3f323f75fe439ded3bb86703be04ccf6.ppt
- Количество слайдов: 33



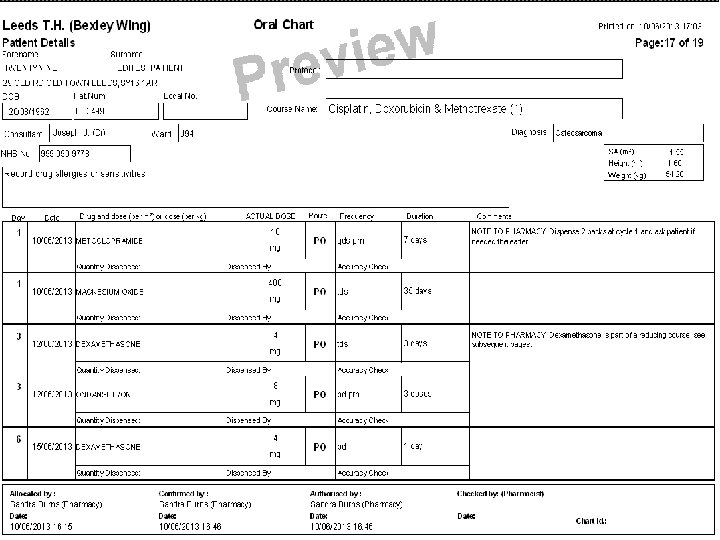
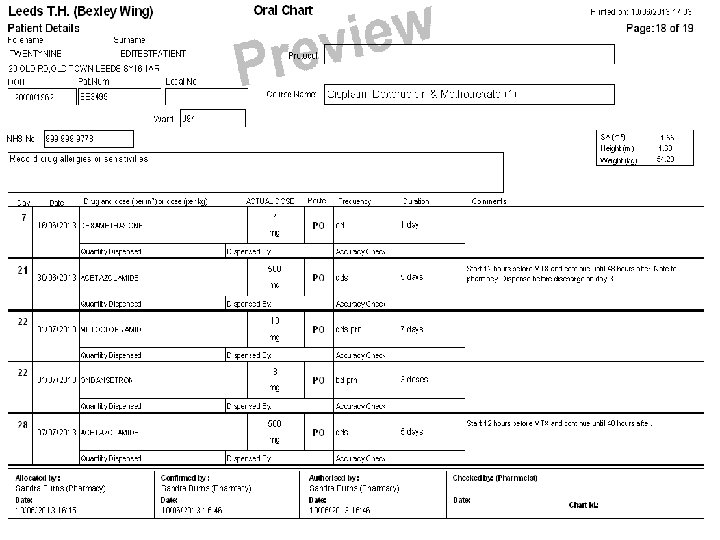
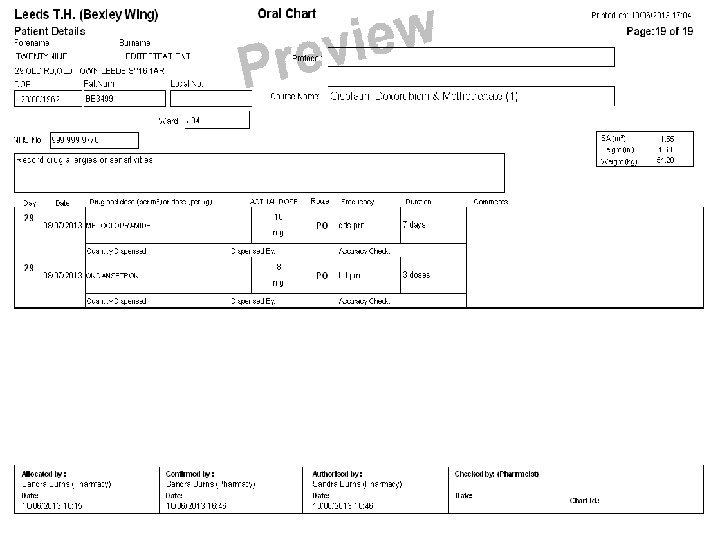
e. Prescribing of Chemotherapy The Leeds Experience Julie Mansell, Lead Chemotherapy Pharmacist, Leeds Cancer Centre

