

introduction to crown and bridge work.pptx
- Количество слайдов: 56
 Dr. Asma Manasrah
Dr. Asma Manasrah
 Current concepts of health include positive aspects of quality of life; self esteem and the ability to undertake daily activities, such as eating, speaking and socializing, comfortably and without embarrassment.
Current concepts of health include positive aspects of quality of life; self esteem and the ability to undertake daily activities, such as eating, speaking and socializing, comfortably and without embarrassment.
 As we progress in the new millennium, a rich blend of improving technology, better oral health, a strengthening scientific base and the timeless ability to employ fine manual skills and artistry are making it increasingly possible.
As we progress in the new millennium, a rich blend of improving technology, better oral health, a strengthening scientific base and the timeless ability to employ fine manual skills and artistry are making it increasingly possible.
 CASE SELECTION Can I meet the expectations of the patient? Will the patient be able to tolerate the treatment and then maintain the restorations? Can I justify the damage I am going to do to the patient’s teeth? Can I, and the patient, control the environment to minimize the risk of disease or damage in the long term?
CASE SELECTION Can I meet the expectations of the patient? Will the patient be able to tolerate the treatment and then maintain the restorations? Can I justify the damage I am going to do to the patient’s teeth? Can I, and the patient, control the environment to minimize the risk of disease or damage in the long term?


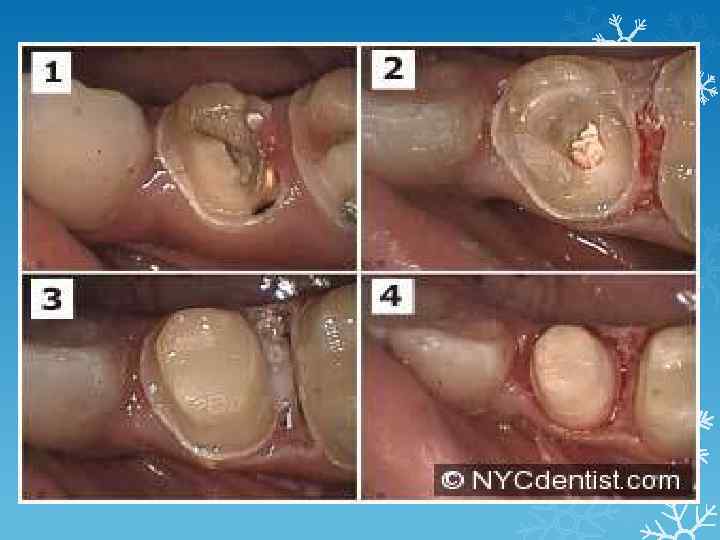
 Are the foundations biologically and biomechanically sound? All crown margins should, ideally, be placed supra gingivally to avoid problems related to gingival inflammation.
Are the foundations biologically and biomechanically sound? All crown margins should, ideally, be placed supra gingivally to avoid problems related to gingival inflammation.
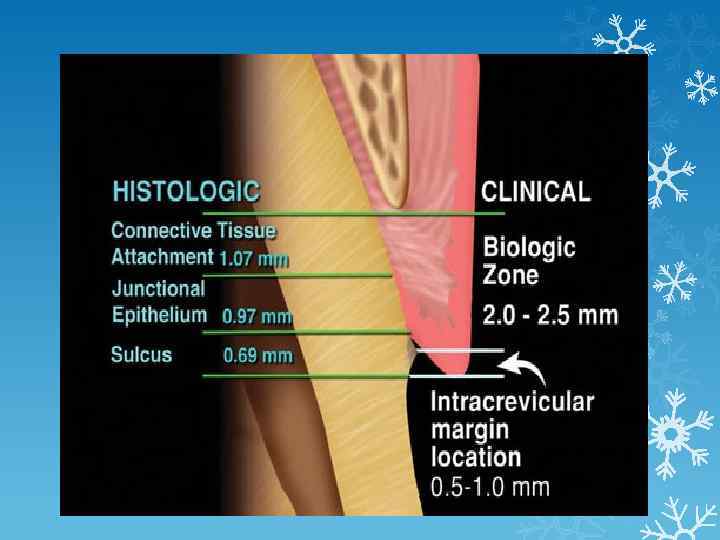
 Where a sub gingival margin is indicated, it is essential that the margin be placed within the limits of the sulcus and that the biologic width is not encroached upon
Where a sub gingival margin is indicated, it is essential that the margin be placed within the limits of the sulcus and that the biologic width is not encroached upon
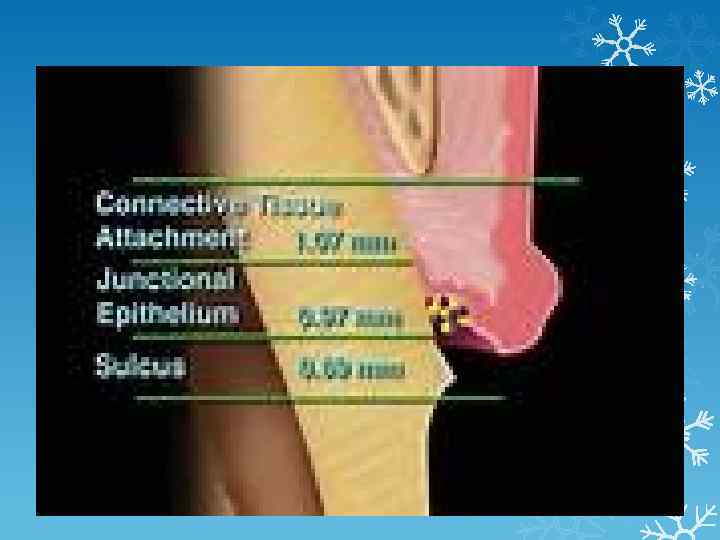
 The biologic width is a band of approximately 2 mm of supra Cristal connective tissue attachment and junctional epithelium around every tooth. If a restoration encroaches upon or eliminates this 2 mm band of attachment, an inflammatory response occurs and attachment loss, apical migration and pocket formation may result.
The biologic width is a band of approximately 2 mm of supra Cristal connective tissue attachment and junctional epithelium around every tooth. If a restoration encroaches upon or eliminates this 2 mm band of attachment, an inflammatory response occurs and attachment loss, apical migration and pocket formation may result.
 Is the endodontic state stable enough to allow a crown to be planned? Is the tooth itself strong enough to receive and retain a crown? Will the preparation be retentive enough? Is there enough space for my restoration?
Is the endodontic state stable enough to allow a crown to be planned? Is the tooth itself strong enough to receive and retain a crown? Will the preparation be retentive enough? Is there enough space for my restoration?

