak instantaneous gradient = 74 mm Hg


 23 mm balloon 25 mm balloon
23 mm balloon 25 mm balloon
 51 cm/sec LAD flow velocity pre transcatheter AV replacement
51 cm/sec LAD flow velocity pre transcatheter AV replacement
 63 cm/sec LAD flow velocity post transcatheter AV replacement
63 cm/sec LAD flow velocity post transcatheter AV replacement
 Pre Post
Pre Post
 This 95 year-old man has returned to bowling !
This 95 year-old man has returned to bowling !
 LA LV Coaxial No tc oa xia l
LA LV Coaxial No tc oa xia l
 LA LV proximal distal
LA LV proximal distal
 Case 2 Case 7
Case 2 Case 7
 Percutaneous Aortic Valve Replacement a. AV placed to avoid impingement on coronary ostia or to impeded motion of anterior mitral leaflet b. Prosthesis deployed by inflating the delivery balloon c. Balloon is deflated and rapidly withdrwan
Percutaneous Aortic Valve Replacement a. AV placed to avoid impingement on coronary ostia or to impeded motion of anterior mitral leaflet b. Prosthesis deployed by inflating the delivery balloon c. Balloon is deflated and rapidly withdrwan
 Make sure wire does not interfere with mitral apparatus
Make sure wire does not interfere with mitral apparatus
 Case 3 Case 7
Case 3 Case 7
 Transapical approach - wire not thru mitral apparatus
Transapical approach - wire not thru mitral apparatus
 Balloon valvuloplasty
Balloon valvuloplasty
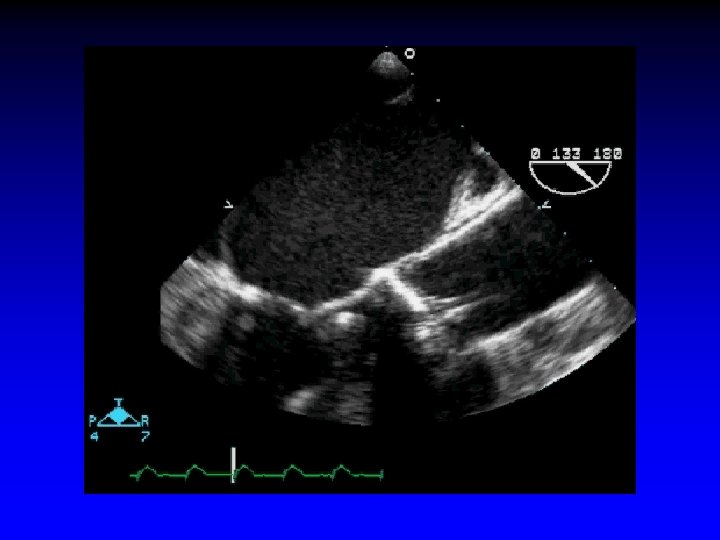
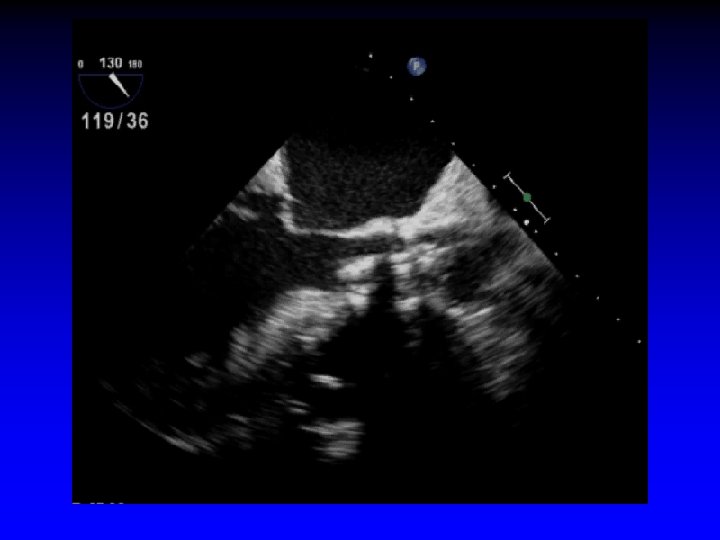
 Pre-deployment - valve in good position
Pre-deployment - valve in good position
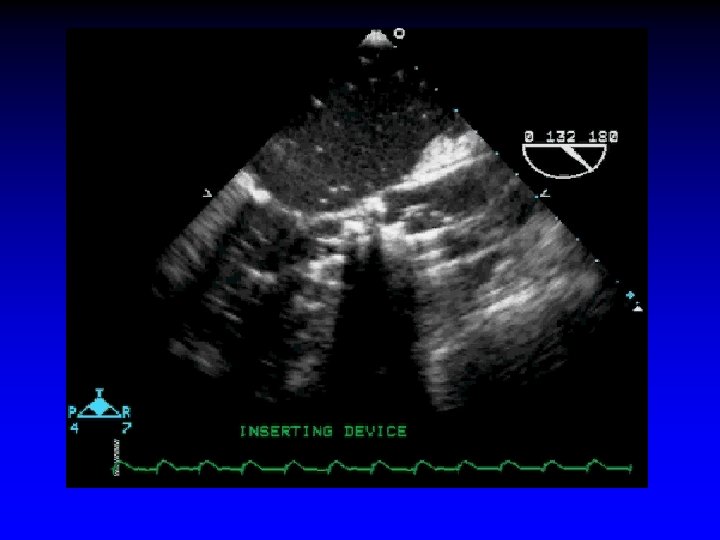
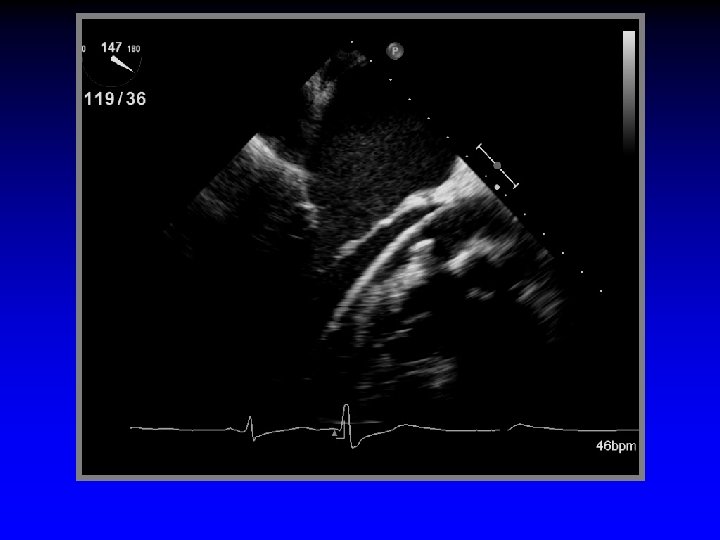
 Deployment of valve
Deployment of valve
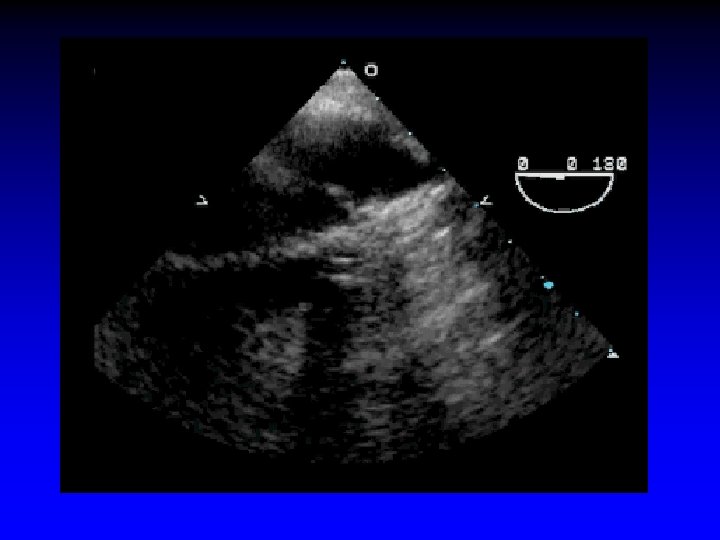
 Valve deployed - good position
Valve deployed - good position
 Case 4 Case 7
Case 4 Case 7
") Valve deployed - slightly “aortic” (too high)
Valve deployed - slightly “aortic” (too high)
 Case 5 Case 7
Case 5 Case 7
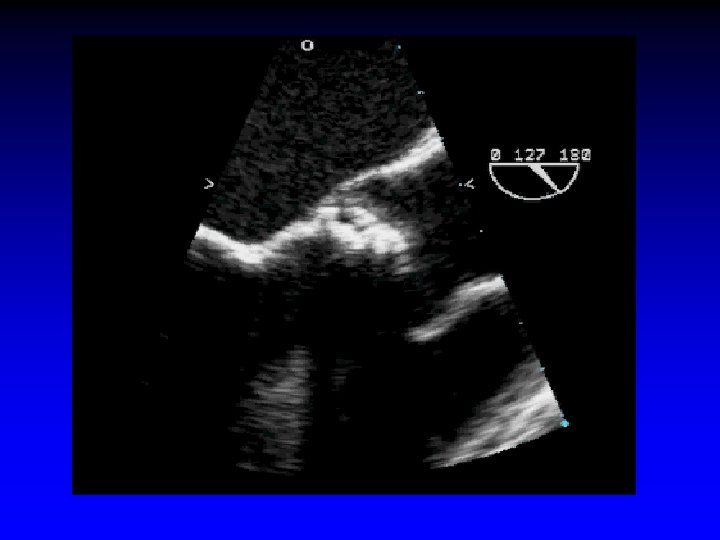
 Wire passing through mitral apparatus
Wire passing through mitral apparatus
 Wire passing through mitral apparatus
Wire passing through mitral apparatus
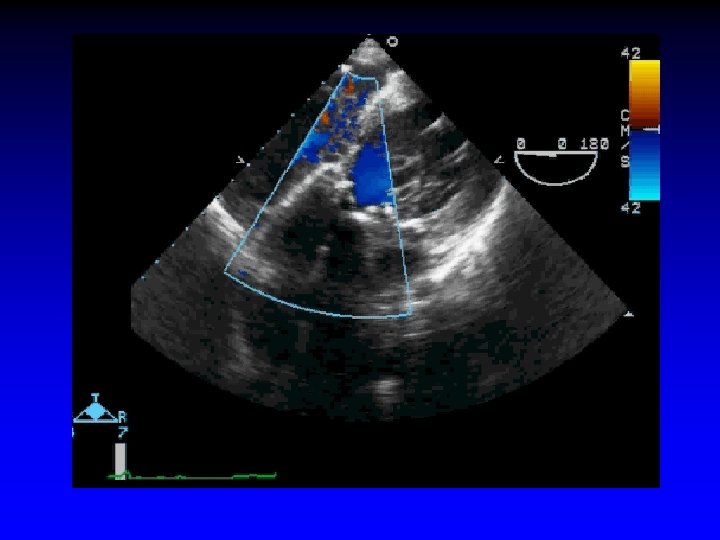
 Wire withdrawn and re-inserted now “safe”
Wire withdrawn and re-inserted now “safe”
 Potential problem Now OK
Potential problem Now OK
 Case 6 Case 7
Case 6 Case 7
