

 Disorders of sex and gender
Disorders of sex and gender
 Sexual Dysfunctions Sexual dysfunctions are disorders in which people cannot respond normally in key areas of sexual functioning As many as 31% of men and 43% of women suffer from such a dysfunction during their lives
Sexual Dysfunctions Sexual dysfunctions are disorders in which people cannot respond normally in key areas of sexual functioning As many as 31% of men and 43% of women suffer from such a dysfunction during their lives
 Sexual Dysfunctions The human sexual response can be described as a cycle with four phases: Desire Excitement Orgasm Resolution Disorder of sexual function affect one or more of the first three phases
Sexual Dysfunctions The human sexual response can be described as a cycle with four phases: Desire Excitement Orgasm Resolution Disorder of sexual function affect one or more of the first three phases

 Figure 10. x 2 Exploring") Summary of Sexual and Gender Identity Disorders (cont. ) Figure 10. x 2 Exploring sexual dysfunctions
Summary of Sexual and Gender Identity Disorders (cont. ) Figure 10. x 2 Exploring sexual dysfunctions
 Etiology of Sexual Dysfunction: Biological factors Diseases of vascular system Diseases of the nervous system Low levels of testosterone or estrogen Heavy alcohol or drug consumption before sex History of chronic alcoholism Heavy cigarette smoking Medications Antihypertensives SSRIs
Etiology of Sexual Dysfunction: Biological factors Diseases of vascular system Diseases of the nervous system Low levels of testosterone or estrogen Heavy alcohol or drug consumption before sex History of chronic alcoholism Heavy cigarette smoking Medications Antihypertensives SSRIs
 Etiology of Sexual Dysfunction: Psychosocial Factors Rape Early childhood sexual abuse Relationship problems Anger, hostility, poor communication Underlying anxiety about relationship security Psychological disorders Major depression, anxiety, or panic disorder Low physiological arousal Stress and exhaustion Negative cognitions
Etiology of Sexual Dysfunction: Psychosocial Factors Rape Early childhood sexual abuse Relationship problems Anger, hostility, poor communication Underlying anxiety about relationship security Psychological disorders Major depression, anxiety, or panic disorder Low physiological arousal Stress and exhaustion Negative cognitions
 Specific Etiologies Common factors of low sexual desire in men & women: Boredom Lack of physical attraction to partner Negative or faulty attitudes Dissatisfaction with partner’s sexual activity History of sexual abuse Common factors of arousal disorders in men & women: Health status Performance anxiety Negative affect: Suppression and expression of anger correlated with higher rates of ED Organic theories of PE Penile hypersensitivity - lower ejaculatory threshold, reached more rapidly Hyperexcitability ejaculatory reflex – faster emission phase Genetic predisposition Central 5 -HT receptor sensitivity – lower 5 -HT transmission, receptor hyposensitivity Religion & culture may influence sexual functioning, all three stages
Specific Etiologies Common factors of low sexual desire in men & women: Boredom Lack of physical attraction to partner Negative or faulty attitudes Dissatisfaction with partner’s sexual activity History of sexual abuse Common factors of arousal disorders in men & women: Health status Performance anxiety Negative affect: Suppression and expression of anger correlated with higher rates of ED Organic theories of PE Penile hypersensitivity - lower ejaculatory threshold, reached more rapidly Hyperexcitability ejaculatory reflex – faster emission phase Genetic predisposition Central 5 -HT receptor sensitivity – lower 5 -HT transmission, receptor hyposensitivity Religion & culture may influence sexual functioning, all three stages
 Prevalence & Comorbidity High rates of comorbidity with anxiety & depression Loss of libido or decreased sexual desire in up to 72% of patients with unipolar depression; 77% with bipolar General medical conditions associated with SD Men: diabetes, cardiovascular disorder, hypertension, dyslipidemia, obesity, smoking, prostate disorders Women: chronic illness, poor general health status, such as diabetes, breast cancer, lower urinary tract infection, surgical removal of ovaries, multiple sclerosis Risk of SD is increased by smoking and excessive alcohol use SD consistently reported in patients taking SSRIs Estimates range from 10%-65%
Prevalence & Comorbidity High rates of comorbidity with anxiety & depression Loss of libido or decreased sexual desire in up to 72% of patients with unipolar depression; 77% with bipolar General medical conditions associated with SD Men: diabetes, cardiovascular disorder, hypertension, dyslipidemia, obesity, smoking, prostate disorders Women: chronic illness, poor general health status, such as diabetes, breast cancer, lower urinary tract infection, surgical removal of ovaries, multiple sclerosis Risk of SD is increased by smoking and excessive alcohol use SD consistently reported in patients taking SSRIs Estimates range from 10%-65%
 Disorders of Desire phase of the sexual response cycle Consists of an urge to have sex, sexual fantasies, and sexual attraction to others A person's sex drive is determined by a combination of biological, psychological, and sociocultural factors, and any of these may reduce sexual desire Most cases of low sexual desire or sexual aversion are caused primarily by sociocultural and psychological factors, but biological conditions can also lower sex drive significantly Two dysfunctions affect this phase: • Male/ female hypoactive sexual desire disorder • Male/ female sexual aversion disorder
Disorders of Desire phase of the sexual response cycle Consists of an urge to have sex, sexual fantasies, and sexual attraction to others A person's sex drive is determined by a combination of biological, psychological, and sociocultural factors, and any of these may reduce sexual desire Most cases of low sexual desire or sexual aversion are caused primarily by sociocultural and psychological factors, but biological conditions can also lower sex drive significantly Two dysfunctions affect this phase: • Male/ female hypoactive sexual desire disorder • Male/ female sexual aversion disorder
 Disorders of Desire Hypoactive sexual desire disorder • Characterized by a lack of interest in sex and little sexual activity • Physical responses may be normal • Accounts for half of all complaints at sexuality clinics • Many experience little excitement during sexual activity, are unaroused by erotic cues, and experience few genital or nongenital sensations during sexual activity 22% of women and 5% of men suffer from this disorder • Sexual Aversion Disorder Little interest in sex Extreme fear, panic, or disgust related to physical or sexual contact 10% of males report panic attacks during attempted sexual activity
Disorders of Desire Hypoactive sexual desire disorder • Characterized by a lack of interest in sex and little sexual activity • Physical responses may be normal • Accounts for half of all complaints at sexuality clinics • Many experience little excitement during sexual activity, are unaroused by erotic cues, and experience few genital or nongenital sensations during sexual activity 22% of women and 5% of men suffer from this disorder • Sexual Aversion Disorder Little interest in sex Extreme fear, panic, or disgust related to physical or sexual contact 10% of males report panic attacks during attempted sexual activity

 Disorders of Desire Biological causes • A number of hormones interact to produce sexual desire and behavior- prolactin, testosterone, and estrogen for both men and women • Abnormalities in their activity can lower sex drive • Recent investigation has also linked sexual desire disorders to excessive activity of the NTs serotonin and dopamine • Sex drive can also be lowered by some medications (including birth control pills and pain medications), some psychotropic drugs, a number of illegal drugs, and chronic illness
Disorders of Desire Biological causes • A number of hormones interact to produce sexual desire and behavior- prolactin, testosterone, and estrogen for both men and women • Abnormalities in their activity can lower sex drive • Recent investigation has also linked sexual desire disorders to excessive activity of the NTs serotonin and dopamine • Sex drive can also be lowered by some medications (including birth control pills and pain medications), some psychotropic drugs, a number of illegal drugs, and chronic illness
 Disorders of Desire Psychological causes • A general increase in anxiety, depression, or anger may reduce sexual desire in both men and women • Fears, attitudes, and memories may contribute to disorder of sexual desire • Certain disorders, including depression and obsessive-compulsive disorder, may lead to sexual desire disorders
Disorders of Desire Psychological causes • A general increase in anxiety, depression, or anger may reduce sexual desire in both men and women • Fears, attitudes, and memories may contribute to disorder of sexual desire • Certain disorders, including depression and obsessive-compulsive disorder, may lead to sexual desire disorders
 Disorders of Desire Sociocultural causes • Attitudes, fears, and psychological disorders that contribute to sexual desire disorders occur within a social context • Many sufferers of desire disorders are feeling situational pressures • Examples: divorce, death, job stress, infertility, and/or relationship difficulties • Cultural standards can lead to development of these disorders • The trauma of sexual molestation or assault is especially likely to produce disorder of sexual desire
Disorders of Desire Sociocultural causes • Attitudes, fears, and psychological disorders that contribute to sexual desire disorders occur within a social context • Many sufferers of desire disorders are feeling situational pressures • Examples: divorce, death, job stress, infertility, and/or relationship difficulties • Cultural standards can lead to development of these disorders • The trauma of sexual molestation or assault is especially likely to produce disorder of sexual desire