 INDICATIONS FOR CROWN PREPARATION
INDICATIONS FOR CROWN PREPARATION
 STAINED TEETH
STAINED TEETH
 Diastema closure
Diastema closure
 pig-shaped lateral
pig-shaped lateral
 Rotated teeth
Rotated teeth
 TRAUMA
TRAUMA
 Discolored or damaged teeth
Discolored or damaged teeth

 SEVERE TOOTH WEAR
SEVERE TOOTH WEAR
 PART OF ANOTHER RESTORATION TO ALTER THE OCCLUSION
PART OF ANOTHER RESTORATION TO ALTER THE OCCLUSION
 CORE MATERIALS Amalgam Advantages • Not especially technique sensitive • Strong in bulk section • Sealed by corrosion products • Can be ‘glued’ into place with cements and resins
CORE MATERIALS Amalgam Advantages • Not especially technique sensitive • Strong in bulk section • Sealed by corrosion products • Can be ‘glued’ into place with cements and resins

 Disadvantages • Best left to set for 24 hours before tooth preparation • Weak in thin section • Mercury content may be of concern to some patients and dentists • Potential electrolytic action between core and metal crown • Not intrinsically adhesive
Disadvantages • Best left to set for 24 hours before tooth preparation • Weak in thin section • Mercury content may be of concern to some patients and dentists • Potential electrolytic action between core and metal crown • Not intrinsically adhesive

 Composite Advantages • Strong • Can be used in a thinner section than amalgam • Fast setting (either light or chemically cured) • Does not always need a matrix during placement • Avoids mercury controversy
Composite Advantages • Strong • Can be used in a thinner section than amalgam • Fast setting (either light or chemically cured) • Does not always need a matrix during placement • Avoids mercury controversy