 Mobile thrombus in descending thoracic aorta
Mobile thrombus in descending thoracic aorta
 Mobile thrombus in aortic arch
Mobile thrombus in aortic arch
 Case 7
Case 7
 SK - 67 year old lawyer Severe aortic stenosis Symptomatic dyspnea and angina Successful transcatheter deployment of #26 Edwards-Sapien prosthetic aortic valve Post-procedure R-hemiparesis
SK - 67 year old lawyer Severe aortic stenosis Symptomatic dyspnea and angina Successful transcatheter deployment of #26 Edwards-Sapien prosthetic aortic valve Post-procedure R-hemiparesis
 J Am Coll Cardiol 2008; 51: 579") Different Shapes of Stent Deployment Zegdi (Paris) J Am Coll Cardiol 2008; 51: 579 -84
Different Shapes of Stent Deployment Zegdi (Paris) J Am Coll Cardiol 2008; 51: 579 -84
") Sharp Calcific Excrescenses Crossing the Stent Frame Protrude Inside the Aortic Lumen Zegdi (Paris) J Am Coll Cardiol 2008; 51: 579 -84
Sharp Calcific Excrescenses Crossing the Stent Frame Protrude Inside the Aortic Lumen Zegdi (Paris) J Am Coll Cardiol 2008; 51: 579 -84
 Influence of Size or Shape of the Orifice On the Valved Stent Deployment Zegdi (Paris) J Am Coll Cardiol 2008; 51: 579 -84
Influence of Size or Shape of the Orifice On the Valved Stent Deployment Zegdi (Paris) J Am Coll Cardiol 2008; 51: 579 -84
 Leaflet Distortion in the Presence of Annular Calcification Close to One Commissure of the Deployed Valved Stent Zegdi (Paris) J Am Coll Cardiol 2008; 51: 579 -84
Leaflet Distortion in the Presence of Annular Calcification Close to One Commissure of the Deployed Valved Stent Zegdi (Paris) J Am Coll Cardiol 2008; 51: 579 -84
") Valve Distortion Secondary to the Valved Stent Deployment Inside a Triangular Orifice Zegdi (Paris) J Am Coll Cardiol 2008; 51: 579 -84
Valve Distortion Secondary to the Valved Stent Deployment Inside a Triangular Orifice Zegdi (Paris) J Am Coll Cardiol 2008; 51: 579 -84
") Stent Shapes after Deployment According to Aortic Valve Pathology Tricuspid Bicuspid (n = 19) Circular n (%) 13 (68) 2 (14) Elliptic n (%) 2 (11) 11 (79) Triangular n (%) 4 (21) Zegdi (Paris) J Am Coll Cardiol 2008; 51: 579 -84 1 (7)
Stent Shapes after Deployment According to Aortic Valve Pathology Tricuspid Bicuspid (n = 19) Circular n (%) 13 (68) 2 (14) Elliptic n (%) 2 (11) 11 (79) Triangular n (%) 4 (21) Zegdi (Paris) J Am Coll Cardiol 2008; 51: 579 -84 1 (7)

