

be94f57aaaeb8abaf8f700a6984b4a7d.ppt
- Количество слайдов: 33
 Assoc. Prof. Ivan Lambev e-mail: itlambev@mail. bg") Drugs Acting on Respiratory Syste (Summary) Assoc. Prof. Ivan Lambev e-mail: itlambev@mail. bg
Drugs Acting on Respiratory Syste (Summary) Assoc. Prof. Ivan Lambev e-mail: itlambev@mail. bg
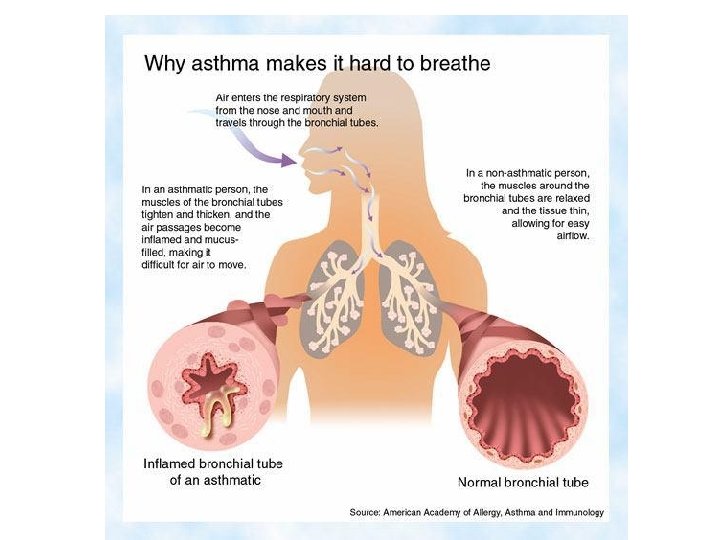
 I. Drug Therapy of Bronchial As The term asthma is derived from the Greek w meaning difficulty in breathing. Asthma is a chronic inflammatory allergic disease: the pat suffer with reversible episodes of airways obs due to bronchial hyper-responsiveness. In the early (acute) phase there are smooth spasm and excessive bronchial secretion of m In the late (chronic or delayed) phase, infla continues, accompanied by fibrosis, oedema necrosis of bronchial epithelial cells.
I. Drug Therapy of Bronchial As The term asthma is derived from the Greek w meaning difficulty in breathing. Asthma is a chronic inflammatory allergic disease: the pat suffer with reversible episodes of airways obs due to bronchial hyper-responsiveness. In the early (acute) phase there are smooth spasm and excessive bronchial secretion of m In the late (chronic or delayed) phase, infla continues, accompanied by fibrosis, oedema necrosis of bronchial epithelial cells.
 FACTORS THAT EXACERBATE ASTHMA
FACTORS THAT EXACERBATE ASTHMA
 The cardinal symptoms of asthma are breathles wheezing, cough and chest tightness with worseni these symptoms at night. In the acute attack there pid respiratory rate and tachycardia. The majority o suffer with atopic extrinsic asthma, which is asso with exposure to specific allergen (pollen or house mite). In non-atopic extrinsic asthma the attack stimulated with some non-specific stimulus, e. g. ch irritants. In such cases, Ig. G and Ig antibodies circu the blood but are not attached to the mast cells or basophils. Neutrophils destroy these antigen-antib complexes. As a result, the liberated lysosomal en
The cardinal symptoms of asthma are breathles wheezing, cough and chest tightness with worseni these symptoms at night. In the acute attack there pid respiratory rate and tachycardia. The majority o suffer with atopic extrinsic asthma, which is asso with exposure to specific allergen (pollen or house mite). In non-atopic extrinsic asthma the attack stimulated with some non-specific stimulus, e. g. ch irritants. In such cases, Ig. G and Ig antibodies circu the blood but are not attached to the mast cells or basophils. Neutrophils destroy these antigen-antib complexes. As a result, the liberated lysosomal en
 can digest the remaining mucoproteins. Drugs w stabilize the lysosomal membrane, e. g. GCS pro relief to these patients. In contrast, the many pat who acquire asthma after the age of 40 years ha identifiable external precipitating factor or immun basis for asthmatic attack. This can be described intrinsic asthma. Many patients suffer from both and intrinsic forms of asthma. In comparison with asthma, extrinsic asthma is episodic and less pro develop into status asthmaticus. Status asthma is a severe acute asthma, which is a life-threaten condition involving exhaustion, cyanosis, bradyc hypotension, dehydration and metabolic acidosis