Background at Leeds Teaching Hospitals • SJUH Opmas 1993 • Cookridge Design partners – Chemocare® 1995 • Introduced to breast cancer clinic, gradual rollout • Cookridge site → oncology SJUH, haematology • 60+ consultants • 5000 patients per annum • Oncology, haematology, BMT, trials including early phase • Treatment given orally, day case, in-patient and ambulatory • All chemotherapy prescribed using Chemocare®

Improved safety 2006 Journal of Quality and Safety in Healthcare “Effect of computerisation on the quality and safety of chemotherapy prescription” • Oncology centre in Lausanne • Examined chemotherapy errors before and after implementation • Classification of errors Major = drug name, dose, route of administration • Before 141 errors in 940 prescriptions (19% major) • After 6 errors in 978 prescriptions (0% major) Error rate reduced from 15% to 0. 6% Marc Voeffray et al. Effect of computerisation on the quality and safety of chemotherapy prescription Qual. Saf. Health Care 2006; 15; 418 -421

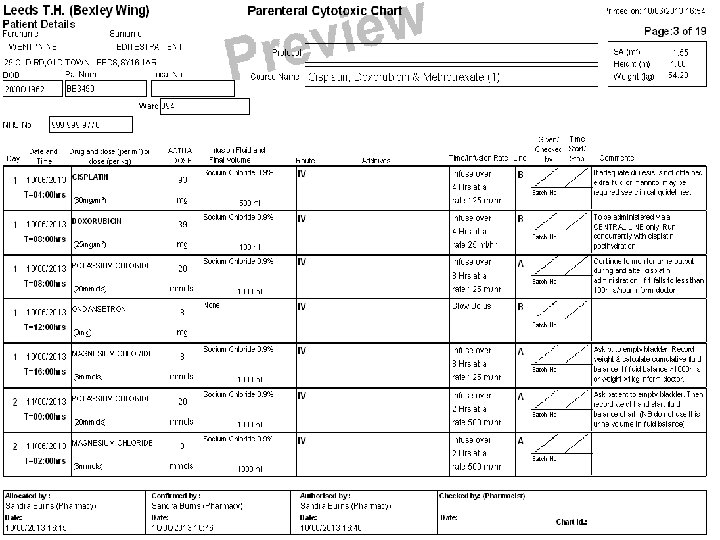
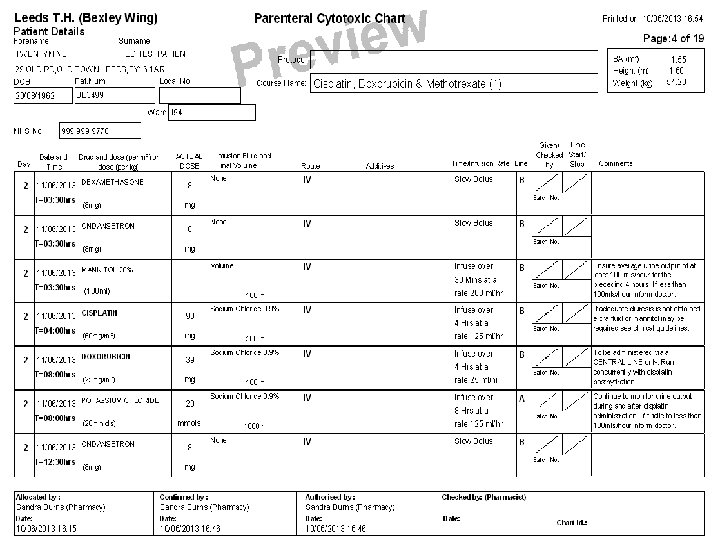
Complex prescribing – ideal target • Narrow therapeutic index and highly toxic– potential for harm is great • Wide range of doses e. g. Methotrexate 10 mg to 12 g/m 2 • Dose, interval, route varies with tumour type • Dosed on BSA, weight, fixed • Several medicines in most regimens • Supportive medicines to deliver safely • Multiple day treatment with different medicines on different days • BEP – Bleomycin D 2, 8, 15 Etoposide D 1, 2 3 Cisplatin D 1, 2 • Modifications for myelosuppression, renal + liver impairment frequent • Common use of acronyms • Classes of agents with very different uses e. g. rituximab/trastuzumab