 80 Valve Replacement 60") Symptomatic Aortic Stenosis AVR Must Be Performed 100 Survival (%) 80 Valve Replacement 60 40 No surgery 20 P<0. 05 0 0 1 P<0. 001 2 3 Years Schwartz Circulation 1982; 66: 1105 -10 Chi 2 = 23. 5 P<0. 001 4 5
Symptomatic Aortic Stenosis AVR Must Be Performed 100 Survival (%) 80 Valve Replacement 60 40 No surgery 20 P<0. 05 0 0 1 P<0. 001 2 3 Years Schwartz Circulation 1982; 66: 1105 -10 Chi 2 = 23. 5 P<0. 001 4 5
 Based on estimated") Incidence of Aortic Stenosis for Population > 65 Population (x 106) Based on estimated population growth projection data from US census 2. 00 1. 80 1. 60 1. 40 1. 20 1. 00 0. 80 0. 60 0. 40 0. 20 0. 00 2010 2020 2030 2040 Year US Census Bureau. US Interim Projections by Age, Sex, Race, and Hispanic Origin. In 2004. 2050
Incidence of Aortic Stenosis for Population > 65 Population (x 106) Based on estimated population growth projection data from US census 2. 00 1. 80 1. 60 1. 40 1. 20 1. 00 0. 80 0. 60 0. 40 0. 20 0. 00 2010 2020 2030 2040 Year US Census Bureau. US Interim Projections by Age, Sex, Race, and Hispanic Origin. In 2004. 2050
 Aortic Valve Replacement • Increasing need over next 10 years - Aging population - Increase of world population - Under-diagnosed in upcoming countries (China, India)
Aortic Valve Replacement • Increasing need over next 10 years - Aging population - Increase of world population - Under-diagnosed in upcoming countries (China, India)
 Transcatheter Percutaneous Aortic Valve Replacement A driving force for catheter-based therapies for valvular heart disease since mid-1980 s Pioneered the development of Cribier-Edwards heart valve Performed the first PTAVR in 2002 Alain Cribier Rouen, France
Transcatheter Percutaneous Aortic Valve Replacement A driving force for catheter-based therapies for valvular heart disease since mid-1980 s Pioneered the development of Cribier-Edwards heart valve Performed the first PTAVR in 2002 Alain Cribier Rouen, France
 Percutaneous Aortic Valves • Core. Valve, Inc • Edwards-Sapien Edwards Life Sciences • Direct Flow Medical, Inc • Lotus Sadra Medical • Paniagua Endoluminal Technology Research • Enable ATS • Perceval Sorin Group • Jena Valve technology