 Disorders of Excitement phase of the sexual response cycle Marked by changes in the pelvic region, general physical arousal, and increases in heart rate, muscle tension, blood pressure, and rate of breathing In men: erection of the penis In women: swelling of the clitoris and labia and vaginal lubrication Two dysfunctions affect this phase: Female sexual arousal disorder (formerly “frigidity”) Male erectile disorder (formerly “impotence”)
Disorders of Excitement phase of the sexual response cycle Marked by changes in the pelvic region, general physical arousal, and increases in heart rate, muscle tension, blood pressure, and rate of breathing In men: erection of the penis In women: swelling of the clitoris and labia and vaginal lubrication Two dysfunctions affect this phase: Female sexual arousal disorder (formerly “frigidity”) Male erectile disorder (formerly “impotence”)
 Characterized by persistent inability to attain or") Disorders of Excitement Male erectile disorder (ED) Characterized by persistent inability to attain or maintain an adequate erection during sexual activity This problem occurs in as much as 10% of the general male population According to surveys, half of all adult men have erectile difficulty during intercourse at least some of the time
Disorders of Excitement Male erectile disorder (ED) Characterized by persistent inability to attain or maintain an adequate erection during sexual activity This problem occurs in as much as 10% of the general male population According to surveys, half of all adult men have erectile difficulty during intercourse at least some of the time
 Disorders of Excitement Biological causes • The same hormonal imbalances that can cause hypoactive sexual desire can also produce ED • Most commonly, vascular problems are involved • The use of certain medications and substances may interfere with erections • Medical procedures have been developed for diagnosing biological causes of ED • One strategy involves measuring nocturnal penile tumescence (NPT) • Men typically have erections during REM sleep; abnormal or absent nighttime erections usually indicate a physical basis for erectile failure
Disorders of Excitement Biological causes • The same hormonal imbalances that can cause hypoactive sexual desire can also produce ED • Most commonly, vascular problems are involved • The use of certain medications and substances may interfere with erections • Medical procedures have been developed for diagnosing biological causes of ED • One strategy involves measuring nocturnal penile tumescence (NPT) • Men typically have erections during REM sleep; abnormal or absent nighttime erections usually indicate a physical basis for erectile failure
 Rigiscan The Rigi. Scan, an instrument used to measure continuous penile tumescence and rigidity It has two loops, one to be placed around the base of the penis and the other towards the tip, which tighten every fifteen or thirty seconds The recording unit can be strapped around the waist or thigh
Rigiscan The Rigi. Scan, an instrument used to measure continuous penile tumescence and rigidity It has two loops, one to be placed around the base of the penis and the other towards the tip, which tighten every fifteen or thirty seconds The recording unit can be strapped around the waist or thigh
 Disorders of Excitement Psychological causes • Any of the psychological causes of hypoactive sexual desire can also interfere with arousal and lead to erectile dysfunction • For example, as many as 90% of men with severe depression experience some degree of ED • One well-supported cognitive explanation for ED emphasizes performance anxiety and the spectator role • Once a man begins to have erectile difficulties, he becomes fearful and worries during sexual encounters; instead of being a participant, he becomes a spectator and judge • This can create a vicious cycle of disorder of sexual desire where the original cause of the erectile failure becomes less important than the fear of failure
Disorders of Excitement Psychological causes • Any of the psychological causes of hypoactive sexual desire can also interfere with arousal and lead to erectile dysfunction • For example, as many as 90% of men with severe depression experience some degree of ED • One well-supported cognitive explanation for ED emphasizes performance anxiety and the spectator role • Once a man begins to have erectile difficulties, he becomes fearful and worries during sexual encounters; instead of being a participant, he becomes a spectator and judge • This can create a vicious cycle of disorder of sexual desire where the original cause of the erectile failure becomes less important than the fear of failure
 Disorders of Excitement Sociocultural causes • Each of the sociocultural factors tied to hypoactive sexual desire has also been linked to ED • • Job and marital distress are particularly relevant
Disorders of Excitement Sociocultural causes • Each of the sociocultural factors tied to hypoactive sexual desire has also been linked to ED • • Job and marital distress are particularly relevant
 Disorders of Orgasm phase of the sexual response cycle Sexual pleasure peaks and sexual tension is released as the muscles in the pelvic region contract rhythmically For men: semen is ejaculated For women: the outer third of the vaginal walls contract There are three disorders of this phase: Early ejaculation Delayed ejaculation Female orgasmic disorder
Disorders of Orgasm phase of the sexual response cycle Sexual pleasure peaks and sexual tension is released as the muscles in the pelvic region contract rhythmically For men: semen is ejaculated For women: the outer third of the vaginal walls contract There are three disorders of this phase: Early ejaculation Delayed ejaculation Female orgasmic disorder
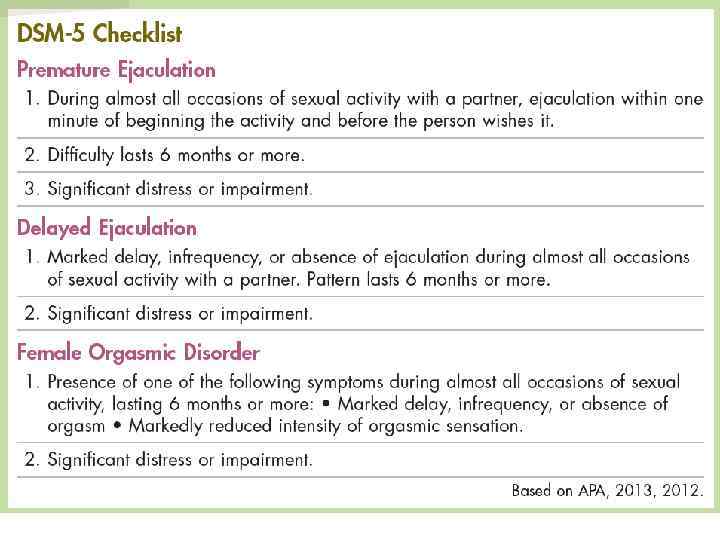
 Disorders of Orgasm – Early Ejaculation Characterized by persistent reaching of orgasm and ejaculation with little sexual stimulation As many as 30% of men experience rapid ejaculation at some time Most prevalent sexual dysfunction in adult males Psychological, particularly behavioral, explanations of this disorder have received more research support than other explanations The dysfunction seems to be typical of young, sexually inexperienced men It may also be related to anxiety, hurried masturbation experiences, or poor recognition of arousal
Disorders of Orgasm – Early Ejaculation Characterized by persistent reaching of orgasm and ejaculation with little sexual stimulation As many as 30% of men experience rapid ejaculation at some time Most prevalent sexual dysfunction in adult males Psychological, particularly behavioral, explanations of this disorder have received more research support than other explanations The dysfunction seems to be typical of young, sexually inexperienced men It may also be related to anxiety, hurried masturbation experiences, or poor recognition of arousal
 Disorders of Orgasm – Delayed Ejaculation Characterized by a repeated inability to reach orgasm or by a very delayed orgasm after normal sexual excitement Occurs in 8% of the male population Rare condition in adult males, but is the most common complaint of adult females 25% of adult females report significant difficulty reaching orgasm 50% of adult females report experiencing regular orgasms during intercourse Biological causes include low testosterone, neurological disease, and head or spinal cord injury A leading psychological cause appears to be performance anxiety and the spectator role, the cognitive factors involved in ED
Disorders of Orgasm – Delayed Ejaculation Characterized by a repeated inability to reach orgasm or by a very delayed orgasm after normal sexual excitement Occurs in 8% of the male population Rare condition in adult males, but is the most common complaint of adult females 25% of adult females report significant difficulty reaching orgasm 50% of adult females report experiencing regular orgasms during intercourse Biological causes include low testosterone, neurological disease, and head or spinal cord injury A leading psychological cause appears to be performance anxiety and the spectator role, the cognitive factors involved in ED
 Disorders of Orgasm- Female Orgasmic Disorder Characterized by persistent delay in or absence of orgasm Most clinicians agree that orgasm during intercourse is not mandatory for normal sexual functioning Typically linked to female sexual arousal disorder
Disorders of Orgasm- Female Orgasmic Disorder Characterized by persistent delay in or absence of orgasm Most clinicians agree that orgasm during intercourse is not mandatory for normal sexual functioning Typically linked to female sexual arousal disorder
 Disorders of Orgasm- Female Orgasmic Disorder Biological causes • A variety of physiological conditions can affect a woman's arousal and orgasm • The same medications and illegal substances that affect erection in men can affect arousal and orgasm in women • Postmenopausal changes may also be responsible Psychological causes • The psychological causes of hypoactive sexual desire and sexual aversion, including depression, may also lead to female arousal and orgasmic disorders • Memories of childhood trauma and relationship distress may also be related
Disorders of Orgasm- Female Orgasmic Disorder Biological causes • A variety of physiological conditions can affect a woman's arousal and orgasm • The same medications and illegal substances that affect erection in men can affect arousal and orgasm in women • Postmenopausal changes may also be responsible Psychological causes • The psychological causes of hypoactive sexual desire and sexual aversion, including depression, may also lead to female arousal and orgasmic disorders • Memories of childhood trauma and relationship distress may also be related