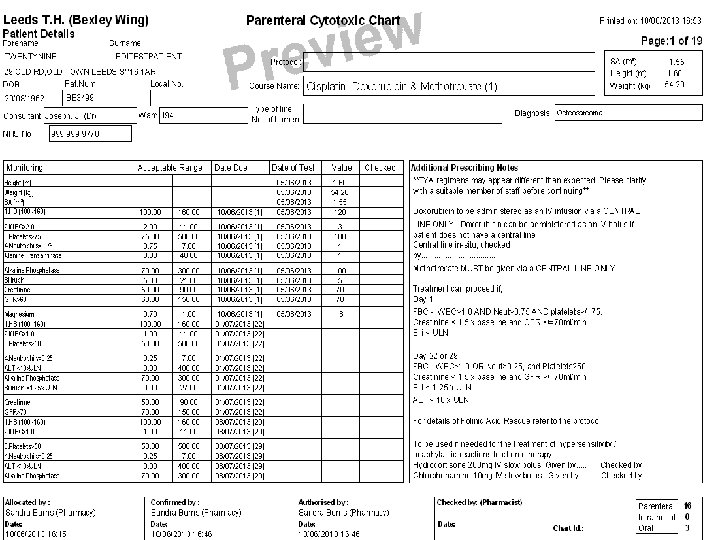
National Drivers • Manual for Cancer Services Rolling quality assurance programme for cancer services Purpose - enables quality improvement both in terms of clinical and patient outcomes 2004 -2007 40% e. Prescribing • Chemotherapy Services in England: Ensuring quality and safety National Chemotherapy Advisory Group 2009 Group established to advise DH on development + delivery of high quality chemotherapy services “Handwritten prescriptions for parenteral chemotherapy should be replaced as soon as possible by pre-printed forms or, preferably, by fully validated electronic prescribing systems” • Chemotherapy measures 2011 11 -3 S-139 to 142 Electronic Prescribing – covers criteria for system and SOP’s
 • Reduces prescription errors • Legible • Faster for complex")
Benefits and successes (1) • Reduces prescription errors • Legible • Faster for complex treatment
 Quality assurance • Consistency of prescribing • Controls access to")
