6fe229b5ebca6e9bd2a09bdc769c98d3.ppt
- Количество слайдов: 54



Diabetes Management in the Outpatient Setting
 • FPG≥ 126 mg/dl. • Prediabetes (IFG)≥ 100 mg/dl. •")
Diagnostic Criteria (before 2010) • FPG≥ 126 mg/dl. • Prediabetes (IFG)≥ 100 mg/dl. • 75 gram OGTT 2 hour-value≥ 200 mg/dl. • Prediabetes (IGT)≥ 140 mg/dl. • Random blood glucose≥ 200 mg/dl + symptoms (polyuria, polydipsia, unexplained weight loss).

International Expert Committee Report on the Role of A 1 C in the Diagnosis of Diabetes 6. 5% THE INTERNATIONAL EXPERT COMMITTEE. Diabetes Care 2009; 32: 1327

2010 Diagnosis of Diabetes and Categories of Increased Risk for Diabetes NORMAL IFG or IGT DIABETES FPG < 100 mg/dl IFG FPG > 100 - 125 mg/dl FPG > 126 mg/dl 2 -h PG < 140 mg/dl IGT 2 -h PG > 140 199 mg/dl 2 -h PG > 200 mg Random PG > 200 + symptoms A 1 C 5. 7% to 6. 4% ≥ 6. 5% ADA, Diabetes Care 33: Suppl. 1, S 11 -S 61, 2010

Main factors in support of using Hb. A 1 C as a screening and diagnostic test • A 1 c does not require patients to be fasting. • Hb. A 1 c reflects longer-term glycemia than does plasma glucose. • Relatively unaffected by acute (e. g. , stress or illness related) perturbations in glucose levels. • Currently used to guide management and adjust therapy. • Hb. A 1 c laboratory methods are now well standardized and reliable. J Clin Endocrinol Metab 93: 2447– 2453, 2008 Diabetes Care 32 (7): 1327 -1334, 2009

Limitations of the Use of A 1 C for the Diagnosis of Diabetes • Greater cost • Limited availability of A 1 C testing in certain regions of the developing world • Incomplete correlation between A 1 C and average glucose • Misleading in patients with anemia and hemoglobinopathies.

Factors influencing A 1 c

Recommendation of the International Expert Committee for the diagnosis of diabetes • Diabetes should be diagnosed when A 1 C is ≥ 6. 5% • Diagnosis should be confirmed with a repeat A 1 C test • Confirmation is not required in symptomatic subjects with plasma glucose levels >200 mg/dl • If A 1 C testing is not possible, previously recommended diagnostic methods (e. g. , FPG or 2 HPG, with confirmation) are acceptable. DIABETES CARE, VOLUME 32, NUMBER 7, JULY 2009

Who To Screen • No major risk factors, FPG every 3 years beginning at 45 y. o. • Any risk factors, screen earlier and more often: • Overweight (BMI>25 kg/m 2). • First degree relative with T 2 DM. • High risk ethnic group. • Hypertension (≥ 140/90 mm. Hg). • HDL≤ 35 mg/dl and/or triglycerides≥ 250 mg/dl. • History of gestational diabetes or delivered baby ≥ 9 lb. • Polycystic ovary syndrome. • History of vascular disease. • Habitual physical inactivity.

