Diabetes Mellitus.Happa.ppt
- Количество слайдов: 42



Diabetes Charith Kumara Group-14 KSMU.

Diabetes Mellitus Disease in which the body doesn’t produce or properly use insulin, leading to hyperglycemia.

Carbohydrate Digestion

Insulin Secretion

What goes wrong in diabetes? ¡ Multitude of mechanisms l Insulin Regulation ¡ Secretion ¡ Uptake or breakdown ¡ l Beta cells ¡ damage

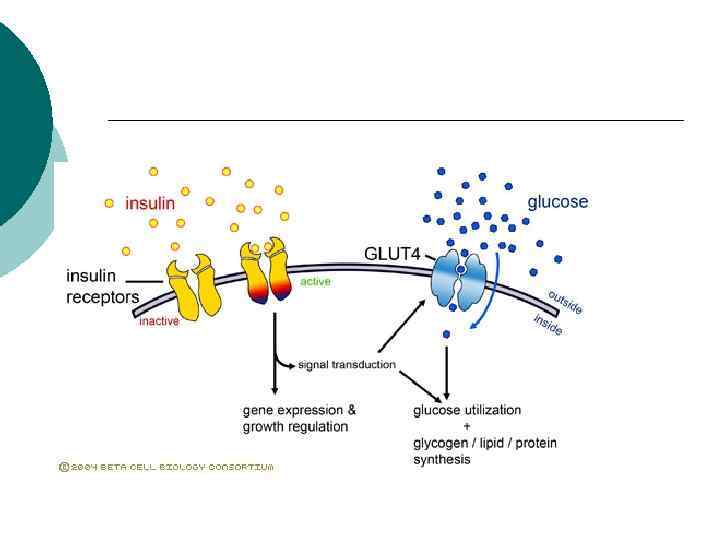
Action of Insulin on the Cell Metabolism

Action of Insulin on Carbohydrate, Protein and Fat Metabolism ¡ Carbohydrate Facilitates the transport of glucose into muscle and adipose cells ¡ Facilitates the conversion of glucose to glycogen for storage in the liver and muscle. ¡ Decreases the breakdown and release of glucose from glycogen by the liver ¡

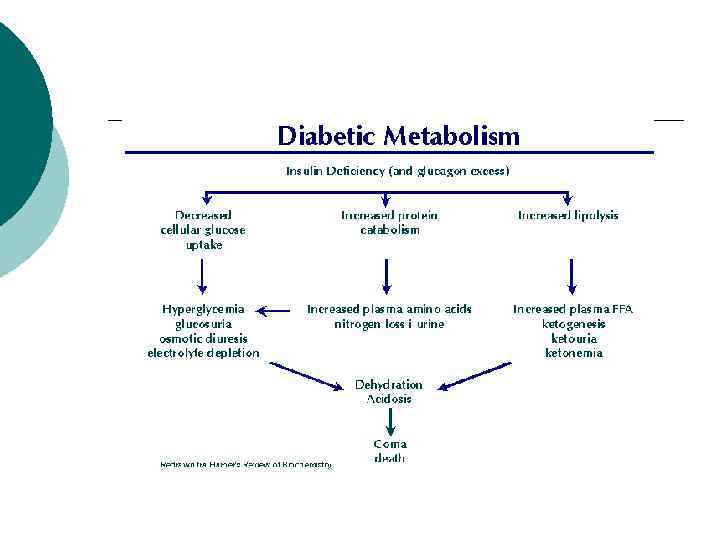
Action of Insulin on Carbohydrate, Protein and Fat Metabolism ¡ Protein Stimulates protein synthesis ¡ Inhibits protein breakdown; diminishes gluconeogenesis ¡

Action of Insulin on Carbohydrate, Protein and Fat Metabolism ¡ Fat Stimulates lipogenesis- the transport of triglycerides to adipose tissue ¡ Inhibits lipolysis – prevents excessive production of ketones or ketoacidosis ¡

Type I Diabetes Low or absent endogenous insulin ¡ Dependent on exogenous insulin for life ¡ Onset generally < 30 years ¡ 5 -10% of cases of diabetes ¡ Onset sudden ¡ l Symptoms: 3 P’s: polyuria, polydypsia, polyphagia

Type I Diabetes Cell

Type I Diabetes ¡ Genetic component to disease

Type II Diabetes ¡ Insulin levels may be normal, elevated or depressed l l l ¡ Characterized by insulin resistance, diminished tissue sensitivity to insulin, and impaired beta cell function (delayed or inadequate insulin release) Often occurs >40 years