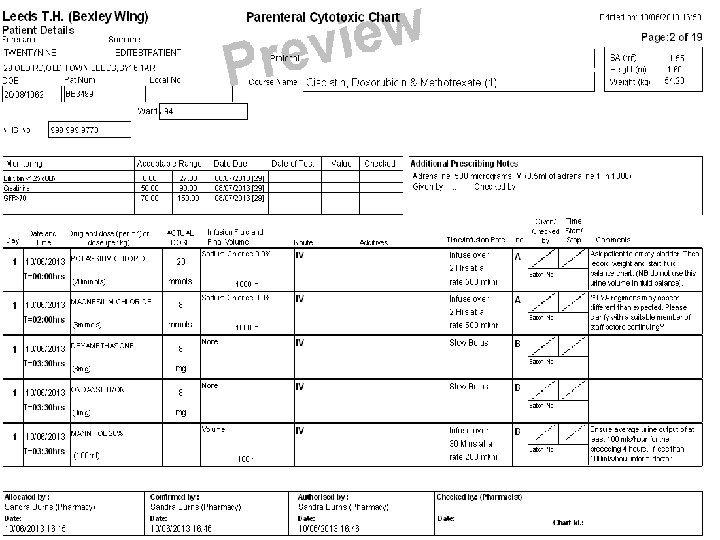
Benefits and Successes (2) Quality assurance • Consistency of prescribing • Controls access to protocol for certain diseases only • Central control of change • Set maximum doses/ routes that cannot be overwritten • Reduces variation in clinical practice • Template sign-off by consultant, 2 pharmacists • Calculation of patient variables e. g. GFR, BSA
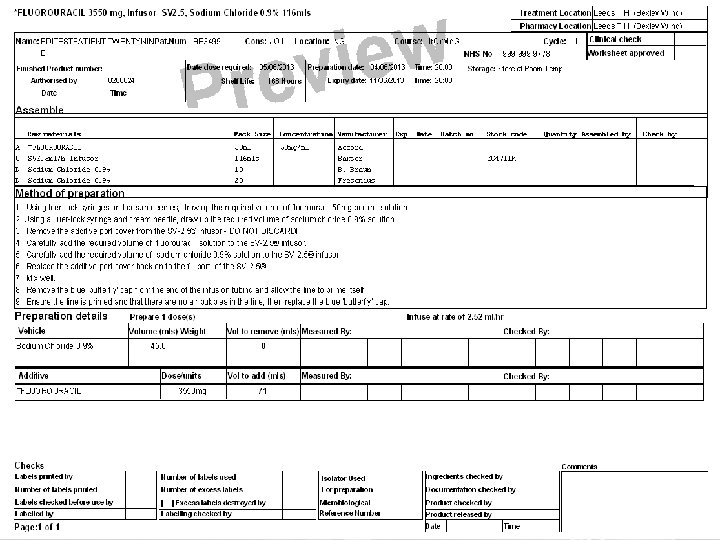
 Pharmacy specific • Integrated worksheet and label preparation • Automatic")
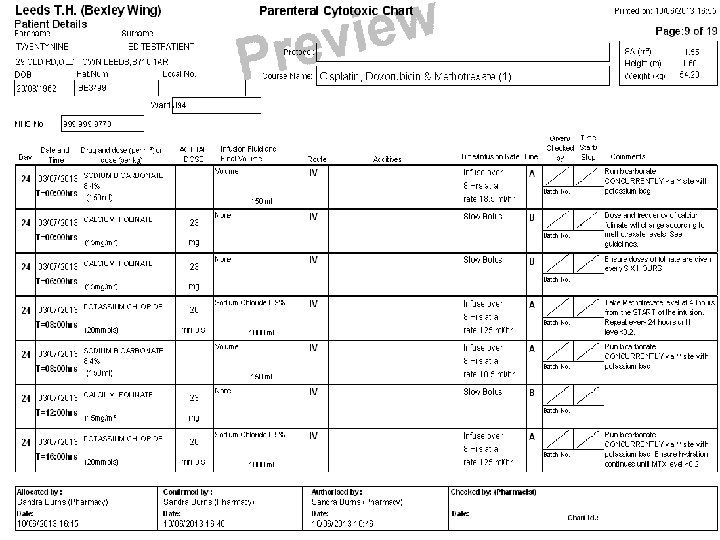
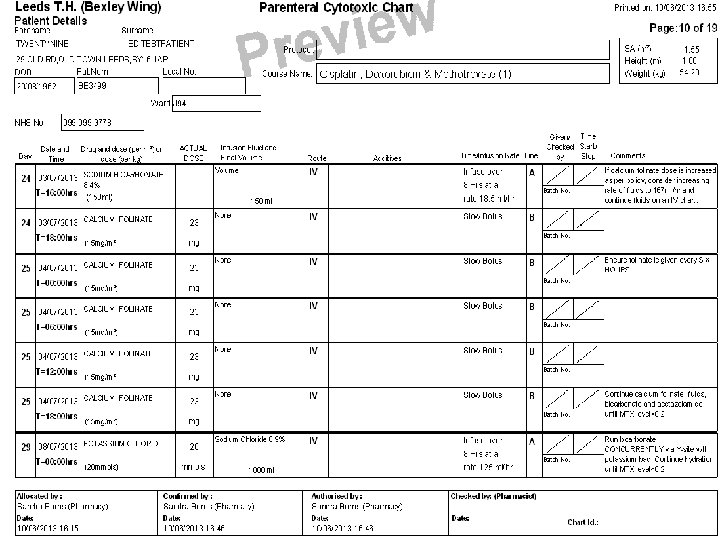
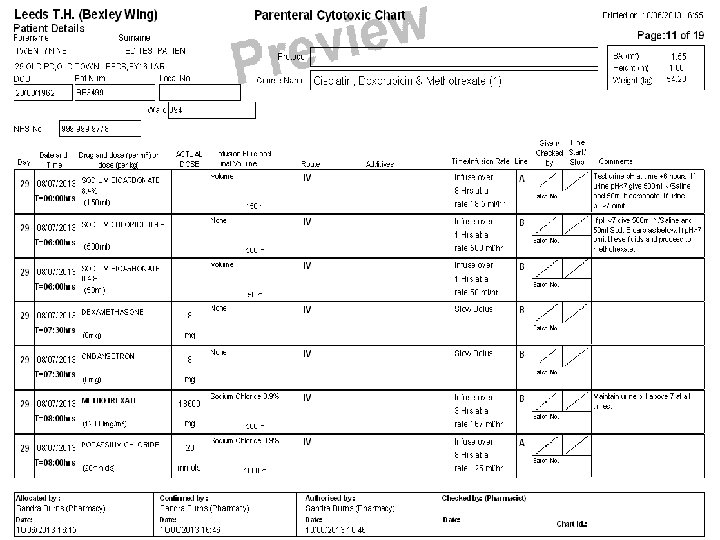
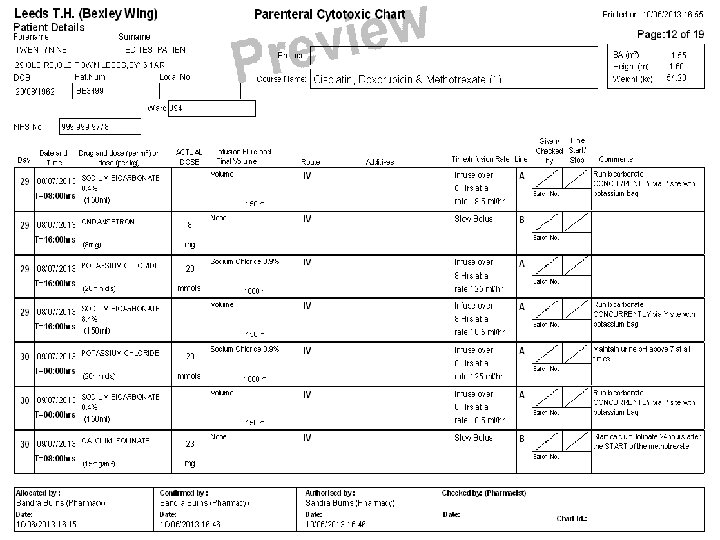
Benefits and Successes (3) Pharmacy specific • Integrated worksheet and label preparation • Automatic dose rounding RAPID RESPONSE REPORT NPSA/2008/RRR 04 “Doses of vinca alkaloids should be prepared for use by dilution in small volume intravenous bags, rather than in syringes”

