783a00912ef99b594850df5333a06591.ppt
- Количество слайдов: 89



Diabetes as a Global Health Problem The IDF meets the Challenge By Prof. Morsi Arab IDF Chairman MENA Region

MENA

Reported Incidence of Type 1 Diabetes at the MENA Region per 100. 000 population under 15 yrs ( Diabetes Atlas 2006) • • • • • Afghanistan Algeria Bahrain Egypt Iran Iraq Jordan Kuwait Lebanon Libya Morocco Palestine Oman Pakistan Qatar Saudi Arabia Sudan Tunisia Emirates Yemen 1. 2 8. 6 2. 5 8. 0 3. 7 3. 2 22. 3 3. 2 9. 0 8. 6 3. 2 2. 5 0. 5 11. 4 12. 3 10. 1 7. 3 2. 5

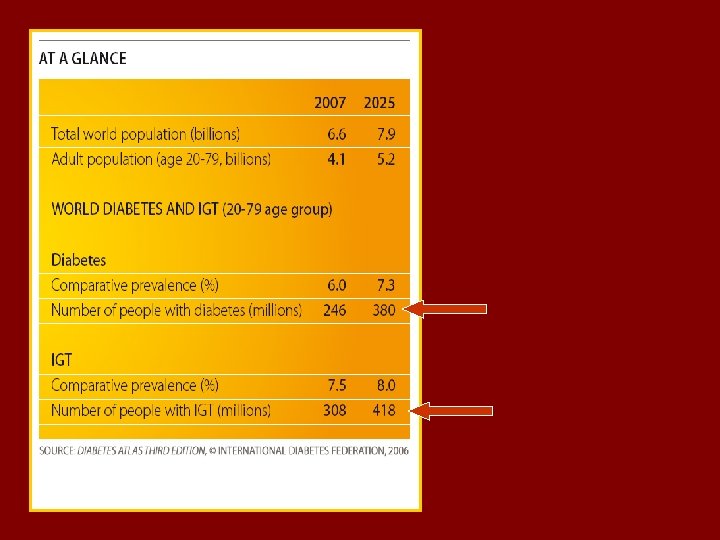
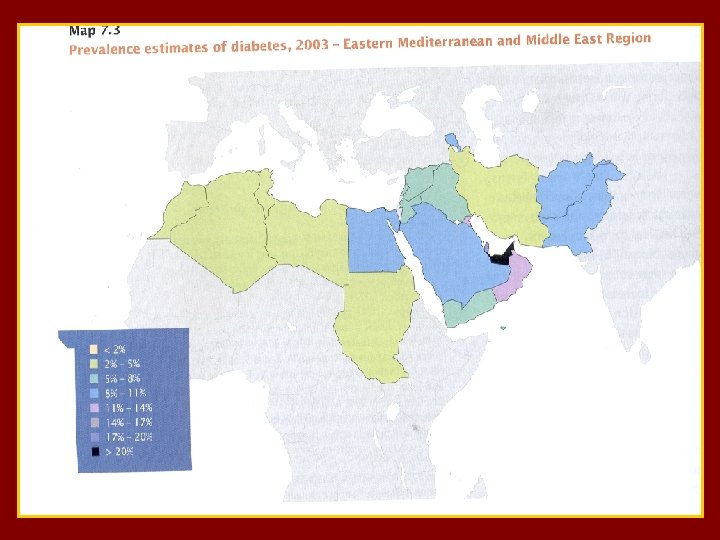
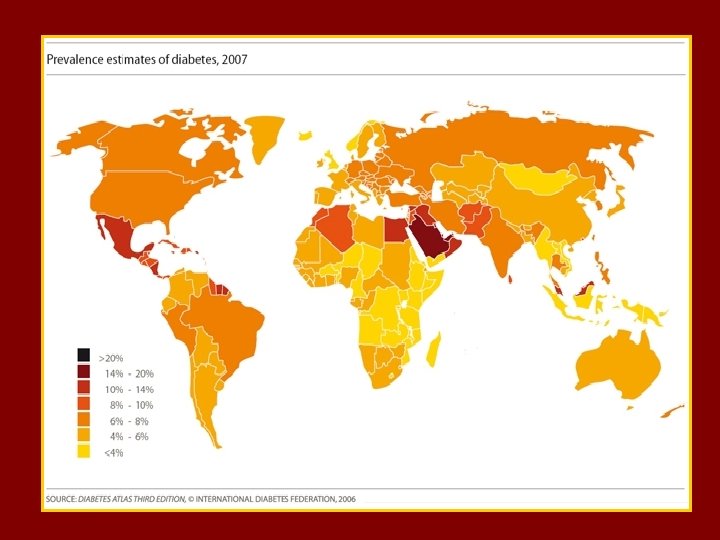
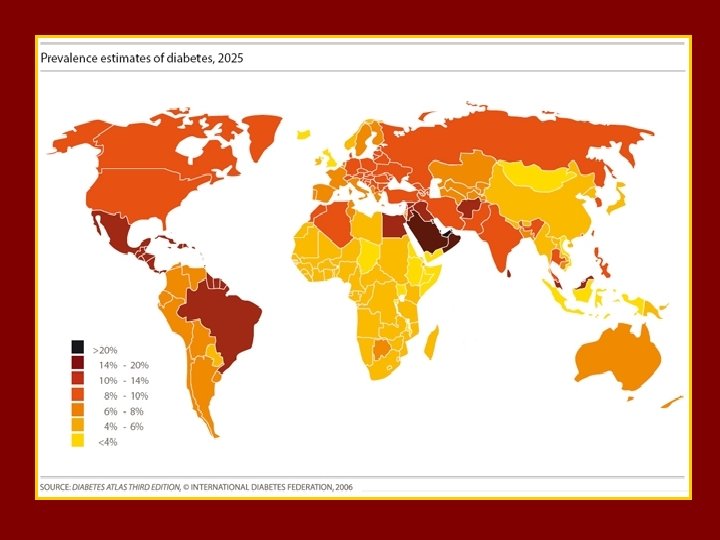
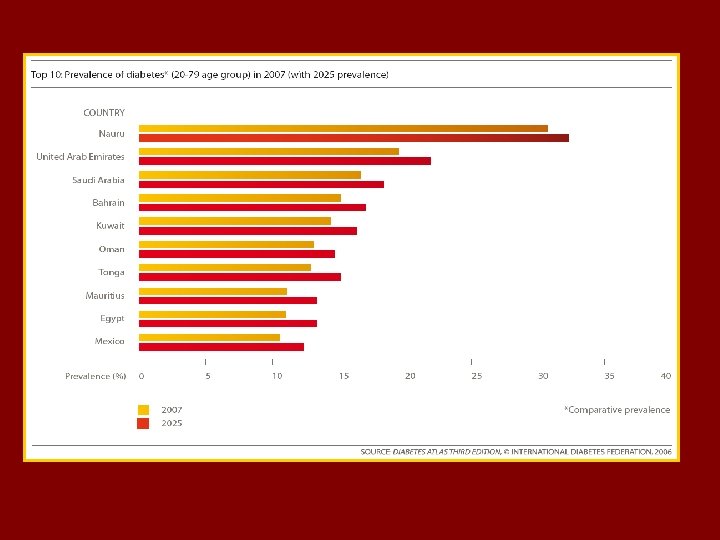
t The MENA Region. A Prevalence of Diabetes is 9. 2 % (age 20 -79) Prevalence of IGT ……. is 8. 1 % 24. 5 millions with Diabetes & 22. 4 with IGT out of the top 10 highest diabetes prevalence rate countries 6 are MENA countries Estimated death due to DM as % of all deaths is 11. 5% ( 11. 1% in Europe and 11. 8 % in MENA )