Percutaneous Aortic Valves • Core. Valve, Inc • Edwards-Sapien Edwards Life Sciences • Direct Flow Medical, Inc • Lotus Sadra Medical • Paniagua Endoluminal Technology Research • Enable ATS • Perceval Sorin Group • Jena Valve technology
 Placement of Ao. RTic Tra. Nscathet. ER Valves Trial PARTNER Trial
Placement of Ao. RTic Tra. Nscathet. ER Valves Trial PARTNER Trial
 PARTNER - Algorithm Severe AS - symptomatic High Risk Patient Operable High Risk Percutaneous AVR Non-operable Percutaneous AVR Surgery High Risk Medical Therapy
PARTNER - Algorithm Severe AS - symptomatic High Risk Patient Operable High Risk Percutaneous AVR Non-operable Percutaneous AVR Surgery High Risk Medical Therapy
 Percutaneous Aortic Valve Indications • Severe AS from degenerative disease • Symptomatic • Aortic valve area <0. 8 cm 2 and Vmax >4. 0 m/s or mean gradient > 40 mm Hg • Surgical mortality > 20%
Percutaneous Aortic Valve Indications • Severe AS from degenerative disease • Symptomatic • Aortic valve area <0. 8 cm 2 and Vmax >4. 0 m/s or mean gradient > 40 mm Hg • Surgical mortality > 20%
 Edwards SAPIEN™ THV using the Retro. Flex 3™ Transfemoral Delivery System Procedural Steps Balloon Valvuloplasty Aortic Arch Navigation Native valve crossing Valve deployment Final assesment
Edwards SAPIEN™ THV using the Retro. Flex 3™ Transfemoral Delivery System Procedural Steps Balloon Valvuloplasty Aortic Arch Navigation Native valve crossing Valve deployment Final assesment
 Edwards SAPIEN™ THV using the Ascendra™ Transapical Delivery System Direct access the apex Balloon valvuloplasty Native valve crossing Valve deployment Procedure steps Final assesment
Edwards SAPIEN™ THV using the Ascendra™ Transapical Delivery System Direct access the apex Balloon valvuloplasty Native valve crossing Valve deployment Procedure steps Final assesment
 Valve before deployment
Valve before deployment
 Valve after deployment
Valve after deployment


 Transcatheter AV Replacement Rapidly Emerging Field • Improving technology • Improved patient selection • Growing procedural experience
Transcatheter AV Replacement Rapidly Emerging Field • Improving technology • Improved patient selection • Growing procedural experience
 Transcatheter AV Replacement Progress with Successive Device Generations - Core Valve 1 st 2 nd 3 rd (25 -F) (21 -F) (18 -F) Procedure success rate 70% 71% 91% Periprocedural mortality 10% 8% 0% Periprocedural stroke rate 10% Grube Circulation Cardiovasc Intervent 2008; 1; 167 -75 <5%