Additional benefits • Audit and review of practice • Identifies case series for research projects • SACT dataset • Facilitates service re-design • Improves prescribing efficiency in clinic • Easily accessible treatment view on admission

Specific Challenges/Limitations Reluctance/resistance to change • Technophobes! • Age range/ skills of staff across MDT • Slower for simple treatments Find Clinical and Managerial Champions Employ national drivers Promote additional benefits Patience and perseverance! Training burden • Time consuming –start up/new staff/upgrades • Level 1 competency (prescribing scenarios) Employ (if possible) a designated e. Prescribing lead

Specific Challenges/Limitations Loss of knowledge • Doses of chemotherapy never learned • Supportive medicines not appreciated Teach and test the basics Errors • e. Prescribing = different errors ≠ NO errors • If template incorrect - affects multiple patients • Depends on quality of input e. g. 0 mg/ height and weight mistakes Foster a quality culture Check and check again Review common themes

Specific Challenges/Limitations Technical challenges • Difficult to set up templates for complex regimens • Chronomodulation / trial dose bands • National system – unable to make many in-house tweaks • No administration module → paper copy for records Be creative, but maintain safety

Future Challenges Paper-lite • Long established use of prescription as communication tool • Reluctance to change Use clinical (multi-professional) champions Use local drivers – efficiency Project group
3f323f75fe439ded3bb86703be04ccf6.ppt