Diabetes Mortality World wide = 3. 2 millions die from complications associated with diabetes In the ME : ( with high prev. of diab. ) one in 4 deaths in adults 35 -64 years is related to diabetes

MENA

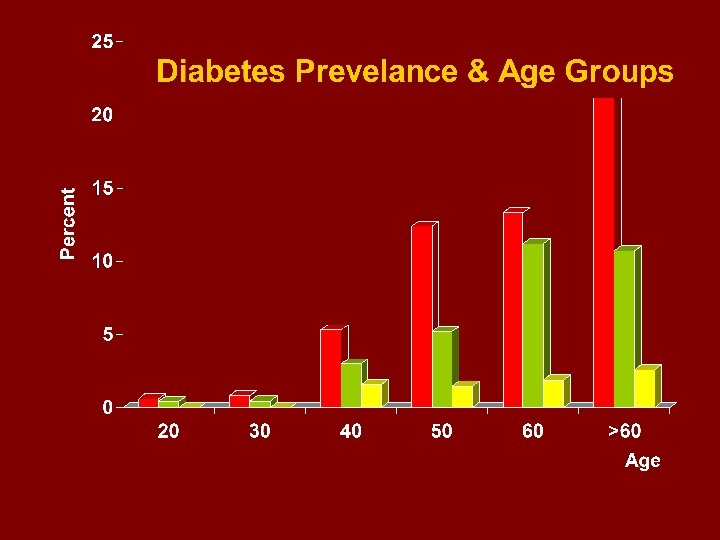
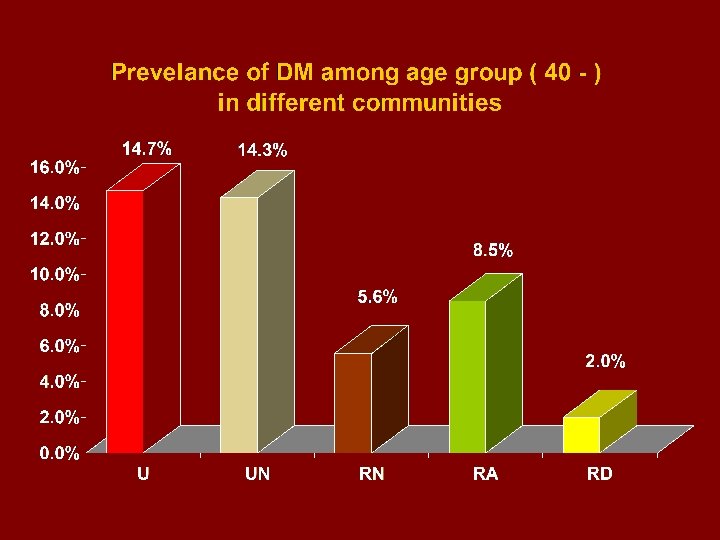
> 60 -50 - 40 -30 -20 -10 The pyramidal structure of the Egyptian population

Age Group 10 20 30 40 50 60

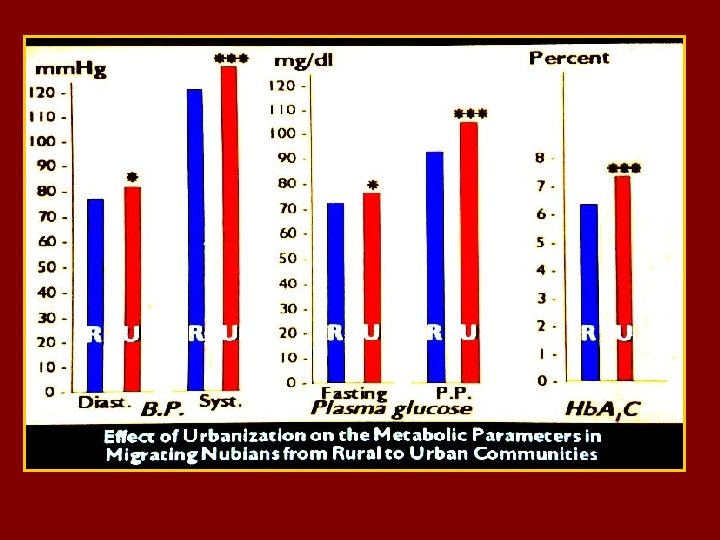
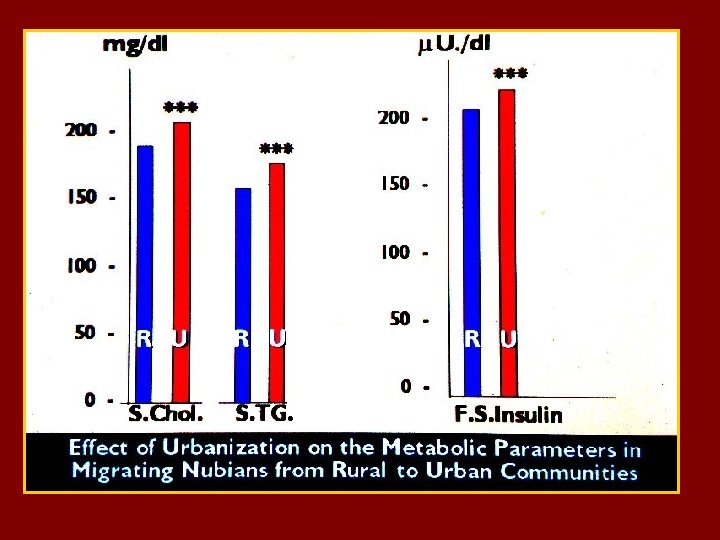
Saini Eastern desert Western desert Nubia

DIABETES IS PART OF THE WIDER HEALTH PROBLEM : THE METABOLIC SYNDROME 20 -25 % of the world adult population have the metabolic syndrome ( MTS) , and these are : - 5 times at risk to develop diabetes type 2 - 3 times likely to have a heart attack or stroke - twice likely to die

Obesity” is always involved , or associated with all elements of the Metabolic Syndrome : But Which type of Obesity ?

