5b1b85f67420fb46505b2fed3abbe2d9.ppt
- Количество слайдов: 29



Devices use for Neonatal AKI Timothy E. Bunchman Professor and Director Pediatric Nephrology & Transplantation Children’s Hospital of Richmond Virginia Commonwealth Univ. School of Medicine Timothy. bunchman@vcuhealth. org pedscrrt@gmail. com www. pcrrt. com

Disclosure n Safety committee for new device for Baxter

Overview n n n What are options for neonatal RRT Is there data that one RRT modality is superior in certain situations In the US is there anything approved?
 HD (standard and")
Mode of Dialysis n n n PD (standard and continuous flow) HD (standard and High Flux) CRRT n n CVVH CHHD CVVHDF SLED
 or Cuffed Equipment-manual or automated Solutions-lactate or")
PD-standard n n n Access-acute (non cuffed) or Cuffed Equipment-manual or automated Solutions-lactate or bicarbonate based from Industry Heater-online Anticoagulation-intraperitoneal with no systemic effect

PD-Equipment

PD-Access Cuffed PD Access Acute PD Access n n Cook Critical Care acute PD access Chest Tubes Feeding Tubes Angiocaths

Pediatric Data-Continuous PD n Raaijmakers et al Clin J Am Soc Nephrol 6: 311– 318, 2011. Compared to Std PD increase in Net UF and Net Solute clearance with less intraabdominal elevated pressure

Ca. Cl infusion line/or TPN/or Med line Venous line “arterial” line
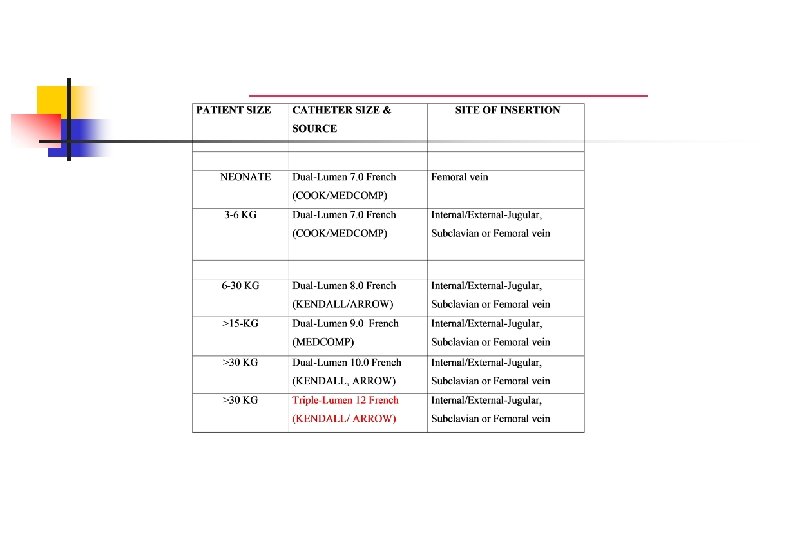

HD-Std or High Flux n n n Access-as above Equipment-multiple machines Solutions-online production Heater-online Anticoagulation-heparin or none

Hemo Dialysis Machine Evolution Fresenius 2008 h: Travenol RSP: Cobe C 3: Drake-Willock: Cobe Centry: 1980 s 1960 s 2000 s 1960 s 1990 s-2000 s Seratron: 1979

CRRT n n n Access-as above Equipment-multiple machines Solutions-industry produced bicarbonate based with or without calcium Heater-online Anticoagulation-heparin, citrate, prostacyclin (www. pcrrt. com)

CRRT Machines: Modern Generation

Factors effecting hemodynamics-4 n Circuit reaction n n Circuit compliance Circuit extracorporeal volume n n more or a problem in pediatrics Membrane reaction n Bradykinin release syndrome

Membranes Compatibility n Complement activated reaction to blood/hemodialysis membrane interaction that causes n n n leukopenia thrombocytopenia increased Alveolar-Arterial gradient to to pulmonary sequestration resulting in hypoxia

Membranes Compatibility n n Use of more biocompatible membranes (eg AN-69 polyacrylonitrile marketed as the M 60 or M 100) results in less complement activation Hemodialysis data has shown that biocompatible membranes (eg AN 69 membrane) improve survival in ARF, have a shorter time to recovery of renal function, and is less associated with oliguria