 Disadvantages • Highly technique sensitive • Relies on multi-stage dentine bonding requiring effective isolation • Dentine bond can be ruptured by polymerization contraction
Disadvantages • Highly technique sensitive • Relies on multi-stage dentine bonding requiring effective isolation • Dentine bond can be ruptured by polymerization contraction
 • Minor dimensional changes caused by the coefficient of thermal expansion (three times higher than the tooth) and water absorption — not usually clinically significant • Can be difficult to distinguish between tooth and core during preparation
• Minor dimensional changes caused by the coefficient of thermal expansion (three times higher than the tooth) and water absorption — not usually clinically significant • Can be difficult to distinguish between tooth and core during preparation
 Glass ionomer Advantages • Intrinsically adhesive • Fluoride release — but this does not guarantee freedom from 2 o decay • Similar coefficient of thermal expansion to tooth
Glass ionomer Advantages • Intrinsically adhesive • Fluoride release — but this does not guarantee freedom from 2 o decay • Similar coefficient of thermal expansion to tooth
 Disadvantages • Considerably weaker than amalgam and composite • Tendency to crack worsened by early instrumentation • Silver containing materials offer little improvement in physical properties • Some materials radiolucent
Disadvantages • Considerably weaker than amalgam and composite • Tendency to crack worsened by early instrumentation • Silver containing materials offer little improvement in physical properties • Some materials radiolucent
 Resin modified glass ionomers Advantages • Command set • Stronger than regular GICs • Either intrinsically adhesive or with simplified bonding system • Fluoride release Disadvantages • Most are weaker than amalgam and composite • Hydrophilic resins cause swelling and can crack overlying • Some materials can inhibit surface setting of addition impressions porcelain silicone • Not reliable like amalgam and composite as an interim restoration
Resin modified glass ionomers Advantages • Command set • Stronger than regular GICs • Either intrinsically adhesive or with simplified bonding system • Fluoride release Disadvantages • Most are weaker than amalgam and composite • Hydrophilic resins cause swelling and can crack overlying • Some materials can inhibit surface setting of addition impressions porcelain silicone • Not reliable like amalgam and composite as an interim restoration
 Principles of tooth preparation 1. preservation of tooth structure. 2. retention and resistance. 3. structural durability. 4. marginal integrity. 5. preservation of periodontium.
Principles of tooth preparation 1. preservation of tooth structure. 2. retention and resistance. 3. structural durability. 4. marginal integrity. 5. preservation of periodontium.
 BIOMECHANICAL CONSIDERATIONS Periodontal ligament area ANTES LAW “the root surface area of the abutment teeth had to equal or surpass that of the teeth being replaced by pontics” Any FPD replacing more than two teeth should be considered a high risk
BIOMECHANICAL CONSIDERATIONS Periodontal ligament area ANTES LAW “the root surface area of the abutment teeth had to equal or surpass that of the teeth being replaced by pontics” Any FPD replacing more than two teeth should be considered a high risk
 Bending or deflection varies directly with the cube of the length and inversely with the cube of the occlusogingival thickness of the pontic. The dislodging forces on FPD retainer tend to act in mesiodistal direction as opposed to the more common buccolingual direction of forces on a single restoration