 Disorders of Orgasm- Female Orgasmic Disorder Sociocultural causes • For years, the leading sociocultural theory of female disorder of sexual desire was that it resulted from sexually restrictive cultural messages • This theory has been challenged because: • Sexually restrictive histories are equally common in women with and without disorders • Cultural messages about female sexuality have been changing while the rate of female disorder of sexual desire stays constant • Researchers suggest that unusually stressful events, traumas, or relationships may produce the fears, memories, and attitudes that characterize these dysfunctions • Research has also linked orgasmic behavior to certain qualities in a woman's intimate relationships (such as emotional intimacy)
Disorders of Orgasm- Female Orgasmic Disorder Sociocultural causes • For years, the leading sociocultural theory of female disorder of sexual desire was that it resulted from sexually restrictive cultural messages • This theory has been challenged because: • Sexually restrictive histories are equally common in women with and without disorders • Cultural messages about female sexuality have been changing while the rate of female disorder of sexual desire stays constant • Researchers suggest that unusually stressful events, traumas, or relationships may produce the fears, memories, and attitudes that characterize these dysfunctions • Research has also linked orgasmic behavior to certain qualities in a woman's intimate relationships (such as emotional intimacy)
 Genito-pelvic Pain/sexual pain Disorder Dysfunctions that do not fit neatly into a specific phase of the sexual response cycle and are characterized by enormous physical discomfort during intercourse, and are called genito-pelvic pain/penetration disorders Vaginismus Dyspareunia
Genito-pelvic Pain/sexual pain Disorder Dysfunctions that do not fit neatly into a specific phase of the sexual response cycle and are characterized by enormous physical discomfort during intercourse, and are called genito-pelvic pain/penetration disorders Vaginismus Dyspareunia
 Disorders of Sexual Pain Dyspareunia Characterized by severe pain in the genitals during sexual activity Affects 1% to 5% of men and about 10% to 15% of women Adequate sexual desire, and ability to attain arousal and orgasm Dyspareunia in women usually has a physical cause, most commonly from injury sustained in childbirth Although psychological factors or relationship problems may contribute to dyspareunia, psychosocial factors alone are rarely responsible
Disorders of Sexual Pain Dyspareunia Characterized by severe pain in the genitals during sexual activity Affects 1% to 5% of men and about 10% to 15% of women Adequate sexual desire, and ability to attain arousal and orgasm Dyspareunia in women usually has a physical cause, most commonly from injury sustained in childbirth Although psychological factors or relationship problems may contribute to dyspareunia, psychosocial factors alone are rarely responsible
 Disorders of Sexual Pain Vaginismus Characterized by involuntary contractions of the muscles of the outer third of the vagina fewer than 1% of all women Most clinicians agree with the cognitive-behavioral theory that vaginismus is a learned fear response Some women experience painful intercourse because of infection or disease Many women with vaginismus also have other sexual disorders
Disorders of Sexual Pain Vaginismus Characterized by involuntary contractions of the muscles of the outer third of the vagina fewer than 1% of all women Most clinicians agree with the cognitive-behavioral theory that vaginismus is a learned fear response Some women experience painful intercourse because of infection or disease Many women with vaginismus also have other sexual disorders

 Treatment of sexual disorders Modern sex therapy is short-term and instructive Therapy typically lasts 15 to 20 sessions It is centered on specific sexual problems rather than on broad personality issues Disorders of desire: Affectual awareness, self-instruction training, behavioral techniques, insight-oriented exercises, and biological interventions such as hormone treatments Erectile disorder Treatments for ED focus on reducing a man's performance anxiety and/or increasing his stimulation May include sensate-focus exercises such as the “tease technique” Medications
Treatment of sexual disorders Modern sex therapy is short-term and instructive Therapy typically lasts 15 to 20 sessions It is centered on specific sexual problems rather than on broad personality issues Disorders of desire: Affectual awareness, self-instruction training, behavioral techniques, insight-oriented exercises, and biological interventions such as hormone treatments Erectile disorder Treatments for ED focus on reducing a man's performance anxiety and/or increasing his stimulation May include sensate-focus exercises such as the “tease technique” Medications
 Treatment of sexual disorders Male orgasmic disorder Like treatment for ED, therapies for this disorder include techniques to reduce performance anxiety and increase stimulation When the cause of the disorder is physical, treatment may include a drug to increase arousal of the sympathetic nervous system Early ejaculation Premature ejaculation has been successfully treated for years by behavioral procedures such as the “stop-start” or “pause” , squeeze= Seeman procedure Some clinicians use SSRIs, the serotonin-enhancing antidepressant drugs Because these drugs often reduce sexual arousal or orgasm, they may be helpful in delaying premature ejaculation Many studies have reported positive results with this approach
Treatment of sexual disorders Male orgasmic disorder Like treatment for ED, therapies for this disorder include techniques to reduce performance anxiety and increase stimulation When the cause of the disorder is physical, treatment may include a drug to increase arousal of the sympathetic nervous system Early ejaculation Premature ejaculation has been successfully treated for years by behavioral procedures such as the “stop-start” or “pause” , squeeze= Seeman procedure Some clinicians use SSRIs, the serotonin-enhancing antidepressant drugs Because these drugs often reduce sexual arousal or orgasm, they may be helpful in delaying premature ejaculation Many studies have reported positive results with this approach
 Treatment of sexual disorders Delayed ejaculation Therapies for delayed ejaculation include techniques to reduce performance anxiety and increase stimulation When delayed ejaculation is caused by physical factors such as neurological damage or injury, treatment may include a drug to increase arousal of the sympathetic nervous system
Treatment of sexual disorders Delayed ejaculation Therapies for delayed ejaculation include techniques to reduce performance anxiety and increase stimulation When delayed ejaculation is caused by physical factors such as neurological damage or injury, treatment may include a drug to increase arousal of the sympathetic nervous system
 Treatment of sexual disorders Female orgasmic disorder Specific treatments for these disorders include cognitive-behavioral techniques, self-exploration, enhancement of body awareness, and directed masturbation training Biological treatments, including hormone therapy or the use of sildenafil (Viagra), have also been tried, but research has not found such interventions to be consistently helpful
Treatment of sexual disorders Female orgasmic disorder Specific treatments for these disorders include cognitive-behavioral techniques, self-exploration, enhancement of body awareness, and directed masturbation training Biological treatments, including hormone therapy or the use of sildenafil (Viagra), have also been tried, but research has not found such interventions to be consistently helpful
 Treatment of sexual disorders Vaginismus Specific treatment for vaginismus typically involves two approaches: Practice tightening and releasing the muscles of the vagina to gain more voluntary control Overcome fear of penetration through gradual behavioral exposure treatment- dilators Dyspareunia Determining the specific cause of dyspareunia is the first stage of treatment Given that most cases are caused by physical problems, medical intervention may be necessary
Treatment of sexual disorders Vaginismus Specific treatment for vaginismus typically involves two approaches: Practice tightening and releasing the muscles of the vagina to gain more voluntary control Overcome fear of penetration through gradual behavioral exposure treatment- dilators Dyspareunia Determining the specific cause of dyspareunia is the first stage of treatment Given that most cases are caused by physical problems, medical intervention may be necessary
 Tadalafil (Cialis) Viagra is the most popular of the PDE 5 inhibitors") sildenafil (VIAGRA) Tadalafil (Cialis) Viagra is the most popular of the PDE 5 inhibitors administered orally in 10 mg and 20 mg doses Instructed to take Tadalafil two hours before sexual intercourse 25, 50 and 100 mg doses. Its efficacy is maintained for at least 36 hours Taken 1 hour before sexual intercourse The maximum dosing frequency is once every other day Maximum dose is once daily Window of opportunity: 30 minutes to 45 hrs But can be effective for up to 12 hrs side effects, such as: headache, facial flushing, dyspepsia, dizziness, rhinitis and abnormal vision C/I: after AMI Improved erections were reported by 82. 8% of treated men. Thirty six hours after administration of Tadalafil, 59. 2% of intercourse attempts were successful Side effects: headache, flushing, rhinitis and back pain/myalagia Safety concern: it also serves as an inhibitor of PDE 11, an enzyme in the testes, so there is concern on the effect that it has one sperm and spermatogenesis