can digest the remaining mucoproteins. Drugs w stabilize the lysosomal membrane, e. g. GCS pro relief to these patients. In contrast, the many pat who acquire asthma after the age of 40 years ha identifiable external precipitating factor or immun basis for asthmatic attack. This can be described intrinsic asthma. Many patients suffer from both and intrinsic forms of asthma. In comparison with asthma, extrinsic asthma is episodic and less pro develop into status asthmaticus. Status asthma is a severe acute asthma, which is a life-threaten condition involving exhaustion, cyanosis, bradyc hypotension, dehydration and metabolic acidosis
 Cardiac asthma is a bronchospasm precipitat uncompensated congestive heart failure. Pathophysiology of Asthma Antigens (pollen and house-dust mites) sensitize by eliciting the production of Ig. E type of antibodie remain either circulating in the blood or become at the mast cells of nasal or bronchial tissues and ba On re-exposure the same antigen, the resulting an antibody reaction in the early phase causes degra of the lung mast cells and releasing of the powerfu bronchoconstrictors: histamine, 5 -HT, PGD 2 and cysteinyl leucotriens (LTB 4, LTC 4 and LTD 4).
Cardiac asthma is a bronchospasm precipitat uncompensated congestive heart failure. Pathophysiology of Asthma Antigens (pollen and house-dust mites) sensitize by eliciting the production of Ig. E type of antibodie remain either circulating in the blood or become at the mast cells of nasal or bronchial tissues and ba On re-exposure the same antigen, the resulting an antibody reaction in the early phase causes degra of the lung mast cells and releasing of the powerfu bronchoconstrictors: histamine, 5 -HT, PGD 2 and cysteinyl leucotriens (LTB 4, LTC 4 and LTD 4).
 phase") Lung mast cells also release ILs (IL-4, IL-5 and ILIn the late (delayed) phase of asthma, these med activate additional inflammatory cells (eosinophils, basophils, and alveolar macrophages) which also LTs and ILs. Other mediators of inflammation, in delayed phase are: adenosine (causing bronchconstriction), neuro (SP, causing mucus secretion and increase in vas permeability; neurokinin A, causing bronchoconstr PAF etc. The normal tone of bronchial smooth muscle is inf by a balance between parasympathetic, sympathe non-adrenergic–non-cholinergic (NANC) mediator
Lung mast cells also release ILs (IL-4, IL-5 and ILIn the late (delayed) phase of asthma, these med activate additional inflammatory cells (eosinophils, basophils, and alveolar macrophages) which also LTs and ILs. Other mediators of inflammation, in delayed phase are: adenosine (causing bronchconstriction), neuro (SP, causing mucus secretion and increase in vas permeability; neurokinin A, causing bronchoconstr PAF etc. The normal tone of bronchial smooth muscle is inf by a balance between parasympathetic, sympathe non-adrenergic–non-cholinergic (NANC) mediator
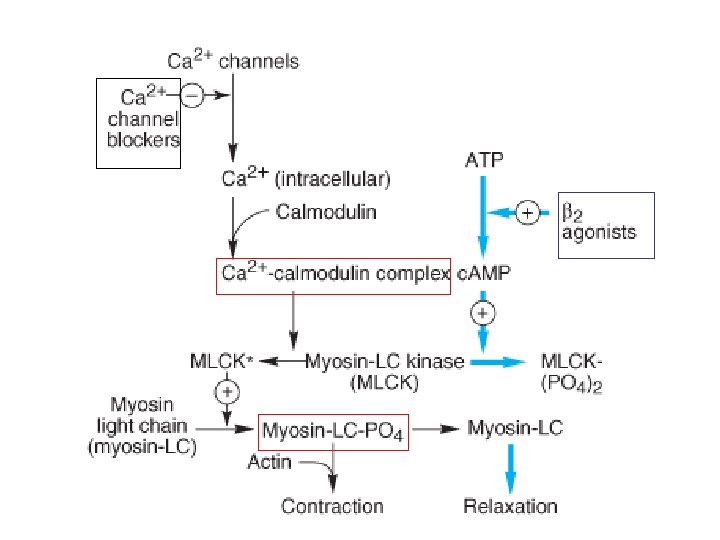