Bending or deflection varies directly with the cube of the length and inversely with the cube of the occlusogingival thickness of the pontic. The dislodging forces on FPD retainer tend to act in mesiodistal direction as opposed to the more common buccolingual direction of forces on a single restoration
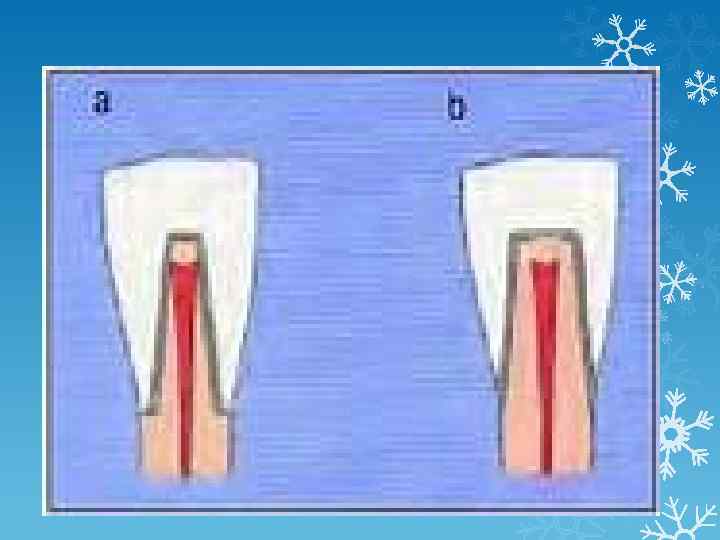
 CROWN ROOT RATIO It is a measure of the length of tooth occlusal to the alveolar crest bone compared with the length of root embedded in the bone Ideal crown root ratio is 1: 2 The optimum crown root ratio for a tooth to be utilized as a FPD abutment is 2: 3 Minimum crown root ratio is 1; 1 Double abutments are used to overcome unfavorable crown root ratio and long spans
CROWN ROOT RATIO It is a measure of the length of tooth occlusal to the alveolar crest bone compared with the length of root embedded in the bone Ideal crown root ratio is 1: 2 The optimum crown root ratio for a tooth to be utilized as a FPD abutment is 2: 3 Minimum crown root ratio is 1; 1 Double abutments are used to overcome unfavorable crown root ratio and long spans
 A secondary abutment must have at least as much root surface area and a favorable crown root ratio as the primary abutment The retainers on secondary abutment must be at least as retentive as the retainers on the primary abutments When the pontic flexes tensile forces will be applied to the retainers on secondary abutments
A secondary abutment must have at least as much root surface area and a favorable crown root ratio as the primary abutment The retainers on secondary abutment must be at least as retentive as the retainers on the primary abutments When the pontic flexes tensile forces will be applied to the retainers on secondary abutments
 Arch curvature has its effect on the stresses occurring in FPD When pontic lie outside the inter abutment axis line, the pontic act as lever arm which can produce a torquing movement Common in replacing upper incisor Best accomplished by gaining additional retention in opposite direction from lever arm
Arch curvature has its effect on the stresses occurring in FPD When pontic lie outside the inter abutment axis line, the pontic act as lever arm which can produce a torquing movement Common in replacing upper incisor Best accomplished by gaining additional retention in opposite direction from lever arm
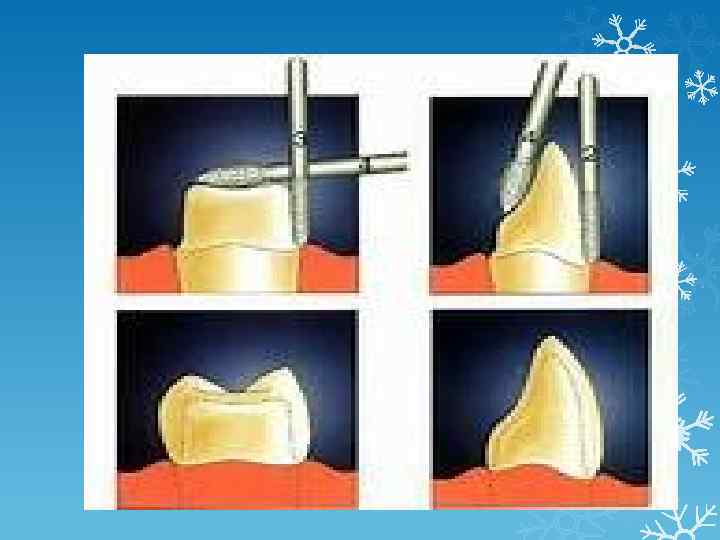
 TOOTH PREPARATION GUIDLINES 1. Total occlusal converence; the angle between 2 opposing prepared axial surfaces Shilling burg et al, suggested that TOC should be between 10 -20 degrees: A. are achievable B. provide adequate resistance to dislodgement
TOOTH PREPARATION GUIDLINES 1. Total occlusal converence; the angle between 2 opposing prepared axial surfaces Shilling burg et al, suggested that TOC should be between 10 -20 degrees: A. are achievable B. provide adequate resistance to dislodgement
 2. Occlusogingival –incisocervical dimension A. 3 mm is the minimal oc dimension for premolars and anterior teeth B. 4 mm is proposed as the minimal oc dimension for prepared molars Teeth that do not possess these minimal dimensions should be modified with auxiliary grooves or boxes
2. Occlusogingival –incisocervical dimension A. 3 mm is the minimal oc dimension for premolars and anterior teeth B. 4 mm is proposed as the minimal oc dimension for prepared molars Teeth that do not possess these minimal dimensions should be modified with auxiliary grooves or boxes