Type II Diabetes

Type II Diabetes Risk factors: family history, sedentary lifestyle, obesity and aging ¡ Controlled by weight loss, oral hypoglycemic agents and or insulin ¡

Screening for Diabetes

Management of Diabetes Mellitus ¡ Nutrition ¡ Blood glucose ¡ Medications ¡ Physical activity/exercise ¡ Behavior modification

Medical Nutrition Therapy ¡Primary Goal – improve metabolic control ¡ Blood glucose ¡ Lipid (cholesterol) levels

Medical Nutrition Therapy Maintain short and long term body weight ¡ Reach and maintain normal growth and development ¡ Prevent or treat complications ¡ Improve and maintain nutritional status ¡ Provide optimal nutrition for pregnancy ¡

Nutritional Management for Type I Diabetes ¡Consistency and timing of meals ¡Timing of insulin ¡Monitor blood glucose regularly

Nutritional Management for Type II Diabetes Weight loss ¡ Smaller meals and snacks ¡ Physical activity ¡ Monitor blood glucose and medications ¡

Diabetes Control and Complications Trial 10 year randomized, controlled, clinical trial ¡ Determine the effects of glucose control on the development of long term microvascular and neurologic complications in persons with type I diabetes. ¡ 1441 participants, ages 13 to 39 ¡

Diabetes Control and Complications Trial ¡ Conventional l 1 - 2 insulin injections, self monitoring B. G routine contact with MD and case manager 4 X/year. ¡ Intensive l l therapy: 3 or more insulin injections, with adjustments in dose according to B. G monitoring, planned dietary intake and anticipated exercise.

Diabetes Control and Complications Trial ¡ Results: l l ¡ 76% 60% 54% 39% reduction in in retinopathy neuropathy albuminuria microalbuminuria Implication: Improved blood glucose control also applies to person with type II diabetes.

Nutrition Recommendations ¡ Carbohydrate l ¡ 60 -70% calories from carbohydrates and monounsaturated fats Protein l 10 -20% total calories

Nutrition Recommendations ¡ Fat l l l ¡ Fiber l ¡ <10% calories from saturated fat 10% calories from PUFA <300 mg cholesterol 20 -35 grams/day Alcohol l l Type I – limit to 2 drinks/day, with meals Type II – substitute for fat calories

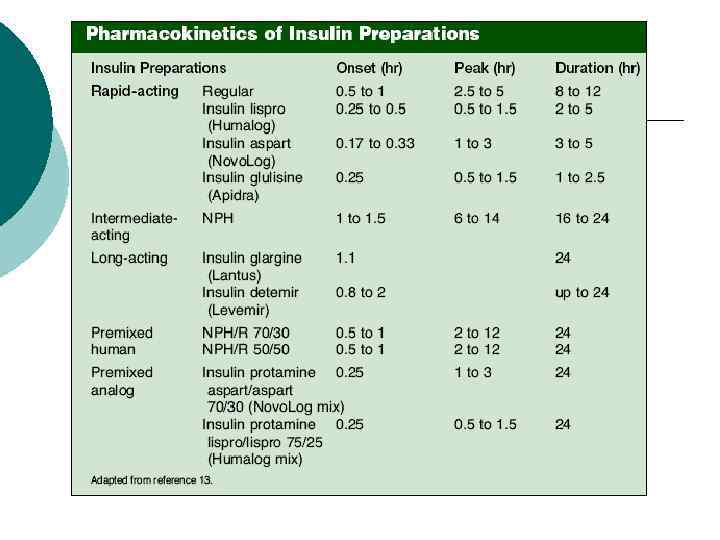
Types of Insulins • • • Regular insulins Insulin analogs Pre-mixed insulin • Short peptide mimics
, Novalin® (from yeast)")
Regular insulins: ¡ ¡ ¡ Human insulin: Humulin® (from E. coli), Novalin® (from yeast) NPH - neutral protamine Hagedorn (NPH), protamine mixed. Lente® insulin / Ultralente® insullinzinc added
 (1996) ¡ Insulin")
Insulin Analogs: ¡ Fatty Acid Acylated insulins ¡ Insulin Lispro (Humalog®) (1996) ¡ Insulin Aspart (Novo. Log®) (2000) ¡ Insulin Glargine (Lantus®) (2002) ¡ Insulin Detemir (Levemir®) (Jun. , 2005) ¡ Insulin Glulisine (Apidra®) (Jan. , 2006)