Transcatheter AV Replacement Progress with Successive Device Generations - Core Valve 1 st 2 nd 3 rd (25 -F) (21 -F) (18 -F) Procedure success rate 70% 71% 91% Periprocedural mortality 10% 8% 0% Periprocedural stroke rate 10% Grube Circulation Cardiovasc Intervent 2008; 1; 167 -75 <5%
 Next-Generation Transfemoral Valve Delivery System Retro. Flex • • • Retro. Flex II Offers: Greatly improved native valve crossability Smoother tracking Improved handle functionality Fewer system components Continued advancement of the THV Program
Next-Generation Transfemoral Valve Delivery System Retro. Flex • • • Retro. Flex II Offers: Greatly improved native valve crossability Smoother tracking Improved handle functionality Fewer system components Continued advancement of the THV Program
 Conclusions • Marked hemodynamic and clinical improvement • Careful selection and screening essential • TEE important role during procedure • Procedural success rate ≈ 90% (closely linked to experience) • At present, only short-term results
Conclusions • Marked hemodynamic and clinical improvement • Careful selection and screening essential • TEE important role during procedure • Procedural success rate ≈ 90% (closely linked to experience) • At present, only short-term results


 Case 57
Case 57
 DR - 85 year-old woman Longstanding aortic stenosis Felt not to be surgical candidate due to multiple medical problems and small size Entered PARTNER Trial and randomized to receive transcatheter prosthetic aortic valve Transapical due to small femoral arteries
DR - 85 year-old woman Longstanding aortic stenosis Felt not to be surgical candidate due to multiple medical problems and small size Entered PARTNER Trial and randomized to receive transcatheter prosthetic aortic valve Transapical due to small femoral arteries
 Valve positioned properly
Valve positioned properly
 Valve deployed properly
Valve deployed properly
 42 cm/sec Coronary flow pre-procedure
42 cm/sec Coronary flow pre-procedure
 68 cm/sec
68 cm/sec
 Case 8 Case 7
Case 8 Case 7
 History • 85 year-old man with aortic stenosis, mild CAD, and PVD complained of shortness of breath with minimal exertion.
History • 85 year-old man with aortic stenosis, mild CAD, and PVD complained of shortness of breath with minimal exertion.