Treatment Goals for Type 2 Diabetes

Guidelines for Glycemic, BP, & Lipid Control American Diabetes Assoc. Goals Hb. A 1 C Preprandial glucose Postprandial glucose Blood pressure Lipids < 7. 0% (individualization) 70 -130 mg/d. L (3. 9 -7. 2 mmol/l) < 180 mg/d. L < 130/80 mm. Hg LDL: < 100 mg/d. L (2. 59 mmol/l) < 70 mg/d. L (1. 81 mmol/l) (with overt CVD) HDL: > 40 mg/d. L (1. 04 mmol/l) > 50 mg/d. L (1. 30 mmol/l) TG: < 150 mg/d. L (1. 69 mmol/l) HDL = high-density lipoprotein; LDL = low-density lipoprotein; PG = plasma glucose; TG = triglycerides. ADA. Diabetes Care. 2012; 35: S 11 -63
 and UKPDS (1998) established role for better")
Standard of Care-Multifactorial Therapy • DCCT (1993) and UKPDS (1998) established role for better glycemic control on prevention of microvascular complications. • Studies that improved BP or lipids generally showed lower CAD in type 2 diabetes. • Steno 2 trial (2003) showed a marked lowering of both micro and macrovascular events when all 3 utilized.
 and UKPDS (1998) established role for better")
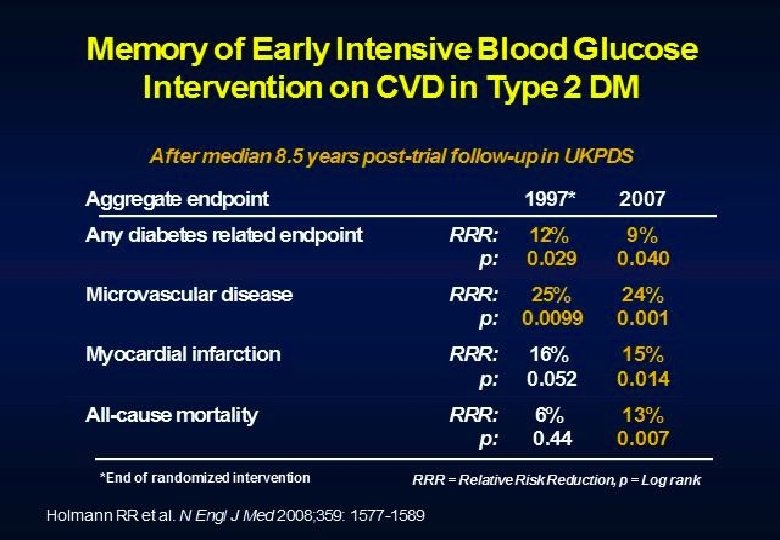
Standard of Care-Multifactorial Therapy • DCCT (1993) and UKPDS (1998) established role for better glycemic control on prevention of microvascular complications. • Studies that improved BP or lipids generally showed lower CAD in type 2 diabetes. • Steno 2 trial (2003) showed a marked lowering of both micro and macrovascular events when all 3 utilized. • Memory effect-longterm micro and macrovascular protection years after stopping the trial-in DCCT, UKPDS, and Steno 2 trials.