Amino Acid Substitutons A- chain Position B- chain Position Source/ Type A 21 B 3 B 28 B 29 B 30 Human Asn Pro Lys Thr Aspart Asn Aspartic Lys acid Thr Lispro Asn Glulisine Asn Glargine Gly B 31 And B 32 Detemir Lys Pro Thr Pro Glu Thr Pro Lys Thr Lys Myristic acid rapid-acting Arg long-acting

Diabetes – Oral Medications 6 Classes : ¡ ¡ ¡ Sulfonylureas Biguanides Sulfonylureas and biguanide combination drugs Thiazolidinediones Alpha-glycosidase inhibitors Meglitinides

Sulfonylureas : stimulate β cells to produce more insulin ¡ 1 st generation l l l 2 -(p-aminobenzenesulfonamido)-5 -isopropyl - (1)Orinase (tolbutamide) thiadiazole (IPTD) was used in treatment of typhoid fever in 1940’s hypoglycemia Currently > 12, 000 (3)Tolinase (tolazamide) (6)Diabinese (chlorpropamide) may become dislodged delayed activity ¨ 2 nd generation – (75)Glucotrol – – – (glipizide) (150)Glucotrol XL (ex. rel. glipizide) (150)Micronase, Diabeta (glyburide) (250)Glynase (micronized glyburide) ¨ 3 rd generation – (350)Amaryl (glimepiride) *Hydroxylation of the aromatic ring appears to be the most favored metabolic pathway *Hydroxylated derivatives have much lower hypoglycemic activity

Mechanism of Action Sulfonylureas interact with receptors on pancreatic b-cells to block ATP-sensitive potassium channels ¡ This, in turn, leads to opening of calcium channels ¡ Which leads to the production of insulin ¡
 ¡ Metformin")
Biguanides : improves insulin’s ability to move glucose into cells (esp. muscle) ¡ Metformin - Glucophage®, Fortamet®, Riomet® - mechanism improves insulin sensitivity by increasing peripheral glucose uptake and utilization. - Zhou et al (2001) showed that metformin stimulates the hepatic enzyme AMP-activated protein kinase - Metformin was first described in the scientific literature in 1957 (Unger et al). - It was first marketed in France in 1979 but did not receive FDA approval for Type 2 diabetes until 1994. Metformin is a widely used monotherapy, and also used in combination with the sulfonylureas in treatment of type 2 diabetes *only anti-diabetic drug that has been proven to reduce the complications of diabetes, as evidenced in a large study of overweight patients with diabetes (UKPDS 1998).
 : make cells more sensitive to insulin (esp. fatty cells) ¡ Pioglitazone")
Thiazolidinediones (TZD’s) : make cells more sensitive to insulin (esp. fatty cells) ¡ Pioglitazone - Actos®, Avandia® - binds to and activates the gamma isoform of the peroxisome proliferator-activated rec - PPARγ is a member of the steroid hormone nuclear receptor superfamily, and is found cardiac and skeletal muscle, liver and placenta - upon activation of this nuclear receptor by a ligand such as a TZD, PPARγ–ligand complex binds to a specific region of DNA and thereby regulates the transcription of many genes involved in glucose and fatty acid metabolism. - Marketed in USA in August of 1999 PPAR - γ

Αlpha – glycosidase inhibitors : Block enzymes that help digest starches slowing the rise in B. G. L. ¡ AGI’s - Precose ® (acarbose), - Glyset ® (miglitol)

Meglitinides : Stimulate more insulin production ; dependant upon level of glucose present ¡ Meglitinides - Prandin ® (repaglinide) - Starlix ® (nateglinide)

Diabetes – Oral Medications Summary 6 Classes : ¡ ¡ ¡ Sulfonylureas stimulate β cells Biguanides improves insulin’s ability to move glucose Sulfonylureas and biguanide combination drugs BOTH Thiazolidinediones cells more sensitive to insulin Alpha-glycosidase inhibitors Block enzymes that help digest starches ¡ Meglitinides stimulate β cells (dependant upon glucose conc. )
 ¡ Type 1")
In Conclusion : 2 major types of diabetes (3 with Gestational) ¡ Type 1 => insulin dependant (510%) ¡ Type 2 => may treat with oral medication which may alter insulin production &/or sensitivity ; disease often succumbs to insulin dependence (>90%) ¡
Diabetes Mellitus.Happa.ppt