72924d991613d7c8b90389b5d69d8671.ppt
- Количество слайдов: 51



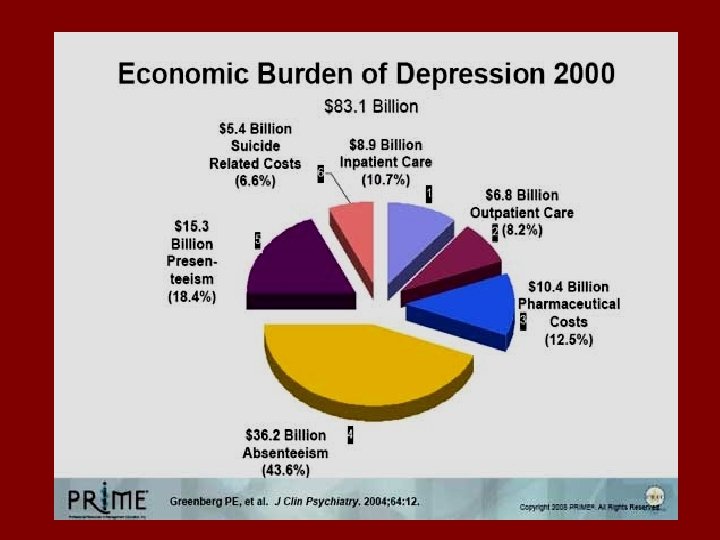
• Depression is 4 th most disabling medical condition worldwide • Predicted to be 2 nd only to chronic heart disease with regards to disability by year 2020 • The management of TRD is a major public health problem worldwide • Need to consider multiple forms of depression: Unipolar Bipolar Dysthymia With Chronic Pain

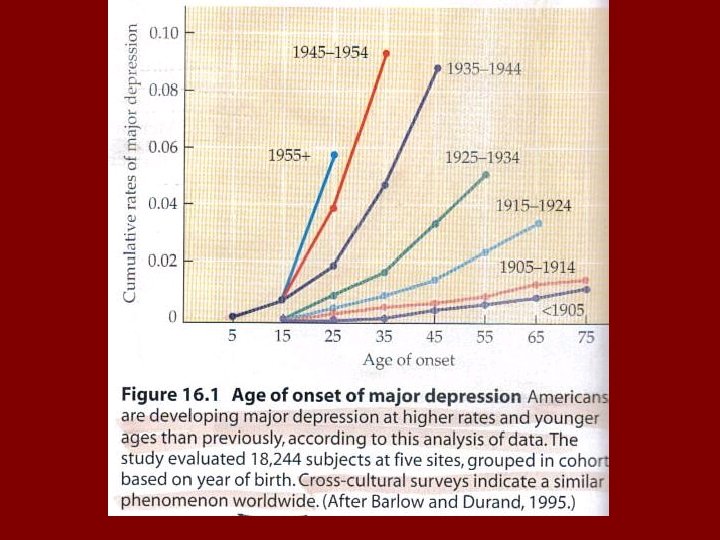
• Common, typically recurrent, often chronic disabling disorder • Life-long prevalence of 4. 9 -17. 9% • Women twice as likely to have depression • More frequent in patients with a general medical condition • Episodic disorder, one episode every 5 years • 20 -35% experience a chronic unremitting course • Early-onset dysthymia is also common and has milder but also chronic depressive symptoms • Relapse and recurrence more common in those with a history of dysthymia and in those with partial recovery • Longer episodes appear more difficult to treat

Life-time and 12 -Month Prevalence of Major Depression in Israel Lifetime 12 -month Gender differences Age group N Total % Wom % Men % Lifetime p 12 -month p 21 -34 1627 10. 6 13. 3 8. 0 6. 3 7. 8 4. 8 . 001 . 015 35 -49 1302 9. 4 12. 4 6. 3 5. 7 7. 6 3. 7 . 000 . 002 50 -64 1069 6. 3 10. 1 6. 2 6. 1 6. 3 . 634 . 876 >65 861 10. 0 11. 6 8. 0 6. 0 7. 5 4. 0 . 09 . 050 All 4859 10. 2 12. 3 7. 9 6. 1 7. 3 4. 7 . 000 Levav and Levinson. The Epidemiology of Affective Disorders in Israel 2009

Age-standardized Suicide Rates per 100. 000 Population Years Men Women Total 2000 14. 2 3. 7 8. 7 2001 14. 6 2. 9 8. 5 2002 12. 8 3. 5 8. 0 2003 14. 7 2. 8 8. 5 2004 13. 5 3. 4 8. 3 Bursztein and Apter The Epidemiology of Suicidal Behavior in The Israeli Population, 2009

Causes of Disability in the United States, Canada, and Western Europe in 2000 Iglehart, J. K. N Engl J Med 2004; 350: 507 -514

Druss el al, Molecular Psychiatry, 2009

Druss el al, Molecular Psychiatry, 2009

Druss el al, Molecular Psychiatry, 2009

Prognosis of Affective Illness The Burden of The Illness

“Paradigmatic Shift” Unipolar Major Depressive Disorders are viewed as chronic illnesses with episodic recurrences as the norm Brodati et al 2001