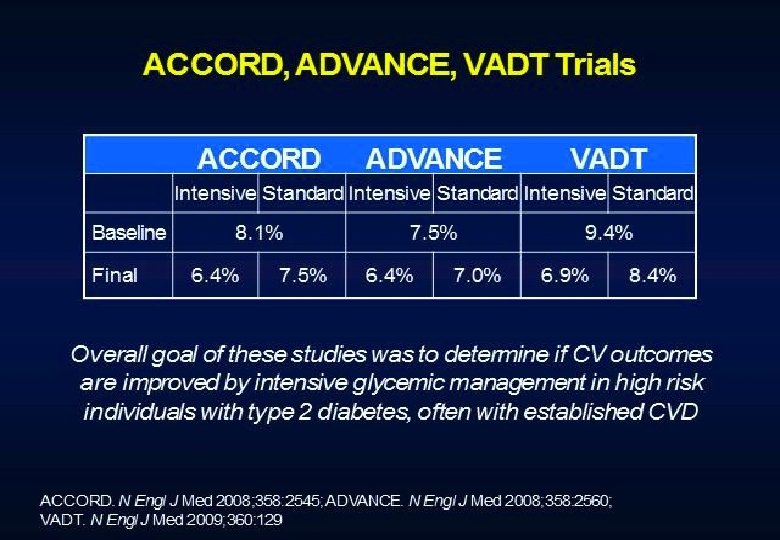
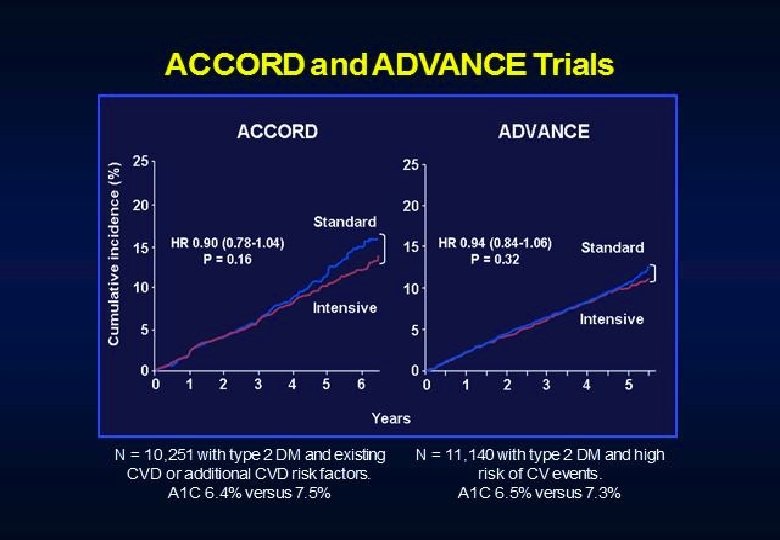
But…then the role of intensive glucose control management came under active debate.
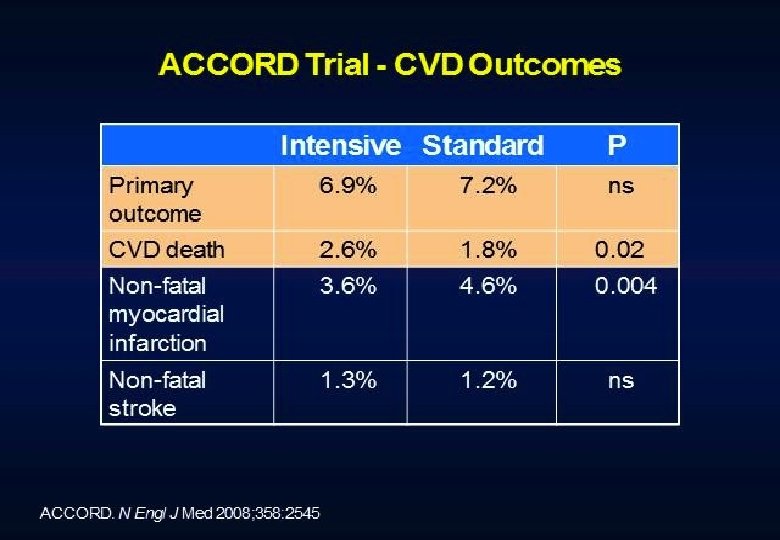
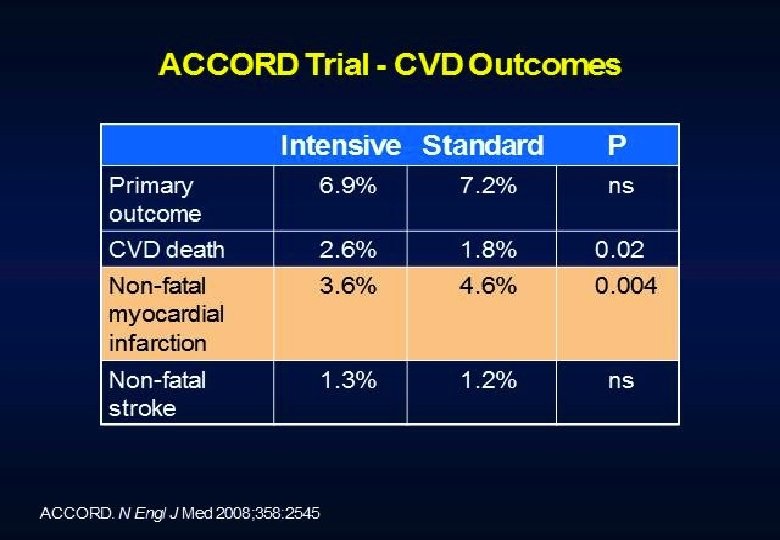

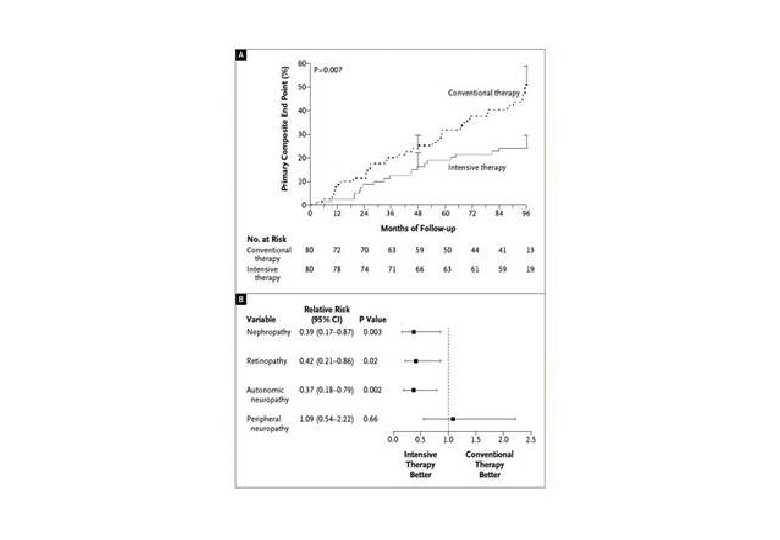
Conclusions Intensive treatment of glycemia in the ACCORD cohort did not reduce the risk of composite measures of advanced microvascular outcomes renal failure: initiation of dialysis or ESRD, or renal transplant, or a rise of serum creatinine above 3. 3 mg/d. L retinal photocoagulation or vitrectomy to treat diabetic retinopathy, or development of neuropathy Intensive therapy delayed the onset of albuminuria and some measures of eye complications and neuropathy Microvascular benefits of intensive therapy should be weighed against increase in total and CVD-related mortality, increased weight gain, and high risk for severe hypoglycemia
![Figure 1 Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print] (Adapted with](https://present5.com/presentation/6fe229b5ebca6e9bd2a09bdc769c98d3/image-22.jpg "Figure 1 Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print] (Adapted with")
Figure 1 Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print] (Adapted with permission from: Ismail-Beigi F, et al. Ann Intern Med 2011; 154: 554)