 Activation of M 3 -receptors by the release ACh resu increase in c. GMP levels and leads to bronchocon and increase in mucus secretion. β 2 -receptor stim leads to an increase of c. AMP levels which results bronchodilation. The main NANC inhibitory neurotransmitter is NO The main NANC excitory transmitters are neurop (neurokinin A and SP), released from unmyelinate sensory C-fibres when stimulated by inflammatory mediators and irritant chemicals (SO 2, cigarette sm
Activation of M 3 -receptors by the release ACh resu increase in c. GMP levels and leads to bronchocon and increase in mucus secretion. β 2 -receptor stim leads to an increase of c. AMP levels which results bronchodilation. The main NANC inhibitory neurotransmitter is NO The main NANC excitory transmitters are neurop (neurokinin A and SP), released from unmyelinate sensory C-fibres when stimulated by inflammatory mediators and irritant chemicals (SO 2, cigarette sm
 Classification of Antiasthmatic D 1. Bronchodilators • Selective β 2 -agonists: Clenbuterol, Salbutam Fenoterol, Indacaterol, Levosalbutamol, Salm Terbutaline • Nonselective β-agonists: Epinephrine, Isopr Orciprenaline; Ephedrine • M-cholinolytics: Ipratropium, Tiotropium, Oxi Ox • Methyl Xanthines: Theophylline, Aminophylli Theotard 2. Mast Cell Stabilizers: Sodium Cromoglycate Ketotifen, Nedocromil
Classification of Antiasthmatic D 1. Bronchodilators • Selective β 2 -agonists: Clenbuterol, Salbutam Fenoterol, Indacaterol, Levosalbutamol, Salm Terbutaline • Nonselective β-agonists: Epinephrine, Isopr Orciprenaline; Ephedrine • M-cholinolytics: Ipratropium, Tiotropium, Oxi Ox • Methyl Xanthines: Theophylline, Aminophylli Theotard 2. Mast Cell Stabilizers: Sodium Cromoglycate Ketotifen, Nedocromil
 • • • Oral: Prednisone, Methylprednisolone Parenteral: Methylprednisolone, Betamethasone Inhalational: Beclomethasone,") 3. Glucocorticosteroids (GCS) • • • Oral: Prednisone, Methylprednisolone Parenteral: Methylprednisolone, Betamethasone Inhalational: Beclomethasone, Budenoside, Fluticasone, Triamcinolone 4. Inhalational β 2 -agonists/Glucocorticoste Seretide® (fluticasone/salmeterol) Symbicort® (budenoside/formoterol) 5. Leukotriene Modulators • 5 -Lipoxygenase Inhibitor: Zileuton • LTD 4 -antgonists: Zafirlukast, Montelukast 6. Monoclonal Anti-Ig. E Antibody: Omalizuma 7. Miscellaneous: NO-donors, Calcium antagonis
3. Glucocorticosteroids (GCS) • • • Oral: Prednisone, Methylprednisolone Parenteral: Methylprednisolone, Betamethasone Inhalational: Beclomethasone, Budenoside, Fluticasone, Triamcinolone 4. Inhalational β 2 -agonists/Glucocorticoste Seretide® (fluticasone/salmeterol) Symbicort® (budenoside/formoterol) 5. Leukotriene Modulators • 5 -Lipoxygenase Inhibitor: Zileuton • LTD 4 -antgonists: Zafirlukast, Montelukast 6. Monoclonal Anti-Ig. E Antibody: Omalizuma 7. Miscellaneous: NO-donors, Calcium antagonis