sildenafil (VIAGRA) Tadalafil (Cialis) Viagra is the most popular of the PDE 5 inhibitors administered orally in 10 mg and 20 mg doses Instructed to take Tadalafil two hours before sexual intercourse 25, 50 and 100 mg doses. Its efficacy is maintained for at least 36 hours Taken 1 hour before sexual intercourse The maximum dosing frequency is once every other day Maximum dose is once daily Window of opportunity: 30 minutes to 45 hrs But can be effective for up to 12 hrs side effects, such as: headache, facial flushing, dyspepsia, dizziness, rhinitis and abnormal vision C/I: after AMI Improved erections were reported by 82. 8% of treated men. Thirty six hours after administration of Tadalafil, 59. 2% of intercourse attempts were successful Side effects: headache, flushing, rhinitis and back pain/myalagia Safety concern: it also serves as an inhibitor of PDE 11, an enzyme in the testes, so there is concern on the effect that it has one sperm and spermatogenesis
 higher in vitro potency, more rapid binding to PDE 5, and slower") vardenafil (Levitra) higher in vitro potency, more rapid binding to PDE 5, and slower dissociation from this enzyme than Sildenafil and Tadalafil Administered orally on demand in 5, 10 and 20 mg doses Maximum dose administration frequency is once daily There is a window of opportunity from 30 minutes to 4 -5 hours after administration. But, the earliest time to onset of action leading to successful intercourse can be just 10 minutes! 75% of intercourse attempts were successful for patients using vardenafil compare with the 40% success in the placebo group Treatment with vardenafil in patients with erectile dysfunction that were previously unresponsive to sildenafil produced significant improvements in erectile function domain score and maintenance of an erection Side effects: headache, flushing and rhinitis
vardenafil (Levitra) higher in vitro potency, more rapid binding to PDE 5, and slower dissociation from this enzyme than Sildenafil and Tadalafil Administered orally on demand in 5, 10 and 20 mg doses Maximum dose administration frequency is once daily There is a window of opportunity from 30 minutes to 4 -5 hours after administration. But, the earliest time to onset of action leading to successful intercourse can be just 10 minutes! 75% of intercourse attempts were successful for patients using vardenafil compare with the 40% success in the placebo group Treatment with vardenafil in patients with erectile dysfunction that were previously unresponsive to sildenafil produced significant improvements in erectile function domain score and maintenance of an erection Side effects: headache, flushing and rhinitis
 Comparison of sildenafil, vardenafil, tadalafil they all are all PDE 5 inhibitors with the same mechanism of action and similar adverse effects They all require sexual stimulation as a prerequisite and are effective regardless of the cause of erectile dysfunction Viagra has been around the longest and thus has the benefit of having long-term safety data. It also has the highest use and lowest discontinuity of the three drugs. However, Viagra is also administered in higher doses than the others Tadalafil has the longest period of onset (2 hours) and lasts up to 36 hours, whereas as sildenafil is effective up to 12 hours and vardenafil is only effective 4 -5 hours after administration Vardenafil, however, is the most potent (lowest maximal concentration) and binds to PDE 5 more rapidly than the others, thus it has a potential time of onset of 10 minutes
Comparison of sildenafil, vardenafil, tadalafil they all are all PDE 5 inhibitors with the same mechanism of action and similar adverse effects They all require sexual stimulation as a prerequisite and are effective regardless of the cause of erectile dysfunction Viagra has been around the longest and thus has the benefit of having long-term safety data. It also has the highest use and lowest discontinuity of the three drugs. However, Viagra is also administered in higher doses than the others Tadalafil has the longest period of onset (2 hours) and lasts up to 36 hours, whereas as sildenafil is effective up to 12 hours and vardenafil is only effective 4 -5 hours after administration Vardenafil, however, is the most potent (lowest maximal concentration) and binds to PDE 5 more rapidly than the others, thus it has a potential time of onset of 10 minutes
 Dopamine acts on the sympathetic nervous system,") Centrally Acting Oral Drugs: Apomorphine HCL (Urima) Dopamine acts on the sympathetic nervous system, producing effects such as increased heart rate and blood pressure. Male orgasm and ejaculation are under the control of the sympathetic nervous system Apomorphine, as a dopamine receptor agonist specifically activates the oxytocinergic neurons in the paraventricular nucleus of the hypothalamus, releasing erectogenic signals and thus facilitating an erection It is a non-selective dopamine receptor agonist and acts mainly on dopamine D 2 -like receptors in the brain Efficacy rates for erections that are hard enough for intercourse, range from 48%-55% for patients receiving apomorphine. It is fast acting and 71% of erections are achieved within 20 minutes of administration Side Effect: nausea 96% of men surveyed preferred sildenafil over apomorphine as a treatment for erectile dysfunction
Centrally Acting Oral Drugs: Apomorphine HCL (Urima) Dopamine acts on the sympathetic nervous system, producing effects such as increased heart rate and blood pressure. Male orgasm and ejaculation are under the control of the sympathetic nervous system Apomorphine, as a dopamine receptor agonist specifically activates the oxytocinergic neurons in the paraventricular nucleus of the hypothalamus, releasing erectogenic signals and thus facilitating an erection It is a non-selective dopamine receptor agonist and acts mainly on dopamine D 2 -like receptors in the brain Efficacy rates for erections that are hard enough for intercourse, range from 48%-55% for patients receiving apomorphine. It is fast acting and 71% of erections are achieved within 20 minutes of administration Side Effect: nausea 96% of men surveyed preferred sildenafil over apomorphine as a treatment for erectile dysfunction
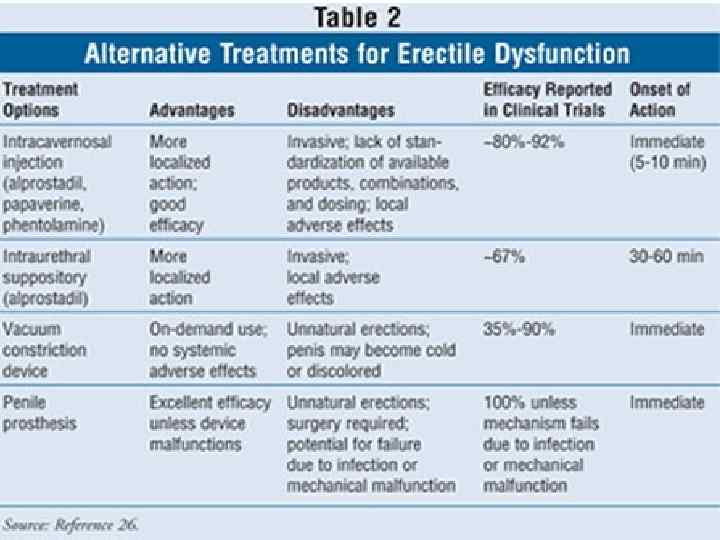
 Intracavernous Pharmacotherapy Patients that are not responding to oral drugs may be offered intracavernous injections Papaverine and alprostadil are the main drugs used for intracavernous treatment
Intracavernous Pharmacotherapy Patients that are not responding to oral drugs may be offered intracavernous injections Papaverine and alprostadil are the main drugs used for intracavernous treatment
 Alprostadil causes blood vessels to expand, increasing blood flow throughout") Alprostadil (MUSE, Caverject, Befar) Alprostadil causes blood vessels to expand, increasing blood flow throughout the body. Thus, by increasing blood flow to the penis, alprostadil helps facilitate an erection Alprostadil is a vasoactive prostaglandin E 1 It is more effective when used in combination with phentolamine and papaverine; this is considered a tri-mix combination therapy. This trimix has an extremely high rate of efficacy at 92% However, alprostadil is normally administered by itself. Sexual activity is reported after 94% of injections, a figure that no other sexual dysfunction treatment option has reached. It also has an almost immediate onset of action Side Effects: penile pain, prolonged erections, priapism, and fibrosis alprostadil is also now available in a cream, under the brand name Befar
Alprostadil (MUSE, Caverject, Befar) Alprostadil causes blood vessels to expand, increasing blood flow throughout the body. Thus, by increasing blood flow to the penis, alprostadil helps facilitate an erection Alprostadil is a vasoactive prostaglandin E 1 It is more effective when used in combination with phentolamine and papaverine; this is considered a tri-mix combination therapy. This trimix has an extremely high rate of efficacy at 92% However, alprostadil is normally administered by itself. Sexual activity is reported after 94% of injections, a figure that no other sexual dysfunction treatment option has reached. It also has an almost immediate onset of action Side Effects: penile pain, prolonged erections, priapism, and fibrosis alprostadil is also now available in a cream, under the brand name Befar
 Testosterone Most commonly used drug for treatment of FSD, especially in post-menopausal women Works to stimulate sexual desire Extremely low doses required- 20 mg administered subcutaneously every three weeks Creams, patches, and combinations with estrogen and progesterone are being developed Side effects: masculinization and could cause liver toxicity in high doses Intrinsa is a Testosterone patch, Testomax is a gel preparation
Testosterone Most commonly used drug for treatment of FSD, especially in post-menopausal women Works to stimulate sexual desire Extremely low doses required- 20 mg administered subcutaneously every three weeks Creams, patches, and combinations with estrogen and progesterone are being developed Side effects: masculinization and could cause liver toxicity in high doses Intrinsa is a Testosterone patch, Testomax is a gel preparation
 Available in pill, cream or injection Used to help relieve menopause symptoms") Estrogen (Premarin) Available in pill, cream or injection Used to help relieve menopause symptoms that occur due to decrease in levels of estrogen such as vaginal dryness, itching and discomfort Side effects of conjugated estrogens include headache, abdominal pain, nervousness, nausea, back pain, joint pain and vaginal bleeding. Patients may also experience vaginal spotting, loss of periods or excessively prolonged periods, breast pain, breast enlargement and an increase or decrease in sexual drive