Main Pathophysiological Defects in T 2 DM pancreatic insulin secretion incretin effect - gut carbohydrate delivery & absorption pancreatic glucagon secretion ? HYPERGLYCEMIA + hepatic glucose production peripheral glucose uptake Adapted from: Inzucchi SE, Sherwin RS in: Cecil Medicine 2011
 Plasma glucose Glucose Carbohydrate Production")
Antihyperglycemic Agents Major Sites of Action Glucosidase Inhibitors (-) Plasma glucose Glucose Carbohydrate Production Absorption Glucose Uptake GI tract Muscle/Fat Sulfonylureas Meglitinides Insulin Secretion (+) Pancreas (-) Liver Injected Insulin (+) Metformin Glitazones Insulin Secretion 1. Hines SE. Intensive management of type 2 diabetes. Patient Care. April 30, 2000: 91 -107. 2. Kelley DB, ed. Medical Management of Type 2 Diabetes. 4 th ed. Alexandria, Va: American Diabetes Association; 1998: 56 -72.

Natural History of Type 2 DM Plasma Glucose Postmeal glucose Fasting glucose 126 mg/d. L Insulin resistance Relative -Cell Function Insulin secretion -30 -20 -10 0 Years of Diabetes De. Fronzo RA. Pathogenesis of type 2 diabetes: Implications for metformin. Drugs. 1999; 58 (suppl 1): 29 -30. 10 20 30

Management of Hyperglycemia in T 2 DM ANTI-HYPERGLYCEMIC THERAPY • Therapeutic options: Lifestyle - Weight optimization - Healthy diet - Increased activity level Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Management of Hyperglycemia in T 2 DM ANTI-HYPERGLYCEMIC THERAPY • Therapeutic options: Oral agents & non-insulin injectables - Metformin - Sulfonylureas - Thiazolidinediones - DPP-4 inhibitors - GLP-1 receptor agonists - Meglitinides - -glucosidase inhibitors - Bile acid sequestrants - Dopamine-2 agonists - Amylin mimetics Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Class Mechanism Advantages Disadvantages Cost Biguanides • Activates AMP-kinase • Hepatic glucose production • Extensive experience • No hypoglycemia • Weight neutral • ? CVD • Gastrointestinal • Lactic acidosis • B-12 deficiency • Contraindications Low SUs / Meglitinides • Closes KATP channels • Insulin secretion • Extensive experience • Microvasc. risk • Hypoglycemia • Weight gain • Low durability • ? Ischemic preconditioning Low TZDs • PPAR-g activator • insulin sensitivity • No hypoglycemia • Durability • TGs, HDL-C • ? CVD (pio) • Weight gain High • Edema / heart failure • Bone fractures • ? MI (rosi) • ? Bladder ca (pio) a-GIs • Inhibits -glucosidase • No hypoglycemia • Gastrointestinal • Slows carbohydrate • Nonsystemic • Dosing frequency absorption • Post-prandial glucose • Modest A 1 c • ? CVD events Table 1. Properties of anti-hyperglycemic agents Mod. Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Class Mechanism Advantages Disadvantages Cost DPP-4 inhibitors • Inhibits DPP-4 • Increases GLP-1, GIP • No hypoglycemia • Well tolerated • Modest A 1 c • ? Pancreatitis • Urticaria High GLP-1 receptor agonists • Activates GLP-1 R • Insulin, glucagon • gastric emptying • satiety • Weight loss • No hypoglycemia • ? Beta cell mass • ? CV protection • GI • ? Pancreatitis • Medullary ca • Injectable High Amylin mimetics • Activates amylin receptor • glucagon • gastric emptying • satiety • Weight loss • PPG • GI • Modest A 1 c • Injectable • Hypo w/ insulin • Dosing frequency High Bile acid sequestrants • Bind bile acids • Hepatic glucose production • No hypoglycemia • GI • Nonsystemic • Modest A 1 c • Post-prandial glucose • Dosing frequency • CVD events High Dopamine-2 agonists • Activates DA receptor • No hypoglyemia • Modulates hypothalamic • ? CVD events control of metabolism • insulin sensitivity Table 1. Properties of anti-hyperglycemic agents • Modest A 1 c High • Dizziness/syncope • Nausea • Fatigue Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Class Insulin Mechanism • Activates insulin receptor • peripheral glucose uptake Advantages • Universally effective • Unlimited efficacy • Microvascular risk Table 1. Properties of anti-hyperglycemic agents Disadvantages • Hypoglycemia • Weight gain • ? Mitogenicity • Injectable • Training requirements • “Stigma” Cost Variable Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Management of Hyperglycemia in T 2 DM ANTI-HYPERGLYCEMIC THERAPY • Implementation strategies: - Initial therapy - Advancing to dual combination therapy - Advancing to triple combination therapy - Transitions to & titrations of insulin Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Management of Hyperglycemia in T 2 DM ANTI-HYPERGLYCEMIC THERAPY • Implementation strategies: • If A 1 c >9% start with 2 meds. • Consider insulin if BS>300 or A 1 c>10% • Adding a second agent drops A 1 c on average 1%. • A 1 c>8. 5% and on 2 drugs=insulin.