“ Abdominal Obesity “ as measured by waist circumference is more indicative of the Metabolic Syndrome profile than increased BMI

 definition According to the new IDF definition ,")
The new international Diabetes Federation (IDF) definition According to the new IDF definition , for a person to be defined as having the metabolic syndrome he/she must have : Central Obesity ( defined as waist circumference * with ethnicity specific values ) plus any two of the following four factors : Raised triglycerides 150 mg/d. L (1. 7 mmol/L ) or specific treatment for this lipid abnormality. Reduced HDL Cholesterol 40 mg/dl ( 1. 03 mmol/L ) in males 50 mg/d. L (1. 29 mmol/L) in females or specific treatment for this lipid abnormality Raised blood pressure Systolic BP 130 or diastolic BP 85 mm. Hg Or treatment of previously diagnosed hypertension Raised fasting plasma glucose ( FPG) 100 mg/d. L (5. 6 mmol/L) or previously diagnosed type 2 diabetes

Diabetes Mellitus and its state of control and complications in the MENA Region
 - Uncontrolled = 19. 8 %")
Fasting Hyperglycemia - Controlled (< 120 mg/dl ) - Uncontrolled = 19. 8 % = 80. 2 % ----------------- Hyperglycemic 121 -150 mg/dl Marked hyperglycemia -200 Severe hyperglycemia -220 Very severe hyperglycemia > 220 = 15. 6 % = 31. 3 % = 12. 5 % = 20. 8 %

Hyperglycemia Fasting 120 mg/dl

Post Prandial Hyperglycemia - Controlled < 160 mg/dl 180 mg/dl = 7. 9 % Total = 13. 5 % = 21. 4 % - Uncontrolled ( >180 mg/dl ) = 78. 6 % * Moderate -220 mg/dl = 17. 4 % * Severe - 260 mg/dl = 16. 0 % * Very Severe > 260 mg/dl = 45. 2 %

Hyperglycemia 180 mg/dl

Diastolic Blood Pressure 80 mm Hg

Systolic Blood Pressure 0. 50% 130 mm Hg

Lipid Control Serum Cholesterol 200 mg

Lipid Control Serum Triglycerides 150 mg

Obesity as a Risk Factor for Hyperglycemia , Hypertension and Hyperlipidemia Obesity as BMI group Syst. B. P. > 150 mm Hg (A) < 24 8. 7 % (B) (C) 24 -30 > 30 20. 5 % * 30. 6 % * Diast. B. P. > 80 mm Hg 17. 1 % 32. 9 % * 41. 5 % * S. Cholest. > 200 mg/d. L 19. 7 % 24. 5 % * 50. 4 % * S. Triglycerides >150 mg/d. L 23. 5 % 22. 6 % 54. 9 % * Fasting Bl. Gluc. >120 mg/d. L 72. 3 % 73. 8 % N. B. (%) percentage of patients above the acceptable levels 80. 0 % , (*) Significant

Cardiac Complications
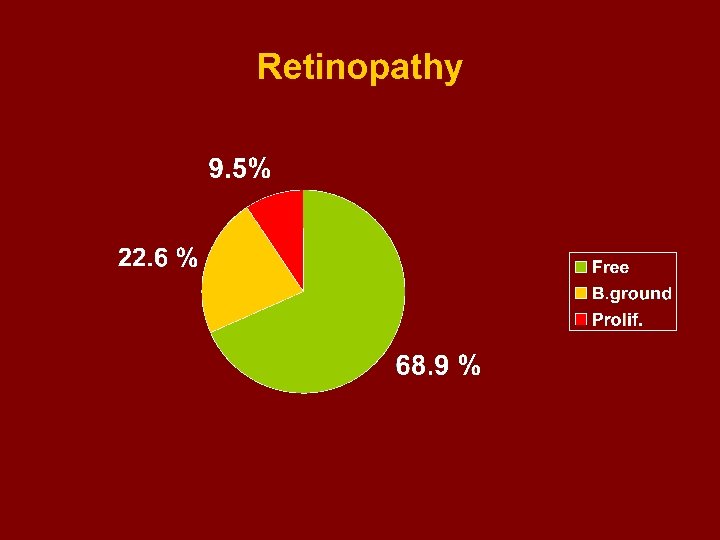
 - Free - Back ground - Proliferative 68. 9")
Retinopathy (in 1173 patients ) - Free - Back ground - Proliferative 68. 9 % 22. 6 % 9. 5 %