 provide a rapid matic relief but they") Bronchodilators – relievers (β-agonis M-cholinolytics, Methyl Xanthins) provide a rapid matic relief but they do not control the disease pro Selective β 2 -agonists activate β 2 -receptors prese airway smooth muscle and mast cells too. These a relax airway smooth muscle, inhibit the release of bronchoconstricting mediators from the adipocytes and increase the mucociliary transport by increasin mucociliary activity. ADRs: tremor, tachycardia, desensitization/down-r of β 2 -receptors that results in diminished responsiv
Bronchodilators – relievers (β-agonis M-cholinolytics, Methyl Xanthins) provide a rapid matic relief but they do not control the disease pro Selective β 2 -agonists activate β 2 -receptors prese airway smooth muscle and mast cells too. These a relax airway smooth muscle, inhibit the release of bronchoconstricting mediators from the adipocytes and increase the mucociliary transport by increasin mucociliary activity. ADRs: tremor, tachycardia, desensitization/down-r of β 2 -receptors that results in diminished responsiv
 (+) Gs Ex AC In c. AMP PKA ATP Effects") Adrenaline (b 1&b 2) (+) Gs Ex AC In c. AMP PKA ATP Effects
Adrenaline (b 1&b 2) (+) Gs Ex AC In c. AMP PKA ATP Effects
 Beta-2 -agonists are available as metered-dose a Short acting beta-2 agonists: the onset of effect (per inhalation) begins after 3 to 5 min and continues 4– 6 h: • Salbutamol (albuterol) • Fenoterol, Terbutaline Highly lipid, soluble long-acting agents (t 1/2 12 h) Effect: after 15– 20 min, duration 12 h: • Salmeterol, Formoterol
Beta-2 -agonists are available as metered-dose a Short acting beta-2 agonists: the onset of effect (per inhalation) begins after 3 to 5 min and continues 4– 6 h: • Salbutamol (albuterol) • Fenoterol, Terbutaline Highly lipid, soluble long-acting agents (t 1/2 12 h) Effect: after 15– 20 min, duration 12 h: • Salmeterol, Formoterol
") Selective β 2 -adrenomimetics with tocolytic effect • Fenoterol (Partusisten : tab. 5 mg) • Hexoprenaline • Salbutamol (Salbupart ) • Terbutaline
Selective β 2 -adrenomimetics with tocolytic effect • Fenoterol (Partusisten : tab. 5 mg) • Hexoprenaline • Salbutamol (Salbupart ) • Terbutaline
 Anticholinergics in asthma • Ipratropium • Tiotropium Primarily, the site of bronchodilation action of inhaled β 2 agonists is mainly the bronchiolar smooth muscle. Atropi cause bronchodilation by blocking cholinergic constricto act primarily in large airways.
Anticholinergics in asthma • Ipratropium • Tiotropium Primarily, the site of bronchodilation action of inhaled β 2 agonists is mainly the bronchiolar smooth muscle. Atropi cause bronchodilation by blocking cholinergic constricto act primarily in large airways.
 a) inhibit phosphodiesterase III (present in airw muscle) and") Methyl Xanthines (Theophylline, Aminophylline, Theotard) a) inhibit phosphodiesterase III (present in airw muscle) and IV (present in eosinophil and mast c the two specific isoenzymes responsible for the degradation of c. AMP; b) block the adenosine-1 -receptors on airway and adenosine-3 -receptors, present on mast ce The main use of methyl xanthins is in the manag of asthma and COPD (Chronic Obstructive Pulm Disease), usually as combination therapy with beta-2 -agonists.