 CIRCUMFERENTIAL MORPHOLOGY The pyramidal tooth preparations provided increased resistance because they possessed corners when compared with conical preparations. It is important to preserve the facio proximal and linguproximal corners of tooth prep. Round teeth should be modified with the creation of grooves or boxes in axial direction.
CIRCUMFERENTIAL MORPHOLOGY The pyramidal tooth preparations provided increased resistance because they possessed corners when compared with conical preparations. It is important to preserve the facio proximal and linguproximal corners of tooth prep. Round teeth should be modified with the creation of grooves or boxes in axial direction.

 FINISH LINE LOCATION SUPRAGINGIVAL FINISH LINES WHEN EVER POSSIBLE Subgingival finish lines required ; 1. To achieve adequate OC dimension for retention and resistance 2. To extend beyond caries 3, To produce acervical crown ferrule 4. to improve esthetics
FINISH LINE LOCATION SUPRAGINGIVAL FINISH LINES WHEN EVER POSSIBLE Subgingival finish lines required ; 1. To achieve adequate OC dimension for retention and resistance 2. To extend beyond caries 3, To produce acervical crown ferrule 4. to improve esthetics
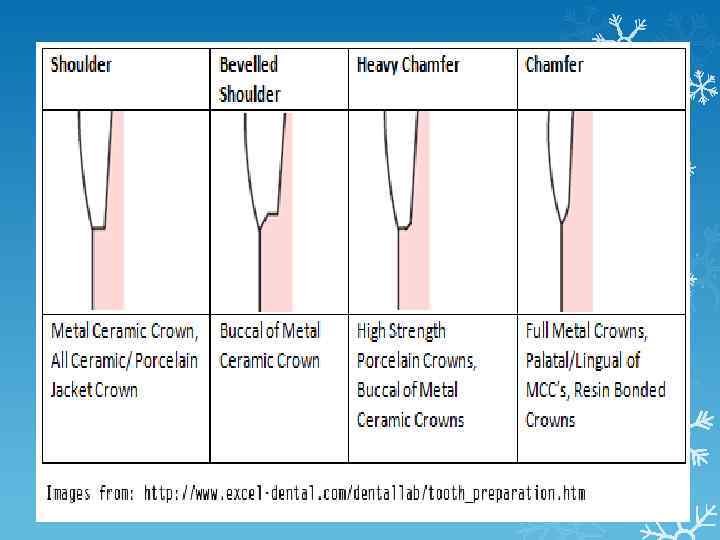
 FINISH LINE FORM AND DEPTH The type of finish line for use with metalceramic crowns should not be based on marginal fit but on personal preference, esthetics. Both shoulder and chamfer finish lines can be used with all ceramic crowns if the crowns are bonded to the prepared tooth. Chamfer finish lines approximately 0. 3 mm deep are well suited for all-metal crowns
FINISH LINE FORM AND DEPTH The type of finish line for use with metalceramic crowns should not be based on marginal fit but on personal preference, esthetics. Both shoulder and chamfer finish lines can be used with all ceramic crowns if the crowns are bonded to the prepared tooth. Chamfer finish lines approximately 0. 3 mm deep are well suited for all-metal crowns
 LINE ANGLE FORM Line angles should be rounded on all ceramic tooth preparations to reduce stress in defensive restoration
LINE ANGLE FORM Line angles should be rounded on all ceramic tooth preparations to reduce stress in defensive restoration
 SURFACE TEXTURE Smooth tooth preparation appears to enhance the fit of restoration Surface roughness increase retention with zinc phosphate cement but it seffect with adhesive cements has not been determined definitely A reasonably smooth tooth preparation is therefore recommended
SURFACE TEXTURE Smooth tooth preparation appears to enhance the fit of restoration Surface roughness increase retention with zinc phosphate cement but it seffect with adhesive cements has not been determined definitely A reasonably smooth tooth preparation is therefore recommended
 REFERENCES 1. Shillingburg H, Fundamentals of fixed prosthdontics, third edetion , 1997. 2. Smith B , Howe L, Planning and making crowns and bridges, 4 th edition, 2007. 3. Goodacre CJ, Campagni WV, Aquilino SA. Tooth preparations for complete crowns : an art form based on scientific principles. J Prosthet Dent 2001. 4. Crowns and other extra-coronal restorations: Introduction R. W. Wassell J. G. Steele and A. W. G. Walls. BRITISH DENTAL JOURNAL VOLUME 192 NO. 3 FEBRUARY 9 2002
REFERENCES 1. Shillingburg H, Fundamentals of fixed prosthdontics, third edetion , 1997. 2. Smith B , Howe L, Planning and making crowns and bridges, 4 th edition, 2007. 3. Goodacre CJ, Campagni WV, Aquilino SA. Tooth preparations for complete crowns : an art form based on scientific principles. J Prosthet Dent 2001. 4. Crowns and other extra-coronal restorations: Introduction R. W. Wassell J. G. Steele and A. W. G. Walls. BRITISH DENTAL JOURNAL VOLUME 192 NO. 3 FEBRUARY 9 2002