Estrogen (Premarin) Available in pill, cream or injection Used to help relieve menopause symptoms that occur due to decrease in levels of estrogen such as vaginal dryness, itching and discomfort Side effects of conjugated estrogens include headache, abdominal pain, nervousness, nausea, back pain, joint pain and vaginal bleeding. Patients may also experience vaginal spotting, loss of periods or excessively prolonged periods, breast pain, breast enlargement and an increase or decrease in sexual drive
 Viagra and Befar for women Due to Viagra’s PDE 5 inhibition it may improve vaginal engorgement and lubrication. Viagra for women is called Avlimil and was created in 2003. 84 percent success rate of decreasing symptoms of female sexual dysfunction, but It doesn’t have FDA approval yet Befar, the topical alprostadil cream, may be used to treat Female Sexual Arousal Disorder. It would cause clitoral stimulation by vasodilatation
Viagra and Befar for women Due to Viagra’s PDE 5 inhibition it may improve vaginal engorgement and lubrication. Viagra for women is called Avlimil and was created in 2003. 84 percent success rate of decreasing symptoms of female sexual dysfunction, but It doesn’t have FDA approval yet Befar, the topical alprostadil cream, may be used to treat Female Sexual Arousal Disorder. It would cause clitoral stimulation by vasodilatation
 48
48
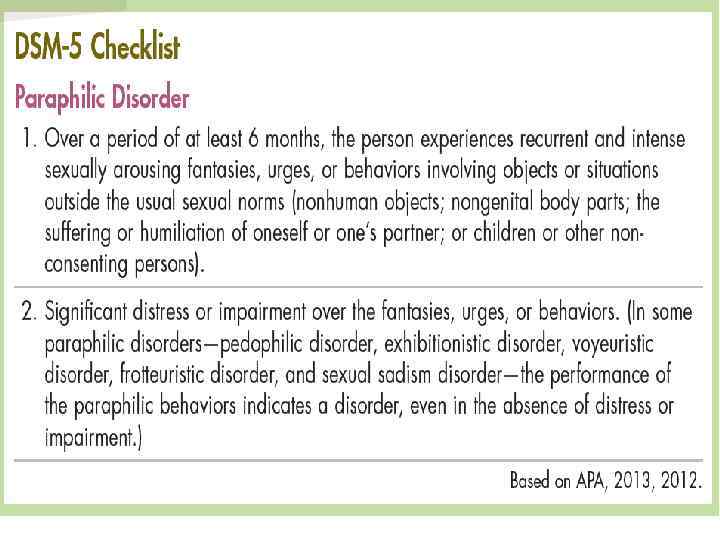
 Paraphilias These disorders are characterized by intense sexual urges, fantasies or behaviors that involve: Nonhumans Children Nonconsenting adults The experience of suffering or humiliation According to the DSM-5, paraphilias should be diagnosed only when the urges, fantasies, or behaviors last at least 6 months For most paraphilias, the urges, fantasies, or behaviors must also cause great distress or interfere with one's functioning Some people with one kind of paraphilia display others as well Relatively few people receive a formal diagnosis, but clinicians suspect that the patterns may be quite common
Paraphilias These disorders are characterized by intense sexual urges, fantasies or behaviors that involve: Nonhumans Children Nonconsenting adults The experience of suffering or humiliation According to the DSM-5, paraphilias should be diagnosed only when the urges, fantasies, or behaviors last at least 6 months For most paraphilias, the urges, fantasies, or behaviors must also cause great distress or interfere with one's functioning Some people with one kind of paraphilia display others as well Relatively few people receive a formal diagnosis, but clinicians suspect that the patterns may be quite common
 A model of the development of paraphilia
A model of the development of paraphilia
 Paraphilias: Clinical Descriptions and Causes Nature of Paraphilias Sexual attraction and arousal to inappropriate people, or objects Often multiple paraphilic patterns of arousal High comorbidity with anxiety, mood, and substance abuse disorders
Paraphilias: Clinical Descriptions and Causes Nature of Paraphilias Sexual attraction and arousal to inappropriate people, or objects Often multiple paraphilic patterns of arousal High comorbidity with anxiety, mood, and substance abuse disorders
 What causes paraphilias? Freudian theorists – arrested psychosexual development early in childhood; defense mechanisms develop to reduce anxiety Learning theorists – classical conditioning (association of an object with sexual arousal) or operant conditioning (early unusual sexual experiences are reinforced by orgasm Paraphilias and obsessive-compulsive disorder have many similarities Psychological factors- Classical conditioning, Operant conditioning Poor social skills or reinforcement of unconventionality History of childhood physical and sexual abuse Alcohol & negative affect are common triggers Cognitive distortions- “Because the child doesn’t run away, she must want me to fondle her” 53
What causes paraphilias? Freudian theorists – arrested psychosexual development early in childhood; defense mechanisms develop to reduce anxiety Learning theorists – classical conditioning (association of an object with sexual arousal) or operant conditioning (early unusual sexual experiences are reinforced by orgasm Paraphilias and obsessive-compulsive disorder have many similarities Psychological factors- Classical conditioning, Operant conditioning Poor social skills or reinforcement of unconventionality History of childhood physical and sexual abuse Alcohol & negative affect are common triggers Cognitive distortions- “Because the child doesn’t run away, she must want me to fondle her” 53
 Why are they so often male? Attitudes about and expectations of men and women are different; consider women “flashing” or cross-dressing Most paraphiliacs are heterosexual, but generally have poor social skills, low self-esteem, history of childhood abuse or neglect (or were raised in families where sex was thought to be evil and normal erotic development was inhibited), and anger at women 54
Why are they so often male? Attitudes about and expectations of men and women are different; consider women “flashing” or cross-dressing Most paraphiliacs are heterosexual, but generally have poor social skills, low self-esteem, history of childhood abuse or neglect (or were raised in families where sex was thought to be evil and normal erotic development was inhibited), and anger at women 54
 Sadism – arousal from infliction of pain on another person Masochism –") Sadomasochism (S&M) Sadism – arousal from infliction of pain on another person Masochism – arousal from experiencing pain In its extreme (paraphilic) form, masochism is more common than sadism, and male sadists far outnumber female sadists Sadists who act out their impulses share many characteristics and behaviors with other sexual aggressors 55
Sadomasochism (S&M) Sadism – arousal from infliction of pain on another person Masochism – arousal from experiencing pain In its extreme (paraphilic) form, masochism is more common than sadism, and male sadists far outnumber female sadists Sadists who act out their impulses share many characteristics and behaviors with other sexual aggressors 55
 In their milder forms S&M are very common as sexual") Dominance and submission (D&S) In their milder forms S&M are very common as sexual variants between consenting partners Rather than extreme pain, the distinctive feature of this roleplaying sex game is domination (or discipline) and submission. Pain is erotically arousing only as part of the agreed-upon ritual or “script” Mutual consent, trust, concern for each other’s safety, sexual and emotional pleasure are characteristics of healthy S&M (D&S) “play” 56
Dominance and submission (D&S) In their milder forms S&M are very common as sexual variants between consenting partners Rather than extreme pain, the distinctive feature of this roleplaying sex game is domination (or discipline) and submission. Pain is erotically arousing only as part of the agreed-upon ritual or “script” Mutual consent, trust, concern for each other’s safety, sexual and emotional pleasure are characteristics of healthy S&M (D&S) “play” 56
 Sexual Masochism Disorder Characterized by fantasies, urges, or behaviors involving the act or the thought of being humiliated, beaten, bound, or otherwise made to suffer Most masochistic fantasies begin in childhood and seem to develop through the behavioral process of classical conditioning
Sexual Masochism Disorder Characterized by fantasies, urges, or behaviors involving the act or the thought of being humiliated, beaten, bound, or otherwise made to suffer Most masochistic fantasies begin in childhood and seem to develop through the behavioral process of classical conditioning
 Sexual Sadism Disorder A person with sexual sadism finds fantasies, urges, or behaviors involving the thought or act of psychological or physical suffering of a victim sexually exciting Named for the infamous Marquis de Sade People with sexual sadism imagine that they have total control over a sexual victim
Sexual Sadism Disorder A person with sexual sadism finds fantasies, urges, or behaviors involving the thought or act of psychological or physical suffering of a victim sexually exciting Named for the infamous Marquis de Sade People with sexual sadism imagine that they have total control over a sexual victim
 Sexual Sadism Sadistic fantasies may first appear in childhood or adolescence Pattern is long-term Appears to be related to classical conditioning and/or modeling Psychodynamic and cognitive theorists view people with sexual sadism as having underlying feelings of sexual inadequacy Biological studies have found signs of possible brain and hormonal abnormalities The primary treatment for this disorder is aversion therapy
Sexual Sadism Sadistic fantasies may first appear in childhood or adolescence Pattern is long-term Appears to be related to classical conditioning and/or modeling Psychodynamic and cognitive theorists view people with sexual sadism as having underlying feelings of sexual inadequacy Biological studies have found signs of possible brain and hormonal abnormalities The primary treatment for this disorder is aversion therapy
 Flagellation Flagellation is the act of beating the human body with special implements such as whips, lashes, rods etc. It can be submitted to willingly, or performed on oneself, in religious or sadomasochistic contexts Flagellation is also used as a sexual practice in the context of BDSM. The intensity of the beating is usually far less than used for punishment 60
Flagellation Flagellation is the act of beating the human body with special implements such as whips, lashes, rods etc. It can be submitted to willingly, or performed on oneself, in religious or sadomasochistic contexts Flagellation is also used as a sexual practice in the context of BDSM. The intensity of the beating is usually far less than used for punishment 60
 Who plays these “games? ” Most are socially well adjusted but close to 1/3 report extreme nervous anxiety Ratio of men to women is 2: 1; heterosexual, well educated (often with prominent careers), and also enjoy “ordinary” sexual activities Dominators – master/mistress, top Submissives – slave, bottom 61