Methyl Xanthines (Theophylline, Aminophylline, Theotard) a) inhibit phosphodiesterase III (present in airw muscle) and IV (present in eosinophil and mast c the two specific isoenzymes responsible for the degradation of c. AMP; b) block the adenosine-1 -receptors on airway and adenosine-3 -receptors, present on mast ce The main use of methyl xanthins is in the manag of asthma and COPD (Chronic Obstructive Pulm Disease), usually as combination therapy with beta-2 -agonists.
 Glucocorticosteroids provide long-term stabilization of the symptoms due to their anti-infla effects. Inhaled GCS, along with beta-2 -agonists a first choice drugs for chronic asthma. GCS inhibit the release of PGs and LTs and thus p smooth muscle contraction, vascular permeability airway mucus secretion. GCS produce eosinopenia which prevents cytotox of the mediators released from eosinophils. GCS enhance beta-2 -adrenergic response by up-r the beta-2 -receptors in lung cells and leuckocytes. hours are required for DNA transcription and RNA translation to occur after administering GCS.
Glucocorticosteroids provide long-term stabilization of the symptoms due to their anti-infla effects. Inhaled GCS, along with beta-2 -agonists a first choice drugs for chronic asthma. GCS inhibit the release of PGs and LTs and thus p smooth muscle contraction, vascular permeability airway mucus secretion. GCS produce eosinopenia which prevents cytotox of the mediators released from eosinophils. GCS enhance beta-2 -adrenergic response by up-r the beta-2 -receptors in lung cells and leuckocytes. hours are required for DNA transcription and RNA translation to occur after administering GCS.
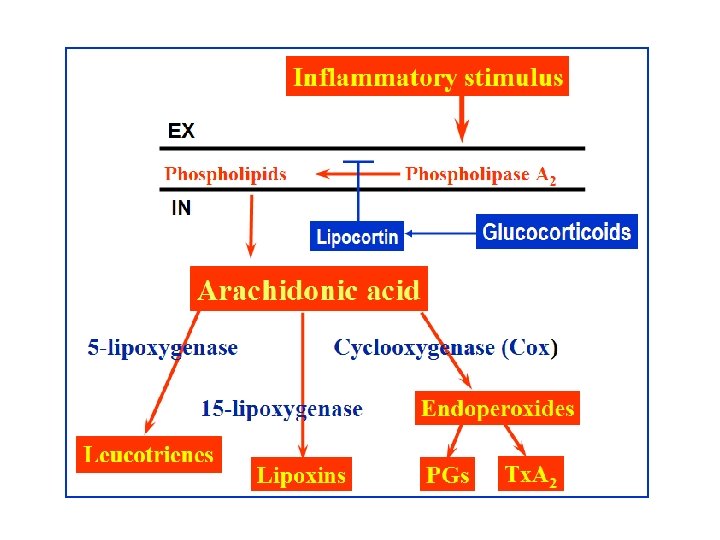
 The anti-inflammatory actions of GCS are mediated by stimulation of synthesis of lipocortin, which inhibits pathways for production of PGs, LTs and PAF. These mediators would normally contribute to increased vascular permeability and subsequent changes including oedema, leucocyte migration, fibrin deposition.
The anti-inflammatory actions of GCS are mediated by stimulation of synthesis of lipocortin, which inhibits pathways for production of PGs, LTs and PAF. These mediators would normally contribute to increased vascular permeability and subsequent changes including oedema, leucocyte migration, fibrin deposition.
 The most used glucocorticoids Hydrocortisone Prednisolone Nonfluorinated prednisolones Methylprednisolone Fluorinated prednisolones Betamethasone, Dexamethasone Fluticasone, Triamcinolone
The most used glucocorticoids Hydrocortisone Prednisolone Nonfluorinated prednisolones Methylprednisolone Fluorinated prednisolones Betamethasone, Dexamethasone Fluticasone, Triamcinolone
 Adverse effects of GCS Cushing’s syndrome • Cushing’s syndrome • Osteoporosis • Tendency to hyperglycae • Negative nitrogen balanc • Increased appetite • Increased susceptibility to infections • Obesity etc.