Retinopathy in correlation with Duration of DM

l

Frequency of Foot Complications

Prevalence of foot complications 1 - Fungus infection 2 - Foot ulcers 3 - Evident Ischaemic changes 4 - Amputations 5 - Deformities = 22. 0 % = 6. 8 % = 9. 7 % = 3. 0 % = 1. 0 %
 - Occurrence of DKA episodes in = 12. 2 %.")
Diabetes Keto Acidosis (DKA) - Occurrence of DKA episodes in = 12. 2 %. ---------------------------------- The mean age in patients who developed DKA = 42. 5 years - The mean age in patients who never developed = 53. 1 years

Hypoglycemia - Occurrence of Hypoglycemic episodes in = 20. 5% ------------------------------------ The mean age of patients who developed hypoglycemic episodes at any time = 50. 8 years The mean age of patients who did not experience hypoglyceamic episodes = 52. 1 years

Fertility and Abortions : 21. 5% Fertility : 3. 6 ch/m

The Socio economic Burden

Middle East Countries- economic status per capitum incomes : High Kuwait Emirates Qatar Bahrain Oman Saudi Arabia Libya >5, 000 US $ Middle (Iraq) Iran Low Syria Jordan Tunisia Morocco Egypt Yemen Sudan < 2, 000 US $
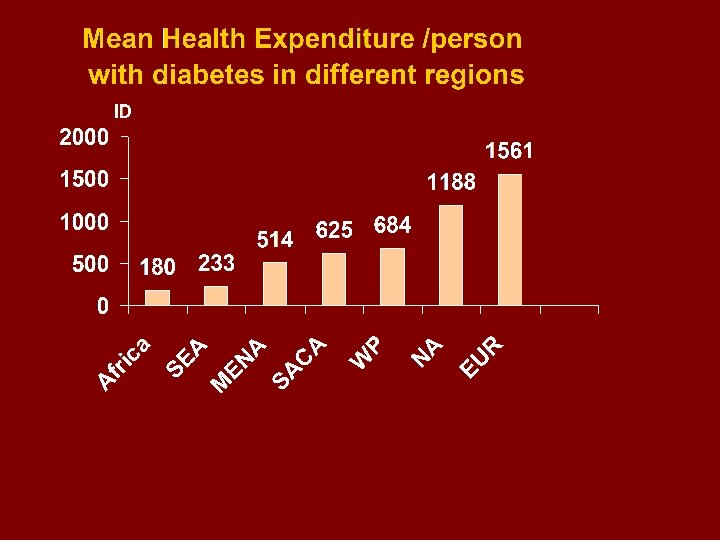

MENA Countries according to The Mean Health Expenditure person with diabetes in ID (international Dollar) : Diabetes Atlas, 3 rd Ed. > 200 Afghanistan 56 Iraq 72 Pakistan 99 Sudan 103 Yemen 110 Syria 185 200 -600 Alger Morocco Egypt Libya 273 285 286 384 600 - 1000 > 1000 Oman 614 Bahrain 1047 Tunisia 637 Lebanon 1050 Jordan 711 Qatar 1198 Iran 744 Kuwait 806 Saudi Arabia 891 Emirates 929
")
Hospital Treatment 2001 Cost /Day (Egyptian Study )

Distribution of Hospital Cost 55% Medicine & Supp. 45% Basic ( Food : 5% H. C. Team 11% Others: 29%)
 8. 85% EGYPT")
Year Cost / percapit. Burden for Human Insulin (40 u /d) 8. 85% EGYPT 1. 9% QATAR 3. 1% SAUDI ARABIA

Cost Burden of Oral Treatment related to Percapitum 4. 2% 29. 9% EGYPT QATAR 8. 4% SAUDI ARABIA

What are The IDF Goals ? 1. Global Advocacy 2. To raise Global Awareness omote appropriate Diabetes Care & Prevention 4. Encourage finding a Cure