Who plays these “games? ” Most are socially well adjusted but close to 1/3 report extreme nervous anxiety Ratio of men to women is 2: 1; heterosexual, well educated (often with prominent careers), and also enjoy “ordinary” sexual activities Dominators – master/mistress, top Submissives – slave, bottom 61
 Fetishistic Disorder The key features of fetishistic disorder are recurrent intense sexual urges, sexually arousing fantasies, or behaviors that involve the use of a nonliving object, often to the exclusion of all other stimuli The disorder, far more common in men than women, usually begins in adolescence Almost anything can be a fetish Researchers have been unable to pinpoint the causes of fetishistic disorder Psychodynamic theorists view fetishes as defense mechanisms, but therapy using this model has been unsuccessful
Fetishistic Disorder The key features of fetishistic disorder are recurrent intense sexual urges, sexually arousing fantasies, or behaviors that involve the use of a nonliving object, often to the exclusion of all other stimuli The disorder, far more common in men than women, usually begins in adolescence Almost anything can be a fetish Researchers have been unable to pinpoint the causes of fetishistic disorder Psychodynamic theorists view fetishes as defense mechanisms, but therapy using this model has been unsuccessful
 Fetishistic Disorder Behaviorists propose that fetishes are learned through classical conditioning Fetishes are sometimes treated with aversion therapy, or covert sensitization Another behavioral treatment is masturbatory satiation, in which clients masturbate to boredom while imagining the fetish object An additional behavioral treatment is orgasmic reorientation, a process which teaches individuals to respond to more appropriate sources of sexual stimulation
Fetishistic Disorder Behaviorists propose that fetishes are learned through classical conditioning Fetishes are sometimes treated with aversion therapy, or covert sensitization Another behavioral treatment is masturbatory satiation, in which clients masturbate to boredom while imagining the fetish object An additional behavioral treatment is orgasmic reorientation, a process which teaches individuals to respond to more appropriate sources of sexual stimulation
 – arousal by urination Coprophilia – arousal by excrement") Fetish-like paraphilias Urophilia (“golden shower) – arousal by urination Coprophilia – arousal by excrement Mysophilia – arousal by filth (sweaty socks, tampons) Beastiality– arousal through sexual contact with animals; most who have done this have done so only a few times as adolescents Zoophilia – when beastiality is preferred; usually horses or dogs; oralgenital sex is most common, vaginal sex 2 nd, masturbating the animal 3 rd, receiving intercourse from the animal 4 th. 64
Fetish-like paraphilias Urophilia (“golden shower) – arousal by urination Coprophilia – arousal by excrement Mysophilia – arousal by filth (sweaty socks, tampons) Beastiality– arousal through sexual contact with animals; most who have done this have done so only a few times as adolescents Zoophilia – when beastiality is preferred; usually horses or dogs; oralgenital sex is most common, vaginal sex 2 nd, masturbating the animal 3 rd, receiving intercourse from the animal 4 th. 64
 Hypoxyphilia- erotic asphyxiation or breath control play is the intentional restriction of oxygen to the brain for the purposes of sexual arousal. This sexual practice is variously called asphyxiophilia, autoerotic asphyxia, hypoxyphilia. The term autoerotic asphyxiation is used when the act is done by a person to themselves. Various methods are used to achieve the level of oxygen depletion needed, such as a hanging, suffocation with a plastic bag over the head, self-strangulation such as with a ligature, gas or volatile solvents, chest compression, or some combination of these The practice can be dangerous even if performed with care and has resulted in a significant number of accidental deaths Autoerotic asphyxiation may often be mistaken for suicide, which is a major cause of death in teenagers 65
Hypoxyphilia- erotic asphyxiation or breath control play is the intentional restriction of oxygen to the brain for the purposes of sexual arousal. This sexual practice is variously called asphyxiophilia, autoerotic asphyxia, hypoxyphilia. The term autoerotic asphyxiation is used when the act is done by a person to themselves. Various methods are used to achieve the level of oxygen depletion needed, such as a hanging, suffocation with a plastic bag over the head, self-strangulation such as with a ligature, gas or volatile solvents, chest compression, or some combination of these The practice can be dangerous even if performed with care and has resulted in a significant number of accidental deaths Autoerotic asphyxiation may often be mistaken for suicide, which is a major cause of death in teenagers 65
 Transvestic Disorder Also known as transvestism or cross-dressing Characterized by fantasies, urges, or behaviors involving dressing in the clothes of the opposite sex in order to achieve sexual arousal The typical person with transvestism is a heterosexual male who began cross-dressing in childhood or adolescence Transvestism is often confused with gender dysphoria (transsexualism), but the two are separate patterns The development of the disorder seems to follow the behavioral principles of operant conditioning
Transvestic Disorder Also known as transvestism or cross-dressing Characterized by fantasies, urges, or behaviors involving dressing in the clothes of the opposite sex in order to achieve sexual arousal The typical person with transvestism is a heterosexual male who began cross-dressing in childhood or adolescence Transvestism is often confused with gender dysphoria (transsexualism), but the two are separate patterns The development of the disorder seems to follow the behavioral principles of operant conditioning
 Exhibitionistic Disorder Characterized by arousal from the exposure of genitals in a public setting Also known as “flashing” Sexual contact is rarely initiated nor desired Usually begins before age 18 and is most common in males Treatment generally includes aversion therapy and masturbatory satiation May be combined with orgasmic reorientation, social skills training, or cognitive-behavioral therapy
Exhibitionistic Disorder Characterized by arousal from the exposure of genitals in a public setting Also known as “flashing” Sexual contact is rarely initiated nor desired Usually begins before age 18 and is most common in males Treatment generally includes aversion therapy and masturbatory satiation May be combined with orgasmic reorientation, social skills training, or cognitive-behavioral therapy
 Exhibitionists – Who are they? Almost all are men (nobody is scared when a woman shows her genitals) who began exposing themselves in their late teens or early 20 s; half or more have been or are married They are emotionally immature, feel inadequate, fear rejection and have trouble forming intimate relationships Most are have normal or above normal intelligence 68
Exhibitionists – Who are they? Almost all are men (nobody is scared when a woman shows her genitals) who began exposing themselves in their late teens or early 20 s; half or more have been or are married They are emotionally immature, feel inadequate, fear rejection and have trouble forming intimate relationships Most are have normal or above normal intelligence 68
 Are they dangerous? A small number of rapists engaged in exhibitionism when younger, but for the most part, they are a different group of men Because their erotic turn-on is directly related to the victim’s expression of shock, disgust and fear, the best way to avoid reinforcing this behavior is to give no facial or verbal response; just leave quietly and report the incident immediately 69
Are they dangerous? A small number of rapists engaged in exhibitionism when younger, but for the most part, they are a different group of men Because their erotic turn-on is directly related to the victim’s expression of shock, disgust and fear, the best way to avoid reinforcing this behavior is to give no facial or verbal response; just leave quietly and report the incident immediately 69
 Voyeuristic Disorder Characterized by repeated and intense sexual urges to observe people as they undress or to spy on couples having intercourse The person may masturbate during the act of observing or while remembering it later The risk of discovery often adds to the excitement Many psychodynamic theorists propose that voyeurs are seeking power Behaviorists explain voyeurism as a learned behavior that can be traced to a chance and secret observation of a sexually arousing scene
Voyeuristic Disorder Characterized by repeated and intense sexual urges to observe people as they undress or to spy on couples having intercourse The person may masturbate during the act of observing or while remembering it later The risk of discovery often adds to the excitement Many psychodynamic theorists propose that voyeurs are seeking power Behaviorists explain voyeurism as a learned behavior that can be traced to a chance and secret observation of a sexually arousing scene
 Are voyeurs dangerous? Generally not, unless he tries to draw attention to the fact that he is watching you or tries to enter your building. Most prefer to stay hidden Most have a history of great difficulty in heterosexual relationships. They are emotionally immature Scoptophilia differs from voyeurism in that the persons being watched have consented 71
Are voyeurs dangerous? Generally not, unless he tries to draw attention to the fact that he is watching you or tries to enter your building. Most prefer to stay hidden Most have a history of great difficulty in heterosexual relationships. They are emotionally immature Scoptophilia differs from voyeurism in that the persons being watched have consented 71