Management of Hyperglycemia in T 2 DM CONSIDERATIONS • Age • Weight • Sex / racial / ethnic / genetic differences • Comorbidities - Coronary artery disease Heart Failure Chronic kidney disease Liver dysfunction Hypoglycemia Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Management of Hyperglycemia in T 2 DM CONSIDERATIONS • Age: Older adults - Reduced life expectancy Higher CVD burden Reduced GFR At risk for adverse events from polypharmacy More likely to be compromised from hypoglycemia üLess ambitious targets üHb. A 1 c <7. 5– 8. 0% if tighter targets not easily achieved üFocus on drug safety Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Management of Hyperglycemia in T 2 DM CONSIDERATIONS • Weight - Majority of T 2 DM patients overweight / obese Intensive lifestyle program Metformin GLP-1 receptor agonists ? Bariatric surgery Consider LADA in lean patients Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Management of Hyperglycemia in T 2 DM CONSIDERATIONS • Sex/ethnic/racial/genetic differences - Little is known - MODY & other monogenic forms of diabetes - Latinos: more insulin resistance - East Asians: more beta cell dysfunction - Gender may drive concerns about adverse effects (e. g. , bone loss from TZDs) Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

T 2 DM Anti-hyperglycemic Therapy: General Recommendations Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Adapted Recommendations: When Goal is to Avoid Weight Gain Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Management of Hyperglycemia in T 2 DM CONSIDERATIONS • Comorbidities Ø Metformin: CVD benefit (UKPDS) - Coronary Disease Ø Avoid hypoglycemia - Heart Failure Ø ? SUs & ischemic preconditioning - Renal disease - Liver dysfunction Ø ? Pioglitazone & CVD events Ø ? Effects of incretin-based therapies - Hypoglycemia Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Management of Hyperglycemia in T 2 DM CONSIDERATIONS • Comorbidities - Coronary Disease - Heart Failure - Renal disease - Liver dysfunction Ø Metformin: May use unless condition is unstable or severe Ø Avoid TZDs Ø ? Effects of incretin-based therapies - Hypoglycemia Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Management of Hyperglycemia in T 2 DM CONSIDERATIONS • Comorbidities - Coronary Disease - Heart Failure Ø Increased risk of hypoglycemia - Renal disease Ø Metformin & lactic acidosis - Liver dysfunction - Hypoglycemia § US: stop @SCr ≥ 1. 5 (1. 4 women) § UK: dose @GFR <45 & stop @GFR <30 Ø Caution with SUs (esp. glyburide) Ø DPP-4 -i’s – dose adjust for most Ø Avoid exenatide if GFR <30 Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Management of Hyperglycemia in T 2 DM CONSIDERATIONS • Comorbidities - Coronary Disease - Heart Failure - Renal disease - Liver dysfunction - Hypoglycemia Ø Most drugs not tested in advanced liver disease Ø Pioglitazone may help steatosis Ø Insulin best option if disease severe Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Management of Hyperglycemia in T 2 DM CONSIDERATIONS • Comorbidities - Coronary Disease - Heart Failure - Renal disease - Liver dysfunction - Hypoglycemia Ø Emerging concerns regarding association with increased mortality Ø Proper drug selection in the hypoglycemia prone Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