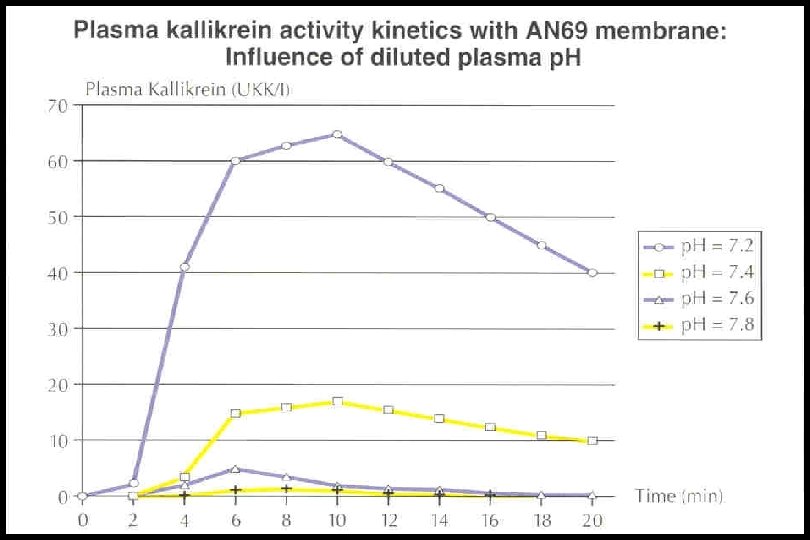
Membranes Compatibility n n n AN-69 membranes have been associated with “Bradykinin Release Syndrome” in patients on ACE inhibitors This “Bradykinin Release Syndrome” may be p. H dependent But what about it use in CRRT?
 n What")
Bradykinin Release Syndrome (Brophy et al, AM J Kid Dis, June 2001) n What is the link n Blood bank blood has n n ICa of 0. 04 mmol/l K+ of 40 -60 m. Eq/l p. H of 6. 4 Therefore we hypothesize that if this is a p. H blood reaction either we buffer the blood or bypass the membrane
: 1328 -33)")
Negating the Bradykinin Factor (Hackbarth et al Pediatr Nephrol. 2005 Sep; 20(9): 1328 -33)
 Dialysate flow (ml/h)")
Prismaflex Device with HF 20 Set n n n Blood flow(ml/min) Dialysate flow (ml/h) Subst-flow rate (ml/h) Subst. prebp (ml/h) Volume reduction(ml/h) Heparin-Infusion (ml/h) 10 -100 50 -2500 20 -1000 30 -1000 10 -2000 0. 5 -5. 0 • treatmentoptions • SCUF • CVVHDF Not available • CVVHDF pre+postdil in the US



SLED n n Access-Same as CRRT and HD Equipment-Fresenius system n n n Same lines as use in HD Same membrane as used in HD Can be diffusive and or convective Solutions-On line production Heater-on line Anticoagulation-heparin or citrate

Which modality is the best?

so n n Vascular access and machinery make extracorporeal therapies difficult in these small children As CRRT machines become miniaturized advancement in vascular access will be needed.
 Continuous Flow PD BFR")
RRT Modalities Modality CRRT SLED HD (standard PD or HF) Continuous Flow PD BFR 3 -5 mls/kg/min access dependent 10 -20 mls/kg/pass 10 -20 mls/kg/hr Dialysis Flow Rate 0 -4 liters/hr 6 liters /hr 30 -50 liters/hr 0. 5 -2 liters/hr Convective Flow Rate 0 -4 liters/hr 0 0 Systemic Anticoagulation Heparin or citrate Heparin or none Thermic control Yes yes partial Ultrafiltration control Yes yes partial Solutions Industry made On Line production Industry made Drug clearance Continuous Intermittent Continuous Nutritional clearance Continuous Intermittent Continuous

Conclusion n n Over 2 decades of advancement we are still struggling with issues of neonatal AKI and RRT Do what you do well and use that modality for no controlled studies to date (or in the future) will demonstrate outcome based upon RRT modality
5b1b85f67420fb46505b2fed3abbe2d9.ppt