 Frotteuristic Disorder A person who develops frotteuristic disorder has recurrent and intense fantasies, urges, or behaviors involving touching and rubbing against a nonconsenting person Almost always male, the person fantasizes during the act that he is having a caring relationship with the victim Usually begins in the teen years or earlier Acts generally decrease and disappear after age 25
Frotteuristic Disorder A person who develops frotteuristic disorder has recurrent and intense fantasies, urges, or behaviors involving touching and rubbing against a nonconsenting person Almost always male, the person fantasizes during the act that he is having a caring relationship with the victim Usually begins in the teen years or earlier Acts generally decrease and disappear after age 25
 Pedophilic Disorder Characterized by fantasies, urges, or behaviors involving sexual activity with a prepubescent child, usually 13 years of age or younger Some people are satisfied with child pornography Others are driven to watching, fondling, or engaging in sexual intercourse with children Two-thirds of victims are female
Pedophilic Disorder Characterized by fantasies, urges, or behaviors involving sexual activity with a prepubescent child, usually 13 years of age or younger Some people are satisfied with child pornography Others are driven to watching, fondling, or engaging in sexual intercourse with children Two-thirds of victims are female
 Pedophilic Disorder People with pedophilic disorder develop the disorder in adolescence Some were sexually abused as children Most are immature, display distorted thinking, and have an additional psychological disorder Most people with pedophilic disorder are imprisoned or forced into treatment Treatments include aversion therapy, masturbatory satiation, orgasmic reorientation, and treatment with antiandrogen drugs Cognitive-behavioral treatment involves relapse-prevention training, modeled after programs used for substance dependence
Pedophilic Disorder People with pedophilic disorder develop the disorder in adolescence Some were sexually abused as children Most are immature, display distorted thinking, and have an additional psychological disorder Most people with pedophilic disorder are imprisoned or forced into treatment Treatments include aversion therapy, masturbatory satiation, orgasmic reorientation, and treatment with antiandrogen drugs Cognitive-behavioral treatment involves relapse-prevention training, modeled after programs used for substance dependence
 Pedophilia: Causes and Assessment Causes of Pedophilia Patterns of inappropriate arousal and fantasy may be learned early in life Pedophilia is associated with sexual and social problems and deficits The role of high sex drive, coupled with suppression of urges Psychophysiological Assessment of Pedophilia Assess extent of deviant patterns of sexual arousal Assess extent of desired sexual arousal to adult content Assess social skills and the ability to form relationships
Pedophilia: Causes and Assessment Causes of Pedophilia Patterns of inappropriate arousal and fantasy may be learned early in life Pedophilia is associated with sexual and social problems and deficits The role of high sex drive, coupled with suppression of urges Psychophysiological Assessment of Pedophilia Assess extent of deviant patterns of sexual arousal Assess extent of desired sexual arousal to adult content Assess social skills and the ability to form relationships
 Telephone scatologia Making an obscene phone call is a verbal form of exhibitionism; like exhibitionism, it is a disorder of the affiliative phase of courtship Sexual arousal is proportionate with the victim’s negative reaction. Even slamming down the phone is reinforcing to him Different types: shock caller, ingratiating seducer, and trickster It is rare that they would approach or molest their victims; most prefer total anonymity 76
Telephone scatologia Making an obscene phone call is a verbal form of exhibitionism; like exhibitionism, it is a disorder of the affiliative phase of courtship Sexual arousal is proportionate with the victim’s negative reaction. Even slamming down the phone is reinforcing to him Different types: shock caller, ingratiating seducer, and trickster It is rare that they would approach or molest their victims; most prefer total anonymity 76
 Other paraphilias Internet sex addiction - preferred over sexual relations with a “live” partner Necrophilia – arousal from having sex with dead bodies Most are men; most are believed to be severely emotionally disturbed or psychotic Vampirism – arousal by extraction of blood 77
Other paraphilias Internet sex addiction - preferred over sexual relations with a “live” partner Necrophilia – arousal from having sex with dead bodies Most are men; most are believed to be severely emotionally disturbed or psychotic Vampirism – arousal by extraction of blood 77
 Treatment for Paraphilias Incarceration and court ordered treatment are common Hormonal agents to reduce androgens Depo-Provera SSRIs Denial and minimization of problem often present Lack of motivation for treatment Some blame the victim 78
Treatment for Paraphilias Incarceration and court ordered treatment are common Hormonal agents to reduce androgens Depo-Provera SSRIs Denial and minimization of problem often present Lack of motivation for treatment Some blame the victim 78
 Pedophilia: Psychosocial Treatment Psychosocial Interventions Covert sensitization – Imaginal procedure involving aversive consequences Orgasmic reconditioning – Associate masturbation with appropriate stimuli Family/marital therapy – Address interpersonal problems Most are behavioral and target deviant and inappropriate sexual associations Coping and relapse prevention – Teaches self-control and coping with risk Efficacy of Psychosocial Interventions About 70% to 100% of cases show improvement Poorest outcomes are for rapists and persons with multiple paraphilias
Pedophilia: Psychosocial Treatment Psychosocial Interventions Covert sensitization – Imaginal procedure involving aversive consequences Orgasmic reconditioning – Associate masturbation with appropriate stimuli Family/marital therapy – Address interpersonal problems Most are behavioral and target deviant and inappropriate sexual associations Coping and relapse prevention – Teaches self-control and coping with risk Efficacy of Psychosocial Interventions About 70% to 100% of cases show improvement Poorest outcomes are for rapists and persons with multiple paraphilias
 Pedophilia: Drug Treatments Medications: The Equivalent of Chemical Castration Often used for dangerous sexual offenders Types of Available Medications Medroxyprogesterone acetate – Depo-provera, also reduces testosterone Cyproterone acetate – Anti-androgen, reduces testosterone, sexual urges and fantasy Triptoretin – A newer and more effective drug that inhibits gonadtropin secretion Efficacy of Medication Treatments Drugs work to greatly reduce sexual desire, fantasy, arousal Relapse rates are high with medication discontinuation
Pedophilia: Drug Treatments Medications: The Equivalent of Chemical Castration Often used for dangerous sexual offenders Types of Available Medications Medroxyprogesterone acetate – Depo-provera, also reduces testosterone Cyproterone acetate – Anti-androgen, reduces testosterone, sexual urges and fantasy Triptoretin – A newer and more effective drug that inhibits gonadtropin secretion Efficacy of Medication Treatments Drugs work to greatly reduce sexual desire, fantasy, arousal Relapse rates are high with medication discontinuation
 Gender disorders
Gender disorders
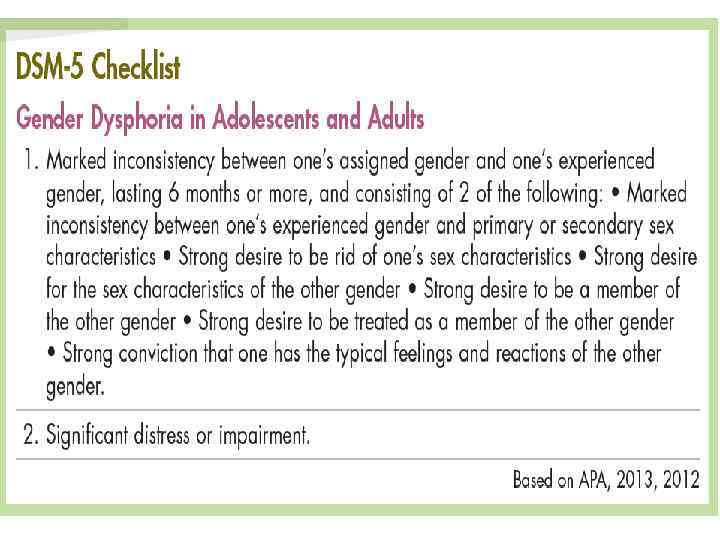
 Gender Dysphoria According to current DSM-5 criteria, people with this disorder persistently feel that they have been assigned to the wrong biological sex, and gender changes would be desirable The DSM-5 categorization of this disorder has become controversial in recent years Many people believe that transgender experiences reflect alternative – not pathological – ways of experiencing one's gender identity Others argue that gender dysphoria is, in fact, a medical problem that may produce personal unhappiness
Gender Dysphoria According to current DSM-5 criteria, people with this disorder persistently feel that they have been assigned to the wrong biological sex, and gender changes would be desirable The DSM-5 categorization of this disorder has become controversial in recent years Many people believe that transgender experiences reflect alternative – not pathological – ways of experiencing one's gender identity Others argue that gender dysphoria is, in fact, a medical problem that may produce personal unhappiness
 Gender Dysphoria The disorder sometimes emerges in childhood and disappears with adolescence In some cases it develops into adult gender dysphoria Many clinicians suspect biological – perhaps genetic or prenatal – factors Abnormalities in the brain, including the hypothalamus (particularly the bed nucleus of stria terminalis), are a potential link
Gender Dysphoria The disorder sometimes emerges in childhood and disappears with adolescence In some cases it develops into adult gender dysphoria Many clinicians suspect biological – perhaps genetic or prenatal – factors Abnormalities in the brain, including the hypothalamus (particularly the bed nucleus of stria terminalis), are a potential link
 Gender Dysphoria To more effectively assess and treat those with the disorder, clinical theorists have tried to distinguish the most common patterns of gender dysphoria: Female-to-male Male-to-female: Androphilic Type Male-to-female: Autogyneophilic Type Many adults with GD receive psychotherapy Some adults with this disorder change their sexual characteristics by way of hormones; others opt for sexual reassignment (sex change) surgery