 LVOTD=2. 0 cm Ao Valve Area = 0. 8 cm 2 V 2=4. 1 m/s V 1=1. 1 m/s
LVOTD=2. 0 cm Ao Valve Area = 0. 8 cm 2 V 2=4. 1 m/s V 1=1. 1 m/s
 After deployment of 23 mm Edwards-Sapien aortic valve
After deployment of 23 mm Edwards-Sapien aortic valve
 Reason……
Reason……
 Patient’s blood pressure decreased from 170/69 to 93/32 mm. Hg
Patient’s blood pressure decreased from 170/69 to 93/32 mm. Hg
 Decision was made to place nd valve inside the 1 st valve. 2
Decision was made to place nd valve inside the 1 st valve. 2
 Deployment of 2 nd valve inside the 1 st valve
Deployment of 2 nd valve inside the 1 st valve
 After valve deployment trace aortic regurgitation
After valve deployment trace aortic regurgitation
 Confucius said…… “If at first you don’t succeed, try and try again. ”
Confucius said…… “If at first you don’t succeed, try and try again. ”
 ECHO
ECHO
 Transcatheter AV Repalcement Edwards-Sapien Valve Successful deployment 87% 30 -day mortality 7. 4% Major adverse cardiac event rate Tops, Kapadia, Tuzcu, Vahanian, Alfieri, Webb, Bax Current Problems in Cardiology 2008; 33 A: 415 -57 16. 7%
Transcatheter AV Repalcement Edwards-Sapien Valve Successful deployment 87% 30 -day mortality 7. 4% Major adverse cardiac event rate Tops, Kapadia, Tuzcu, Vahanian, Alfieri, Webb, Bax Current Problems in Cardiology 2008; 33 A: 415 -57 16. 7%
 Aortic Valve Replacement Percutaneous Approach • General anesthesia or awake patients • Avoids surgery • Steep learning curve • Still experimental
Aortic Valve Replacement Percutaneous Approach • General anesthesia or awake patients • Avoids surgery • Steep learning curve • Still experimental
 Edwards-Sapien Valve Balloon expandable Stainless steel stent Fabric sealing cuff Bovine pericardial leaflets Two sizes: New height 23 mm 26 mm
Edwards-Sapien Valve Balloon expandable Stainless steel stent Fabric sealing cuff Bovine pericardial leaflets Two sizes: New height 23 mm 26 mm
 Core. Valve Prosthesis Self expanding Nitinol alloy stent Porcine pericardial leaflets Pericardial sealing cuff 50 mm long Waist in the middle part Two sizes: 26 mm 29 mm
Core. Valve Prosthesis Self expanding Nitinol alloy stent Porcine pericardial leaflets Pericardial sealing cuff 50 mm long Waist in the middle part Two sizes: 26 mm 29 mm