Adverse effects of GCS Cushing’s syndrome • Cushing’s syndrome • Osteoporosis • Tendency to hyperglycae • Negative nitrogen balanc • Increased appetite • Increased susceptibility to infections • Obesity etc.
 Leukotriene Modulators Metabolism of arachidonic acid via 5 -lipoxige pathway yields the cysteinyl LTs – C 4, D 4 and which activate cysteinyl leukotriene receptors cause bronchoconstriction, stimulate mucus secretion and increase capillary permeability, to pulmonary oedema. Zileuton (p. o. ) inhibits the 5 -lipoxigenase and synthesis of LTs. Zafirlukast, Montelukast and Pranlukast (new block cysteinyl LT-receptors and used with inhaled GCS in poorly respond asthmatic pati
Leukotriene Modulators Metabolism of arachidonic acid via 5 -lipoxige pathway yields the cysteinyl LTs – C 4, D 4 and which activate cysteinyl leukotriene receptors cause bronchoconstriction, stimulate mucus secretion and increase capillary permeability, to pulmonary oedema. Zileuton (p. o. ) inhibits the 5 -lipoxigenase and synthesis of LTs. Zafirlukast, Montelukast and Pranlukast (new block cysteinyl LT-receptors and used with inhaled GCS in poorly respond asthmatic pati
 LTC 4 - receptor LTD 4 - receptor") Arachidonic acid 5 -Lipoxigenase Leukotrienes (LTs) LTC 4 - receptor LTD 4 - receptor LTE 4 - receptor (– ) Montelukast, Zafirlukast
Arachidonic acid 5 -Lipoxigenase Leukotrienes (LTs) LTC 4 - receptor LTD 4 - receptor LTE 4 - receptor (– ) Montelukast, Zafirlukast
 Mast cell stabilizers prevent transmembra of calcium ions, provoked by antigen-Ig. E antib reaction on the mast cell membrane. They prev degranulation and release of histamine and oth autacoids from mast cells. They also inhibit leu activation and chemotaxis. Indications: prophylactic treatment of as Cromoglycate – per inh. (Cromolyn – USAN) Ketotifen (p. o. ) Nedocromil – per inh.
Mast cell stabilizers prevent transmembra of calcium ions, provoked by antigen-Ig. E antib reaction on the mast cell membrane. They prev degranulation and release of histamine and oth autacoids from mast cells. They also inhibit leu activation and chemotaxis. Indications: prophylactic treatment of as Cromoglycate – per inh. (Cromolyn – USAN) Ketotifen (p. o. ) Nedocromil – per inh.
 It inhibits") Monoclonal Anti-Ig. E Antibody Omalizumab is a recombinant humanized monoc antibody. (1) It inhibits the binding of Ig. E to mast c basophils; (3) it inhibits the activation of Ig. E alread to mast cells and prevents their degranulations; (3 down-regulates Fc epsilon receptor-1, present on cells and basophils. Omalizumab is indicated for asthmatic patients wh not adequately controlled by inhaled GCS and wh demonstrate sensitivity to aero-allergens.
Monoclonal Anti-Ig. E Antibody Omalizumab is a recombinant humanized monoc antibody. (1) It inhibits the binding of Ig. E to mast c basophils; (3) it inhibits the activation of Ig. E alread to mast cells and prevents their degranulations; (3 down-regulates Fc epsilon receptor-1, present on cells and basophils. Omalizumab is indicated for asthmatic patients wh not adequately controlled by inhaled GCS and wh demonstrate sensitivity to aero-allergens.