T 2 DM Anti-hyperglycemic Therapy: General Recommendations Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Diabetes Care, Diabetologia. 19 April 2012 Adapted Recommendations: When Goal is to Avoid Hypoglycemia [Epub ahead of print]

Adapted Recommendations: When Goal is to Minimize Costs Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
 Physiologic Insulin Secretion : Basal/Bolus Concept 50 Prandial Insulin 25 0")
Insulin (µU/m. L) Physiologic Insulin Secretion : Basal/Bolus Concept 50 Prandial Insulin 25 0 Basal Insulin Breakfast Glucose (mg/d. L) 150 Lunch Supper Prandial Glucose 100 50 Basal Glucose 0 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 A. M. P. M. Time of Day § Suppresses Glucose Production Between Meals & Overnight § Basal 50% of Daily Needs

Management of Hyperglycemia in T 2 DM ANTI-HYPERGLYCEMIC THERAPY Therapeutic options: Insulin level Rapid (Lispro, Aspart, Glulisine) Short (Regular) Intermediate (NPH) Long (Detemir) Long (Glargine) 0 2 4 6 8 Hours 10 12 14 16 18 20 22 24 Hours after injection

Establishing Basal Requirement for Glargine Initial calculation of basal dose • BW in kilograms x sensitivity index (0. 15 – 0. 2 ) Or • Body Weight in pounds x 0. 1 From BID NPH Take total NPH dose and decrease by 20% for starting dose

Establishing Basal Requirement for Glargine • Sequential increase • Increase every 2 -3 days by 4 U if FBG>140 mg/d. L 2 U if FBG=120 mg/d. L to 140 mg/d. L OR • Mean of am BG after five days • Add to initial Glargine by formula (Average BG-100)/10 • • Example: 200 pounds on 20 units glargine q hs, mean am BG is 200 on 6 th and 7 th day Add (Av BG -100)10 to glargine, (200 -100/10) i. e. increase from 20 to 30 units q hs 2 nd week--average 130 , increase glargine from 30 to 33

Establishing Basal Requirement for Glargine • Sequential increase • Increase every 2 -3 days by 4 U if FBG>140 mg/d. L 2 U if FBG=120 mg/d. L to 140 mg/d. L OR • Mean of am BG after five days • Add to initial Glargine by formula (Average BG-100)/10 • • Example: 200 pounds on 20 units glargine q hs, mean am BG is 200 on 6 th and 7 th day Add (Av BG -100)10 to glargine, (200 -100/10) i. e. increase from 20 to 30 units q hs 2 nd week--average 130 , increase glargine from 30 to 33

Sequential Insulin Strategies in T 2 DM Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Management of Hyperglycemia in T 2 DM ANTI-HYPERGLYCEMIC THERAPY • Glycemic targets - Hb. A 1 c < 7. 0% (mean PG 150 -160 mg/dl [8. 3 -8. 9 mmol/l]) - Pre-prandial PG <130 mg/dl (7. 2 mmol/l) - Post-prandial PG <180 mg/dl (10. 0 mmol/l) - Individualization is key: Ø Tighter targets (6. 0 - 6. 5%) - younger, healthier Ø Looser targets (7. 5 - 8. 0%+) - older, comorbidities, hypoglycemia prone, etc. PG = plasma glucose Avoidance of hypoglycemia Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Management of Hyperglycemia in T 2 DM KEY POINTS • Glycemic targets & BG-lowering therapies must be individualized. • Diet, exercise, & education: foundation of any T 2 DM therapy program • Unless contraindicated, metformin = optimal 1 st-line drug. • After metformin, data are limited. Combination therapy with 1 -2 other oral / injectable agents is reasonable; minimize side effects. • Ultimately, many patients will require insulin therapy alone / in combination with other agents to maintain BG control. • All treatment decisions should be made in conjunction with the patient (focus on preferences, needs & values. ) • Comprehensive CV risk reduction - a major focus of therapy.
6fe229b5ebca6e9bd2a09bdc769c98d3.ppt