Gender Dysphoria To more effectively assess and treat those with the disorder, clinical theorists have tried to distinguish the most common patterns of gender dysphoria: Female-to-male Male-to-female: Androphilic Type Male-to-female: Autogyneophilic Type Many adults with GD receive psychotherapy Some adults with this disorder change their sexual characteristics by way of hormones; others opt for sexual reassignment (sex change) surgery
 Gender Identity Disorder Formerly known as transsexualism Individuals feel that they are of the opposite sex Despite normal genitals Feelings usually present since childhood May seek out surgery to alter body Feelings must cause distress or impairment or no diagnosis is given Individuals with GID may be sexually attracted to same or opposite sex individuals Prevalence: 1 in 12, 000 in men 1 in 30, 000 in women 86
Gender Identity Disorder Formerly known as transsexualism Individuals feel that they are of the opposite sex Despite normal genitals Feelings usually present since childhood May seek out surgery to alter body Feelings must cause distress or impairment or no diagnosis is given Individuals with GID may be sexually attracted to same or opposite sex individuals Prevalence: 1 in 12, 000 in men 1 in 30, 000 in women 86
 Gender Identity Disorder Controversial diagnostic category Should it be a psychiatric disorder? Diagnosis pathologizes a natural diversity found in nature Also carries stigma GID can be diagnosed in children Cross-gender behaviors common in kids Most children with GID grow up to be comfortable with their biological sex without professional intervention 87
Gender Identity Disorder Controversial diagnostic category Should it be a psychiatric disorder? Diagnosis pathologizes a natural diversity found in nature Also carries stigma GID can be diagnosed in children Cross-gender behaviors common in kids Most children with GID grow up to be comfortable with their biological sex without professional intervention 87
 Etiology of Gender Disorder Genetic factors Neurobiological factors symptoms of gender identity during childhood are at least moderately heritable Exposure to high levels of sex hormones in utero Social and psychological factors Reinforcement of cross gender behaviors 88
Etiology of Gender Disorder Genetic factors Neurobiological factors symptoms of gender identity during childhood are at least moderately heritable Exposure to high levels of sex hormones in utero Social and psychological factors Reinforcement of cross gender behaviors 88
 Treatment of Gender Identity Disorder Sex reassignment surgery Genitalia altered to look like those of opposite sex 1 year living as opposite sex before surgery recommended Behavioral treatment to alter gender identity Shaping of more masculine behaviors May only be effective for individuals who want treatment for GID 89
Treatment of Gender Identity Disorder Sex reassignment surgery Genitalia altered to look like those of opposite sex 1 year living as opposite sex before surgery recommended Behavioral treatment to alter gender identity Shaping of more masculine behaviors May only be effective for individuals who want treatment for GID 89
 Summary of Sexual and Gender Identity Disorders Gender Identity and Gender Identity Disorder Problem is not sexual; the problem is feeling trapped in body of wrong sex Sexual Dysfunctions are Common in Men and Women Problems with desire, arousal, and/or orgasm Require comprehensive assessment and treatment approaches Paraphilias Represent Inappropriate Sexual Attraction Desire, arousal, and orgasm gone awry Require comprehensive assessment and treatment approaches
Summary of Sexual and Gender Identity Disorders Gender Identity and Gender Identity Disorder Problem is not sexual; the problem is feeling trapped in body of wrong sex Sexual Dysfunctions are Common in Men and Women Problems with desire, arousal, and/or orgasm Require comprehensive assessment and treatment approaches Paraphilias Represent Inappropriate Sexual Attraction Desire, arousal, and orgasm gone awry Require comprehensive assessment and treatment approaches
 Medication sexual effects
Medication sexual effects
 Neuroleptics Difficulty in achieving or maintaining erection Ejaculatory difficulties") Effects of First Generation (Typical) Neuroleptics Difficulty in achieving or maintaining erection Ejaculatory difficulties Priapism (isolated incidents) Desire & arousal problems Poor lubrication Diminished orgasm Irregular menstruation/ amenorrhea or menorrhagia Gynaecomastia, Galactorrhoea & breast discomfort in both men and women
Effects of First Generation (Typical) Neuroleptics Difficulty in achieving or maintaining erection Ejaculatory difficulties Priapism (isolated incidents) Desire & arousal problems Poor lubrication Diminished orgasm Irregular menstruation/ amenorrhea or menorrhagia Gynaecomastia, Galactorrhoea & breast discomfort in both men and women
 Neuroleptics Significantly lower incidence of EPS and sexual sideeffects") Effect of Second Generation (Atypical) Neuroleptics Significantly lower incidence of EPS and sexual sideeffects Risperidone associated with Galactorrhoea Olanzapine & Clozapine cause fewer sexual sideeffects (negligible effect on prolactin levels)
Effect of Second Generation (Atypical) Neuroleptics Significantly lower incidence of EPS and sexual sideeffects Risperidone associated with Galactorrhoea Olanzapine & Clozapine cause fewer sexual sideeffects (negligible effect on prolactin levels)
 Effect of Anticholinergic Drugs Can diminish some side effects Can cause erectile dysfunction Failure of vaginal lubrication
Effect of Anticholinergic Drugs Can diminish some side effects Can cause erectile dysfunction Failure of vaginal lubrication
 Treatment of medication- induced sexual dysfunction Assess that there is no other physical pathology Spontaneous remission may occur Dose reduction Change medication ‘Antidote’ medication eg. Viagra
Treatment of medication- induced sexual dysfunction Assess that there is no other physical pathology Spontaneous remission may occur Dose reduction Change medication ‘Antidote’ medication eg. Viagra
 Treatment of medication- induced sexual dysfunction Yohimbine- an alkaloid from the bark of Corynanthe yohimbi Its efficacy in treating sexual dysfunction may be associated with ability to block presynaptic alpha-2 adrenergic sites, leading to enhanced adrenergic tone Typical side effects associated with yohimbine include anxiety, nausea, flushing, tremor, hypertension, chest pain, urinary urgency, priapism, sweating Yohimbine may affect medications such as warfarin and antihypertensive medications
Treatment of medication- induced sexual dysfunction Yohimbine- an alkaloid from the bark of Corynanthe yohimbi Its efficacy in treating sexual dysfunction may be associated with ability to block presynaptic alpha-2 adrenergic sites, leading to enhanced adrenergic tone Typical side effects associated with yohimbine include anxiety, nausea, flushing, tremor, hypertension, chest pain, urinary urgency, priapism, sweating Yohimbine may affect medications such as warfarin and antihypertensive medications
 Buspirone - a serotonin-IA partial agonist typically prescribed to treat persistent anxiety. Most patients using buspirone to treat sexual dysfunction take it daily. The dosage is the same as that used for anxiety (15 mg to 60 mg daily) The mechanism of action of buspirone in treating sexual dysfunction may be reduction of serotonergic tone via stimulation of presynaptic autoreceptors or the alpha-2 antagonist effects of one of buspirone's major metabolites, 1 -pyrimidinylpiperazine Mirtazapinemight also be effective in reversing sexual side effects. The putative capacity of mirtazapine to reverse sexual side effects can be attributed either to their serotonergic activity or presynaptic alpha-2 activity Amantadine a dopamine agonist, is used both as an antiviral agent and as a treatment for , Parkinson's disease. It has been shown in a number of small case series to reverse anorgasmia Bupropion is another commonly touted antidote for SSRI-induced sexual dysfunction. It is assumed that the mechanism of action by which bupropion reverses sexual side effects is its weak dopamine agonism. Libido, arousal, and orgasmic difficulties were all effectively reversed Stimulants such as methylphenidate, D-amphetamine, and pemoline, are reported to , reverse a variety of sexual side effects caused by SSRIs. Low doses of 10 mg-25 mg of methylphenidate or D-amphetamine have been effective
Buspirone - a serotonin-IA partial agonist typically prescribed to treat persistent anxiety. Most patients using buspirone to treat sexual dysfunction take it daily. The dosage is the same as that used for anxiety (15 mg to 60 mg daily) The mechanism of action of buspirone in treating sexual dysfunction may be reduction of serotonergic tone via stimulation of presynaptic autoreceptors or the alpha-2 antagonist effects of one of buspirone's major metabolites, 1 -pyrimidinylpiperazine Mirtazapinemight also be effective in reversing sexual side effects. The putative capacity of mirtazapine to reverse sexual side effects can be attributed either to their serotonergic activity or presynaptic alpha-2 activity Amantadine a dopamine agonist, is used both as an antiviral agent and as a treatment for , Parkinson's disease. It has been shown in a number of small case series to reverse anorgasmia Bupropion is another commonly touted antidote for SSRI-induced sexual dysfunction. It is assumed that the mechanism of action by which bupropion reverses sexual side effects is its weak dopamine agonism. Libido, arousal, and orgasmic difficulties were all effectively reversed Stimulants such as methylphenidate, D-amphetamine, and pemoline, are reported to , reverse a variety of sexual side effects caused by SSRIs. Low doses of 10 mg-25 mg of methylphenidate or D-amphetamine have been effective
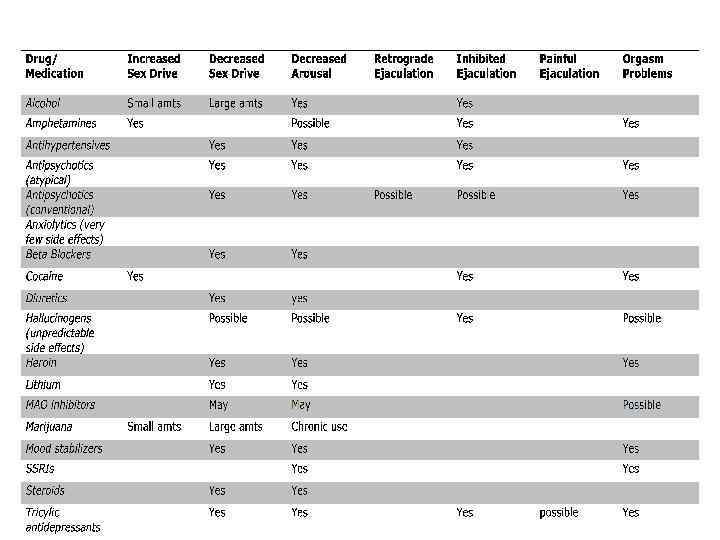
 Thank you!
Thank you!