For improving Diabetes Care and Prevention , Education of Health Care Providers should consider expertise in both: I- Clinical Diabetes , II- Educations skills and




The Way to a National Diabetes Program
 2 - Primary")
Minimal requirements : 1 - Insulin and medications availability ( affordable) 2 - Primary centers for diagnosis and care 3 - wide distribution of services allover the country 4 - Basic requirements to manage complications 5 - Education : knowledge & skills to patients – Public orientation 6 - National basic studies in epidemiology and socioeconomics. 7 - Care for Diabetes in School children 8 - Care for diabetes in pregnancy

Potential Adverse Factors 1 - Economic : Poor Financial Res. /per capit. / Government expenditure/ House-hold expend. with High Prev. of diab. 2 - Demographic Extensive areas with poor communications. High population density 3 - Social : Illiteracy- Misconceptions – adverse habits and traditions.

WHO IDF National Institute Government Parliament NGO Ministry of Health Medical Group Family Patient Work- school Friends Pharmaceutical industries Society MEDIA Syndicate Physician Nurse Dietitian Foot Care Pharmacist Laboratory

In Developing a National Diabetes Programme : 1 - Consider the specific needs in the country and available resources to decide priorities 2 - Define the role to be played by each one of the constituents of the community , and Identify Champions for projects. 3 - Seek partnerships with : WHO , Twining , WDF , Rotary , etc. .
 1 - Increase Investments")
Obligations of Different Parties The Government ( Ministry of Health) 1 - Increase Investments in Health/Diabetes 2 - provide Minimal Diabetes Care in Clinics & Hospitals 3 - Insure Insulin & Medications Availability 4 - provide Education : Patient, Health Care Team and Public 5 - Coordinate with Health Care Syndicates 6 - Coordinate with NGOs 7 - attract International Aid programmes 8 - promote National Research ( epidemiol. -socioeconomic)
 1 - Budget planning to improve diabetes Care 2 - Taxation Exemption")
Parliament (Legislation) 1 - Budget planning to improve diabetes Care 2 - Taxation Exemption for insulin & medical requirements 3 - Put rules and regulations for NGO activities 4 - Maintain and guard Patients’ Human Rights ( anti discrimination, working , children, women , elderly …etc) 5 - Health Insurance Laws
 1 - Advocacy 2 - Education Programs for :")
The Non-Governmental Organizations (NGOs ) 1 - Advocacy 2 - Education Programs for : -Patients and Families -Health Care Team -Community at large 3 - Rules & Regulations - legally recognized - non profitable - accountable and transparent - coordinated & complementary to government - no unhealthy competition, extravagance , business controlled ( by industries )

The Health Care Team The Physician 1 - is Leader of the HC team 2 - is the Final reference for his patient’s education 3 - keep harmony with others in the HC team 4 - requires continuous training courses and updates 5 - acquire education skills Nurses 1 - Training courses , by whom ? 2 - Knowledge + skills & attitude 3 - skills in education 4 - keep Team work 5 - Continuous education , scientific meetings and workshops

Diabetes Care for Special Groups School Children - Registration at national level - Individual records in schools - basic equipments to manage emergencies - Education courses to school attendants. - protecting special rights : play- recreation treatment. non discrimination …etc

Mothers with Diabetes of Pregnancy - Screening for diabetes of pregnancy - Protocols for management of GD - Care for the N. B. - After-labour follow-up of mothers

The National Diabetes Registry - essential as source of information for planning public services - Central location - paper or computer recordings - contains individual patient data - complemented by local & peripheral registries (in schools - work – Health insurance, etc ) - network connections for exchange information

Diabetes Screening Programmes - Specifically to high risk groups - By central planning and organization - ensure unified criteria for diagnosis - Screening for early detection of complications : - Sending study groups to remote areas.

International Relations The International Diabetes Federation 1 - get moral support from IDF to National Associations & programs 2 - use as source of information & educational material 3 - Benefit from IDF Task forces’ activities and programs 4 - Benefit from WDD events

The WHO 1 - Government / collaborative programmes for promotion of diabetes Care 2 - NGO : collaboration in promoting diabetes care through training & education programmes

The Patient Obligations 1 - Take active role: seek to be educated 2 - follow proper life style 3 - comply 4 - not to accept misconceptions and deceptive propaganda

Thank You Bibliotheca Alexandrina on WDD
783a00912ef99b594850df5333a06591.ppt