 Treatment of Status Asthmaticus It is a potentially life-threatening acute attack of s asthma needing immediate treatment. Most often hospitalization is necessary. (1) A high concentration (40– 60%) of O 2 is admin (2) High doses of inhaled short acting beta-2 -ago (3) High doses of systemic GCS (p. o. /i. v. ) (4) Ipratropium through inhalation.
Treatment of Status Asthmaticus It is a potentially life-threatening acute attack of s asthma needing immediate treatment. Most often hospitalization is necessary. (1) A high concentration (40– 60%) of O 2 is admin (2) High doses of inhaled short acting beta-2 -ago (3) High doses of systemic GCS (p. o. /i. v. ) (4) Ipratropium through inhalation.
 II. Drug Therapy of Cough The cough is a physiological useful protective refle clears the respiratory pathway of the accumulated and foreign substances. Many times it occurs as a symptom of an underlying disorder and needs trea The cough may be non-productive (dry) and pro The productive cough is characterized by the pres excessive sputum and may be associated with chr bronchitis and bronchiectasis.
II. Drug Therapy of Cough The cough is a physiological useful protective refle clears the respiratory pathway of the accumulated and foreign substances. Many times it occurs as a symptom of an underlying disorder and needs trea The cough may be non-productive (dry) and pro The productive cough is characterized by the pres excessive sputum and may be associated with chr bronchitis and bronchiectasis.
 1. Antitussive Agents are used for the tr t of non-productive cough which increases discom the patients. Centrally Acting Antitussives (supress the cough center that mediates the coug • Codeine (methylmorphine) Poppy • Dihydrocodeine • Dextrometorphan • Glaucin (Glauvent®) Perpheral Acting Antitussives • Prenoxidiazine (Libexin® – tabl. 100 mg)
1. Antitussive Agents are used for the tr t of non-productive cough which increases discom the patients. Centrally Acting Antitussives (supress the cough center that mediates the coug • Codeine (methylmorphine) Poppy • Dihydrocodeine • Dextrometorphan • Glaucin (Glauvent®) Perpheral Acting Antitussives • Prenoxidiazine (Libexin® – tabl. 100 mg)
 2. Expectorants These drugs increase the volume or/and decrease viscosity of the respiratory secretions and facilitate removal by ciliary action and coughing. Mucokinetic Expectorants stimulate the flow of respiratory tract secretions by stimulating the bronc secretory cells (to increase the volume) and the ciliary movement (to facilitate their removal). • Essential oils (oil anise, oil eucalyptus) • Syrup of Ipecacauanha (in sub-emetic doses) • Infusum of Radix Primulae • Ammonium chloride, Sodium citrate • Guaiacol and Guaifenasin (obtained from creosote
2. Expectorants These drugs increase the volume or/and decrease viscosity of the respiratory secretions and facilitate removal by ciliary action and coughing. Mucokinetic Expectorants stimulate the flow of respiratory tract secretions by stimulating the bronc secretory cells (to increase the volume) and the ciliary movement (to facilitate their removal). • Essential oils (oil anise, oil eucalyptus) • Syrup of Ipecacauanha (in sub-emetic doses) • Infusum of Radix Primulae • Ammonium chloride, Sodium citrate • Guaiacol and Guaifenasin (obtained from creosote
 bonds of mucopr") Mucolytic Expectorants decrease the viscosity o by splitting the disulfide (–S–S–) bonds of mucopr This action is further facilitated by alkaline p. H (7– 9 • Ambroxol • Acetylcystene (used also for the treatment of paracetamol intoxication) • Bromhexine • Dornase-alfa • Mesna (used also for protection of cancerogenic of cyclophosphamide and ifosphamide too)
Mucolytic Expectorants decrease the viscosity o by splitting the disulfide (–S–S–) bonds of mucopr This action is further facilitated by alkaline p. H (7– 9 • Ambroxol • Acetylcystene (used also for the treatment of paracetamol intoxication) • Bromhexine • Dornase-alfa • Mesna (used also for protection of cancerogenic of cyclophosphamide and ifosphamide too)