Typical Symptoms of Affective Disorders Mania Excessive energy Restless Depression Worthlessness Loss of interest/pleasure Aggression Rapid thoughts and speech Sadness Insomnia Significant weight gain/loss Hypersomnia Euphoria Restlessness/ agitation Grandiosity Fatigue Guilt Irritability Recklessness Decreased libido Poor concentration Suicidal tendencies
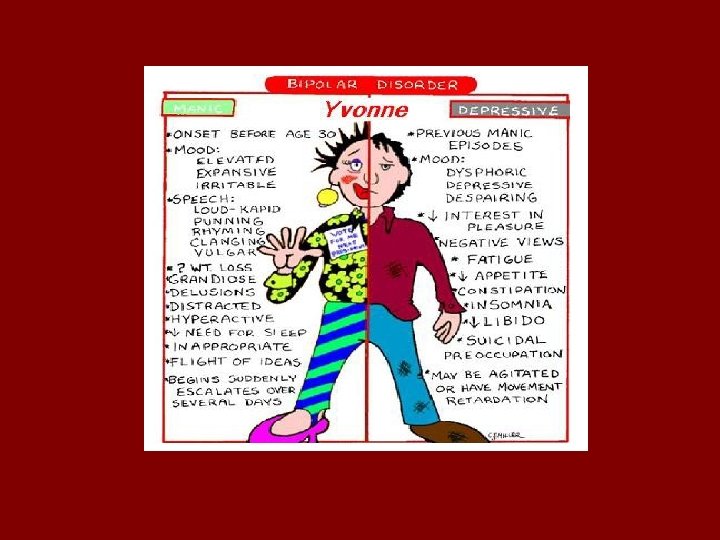

The Bipolar Illness Mania Wide range of syndromes with manic features, associated with episodes of depression Hypomania Normal Depression Severe depression Normal Cyclothymic mood personality disorder variation Bipolar II disorder Unipolar mania Bipolar I disorder Not shown: recurrent unipolar depression with family history of mania/hypomania Goodwin FK, Jamison KR. Manic-depressive illness. New York: Oxford University Press, 1990

The Unipolar Illness Major Depression. Recurrent Episode Major Depression with Residual Symptoms Double Depression Dysthymic Disorder

Long Term Studies of Depressive Disorders Demonstrate Repeat episodes in over 75% of patients Stephens &Mc. Hugh 1991; Picinelly & Wilkinson 1999; O’Leary & Lee 1996; Mueller et al 1999 Readmission of 35 -62% Lee &Murray 1988; Smith & North 1988; Stephens & Mc. Hugh 1991; Thornicroft &Sartorius, 1993 Chronicity or Persistance of 5 -25% Winokur & Morrison 1973; Angst 1988, 1997, 1993; Thornicroft &Sartorius, 1993 Judd 1997; Judd et al 1998 10 -year G. A. F. in moderate to severe scores in > 25% Surtees & Barkley 1994 Fair to poor occupational status in 30% of patients Winokur & Tsuang 1979

Time Spent in Specific Bipolar Disorder Affective Symptoms 1% 2% 6% 9% 53% 32% % of Weeks Asymptomatic Depressed Manic/hypomanic Cycling/mixed 146 bipolar I patients followed 12. 8 years 50% 46%* 86 bipolar II patients followed 13. 4 years *%s do not add to 100 due to rounding Judd LL et al. Arch Gen Psychiatry. 2002; 59: 530 -537. Judd LL et al. Arch Gen Psychiatry. 2003; 60: 261 -269.

Prognosis of Affective Disorders • • • Paradigmatic shift Complex life-long disorders Often misdiagnosed and as a consequence poorly treated Current treatment is a combination of “science and art” Proven treatment algorrhytms and RTC’s are sorely needed Comorbidity with psychiatric and medical conditions common

Comorbidities… The Rule, Not the Exception: The Multidimensionality of Depressive and Bipolar Disorder Pain disorders Diabetes mellitus Cardiovascular Obesity Migraine Personality disorders Mood Disorder Substance abuse Eating disorders ADHD Impulse control Anxiety disorders Mc. Intyre RS, et al. Hum Psychopharmacol. 2004; 19(6): 369386. Osteoporosis

Long-Term Antidepressants for Depressive Disorder and Risk for Diabetes Mellitus Andersohn et al. Am J Psychiatry. 2009; 166: 591 -8


The evolution of antidepressants 1950 s 1960 s 1970 s 1980 s Phenelzine Imipramine Maprotiline Fluoxetine Isocarboxazid Clomipramine Amoxapine Sertraline Tranylcypromine Nortriptyline Mianserin 1990 s Bupropion Mirtazapine Paroxetine Venlafaxine Amitriptyline Fluvoxamine. Duloxetine Desipramine Citalopram Milnacipran Reboxetine Moclobemide Escitalopram 2000 s Agomelatine

Outcome of Depression treatment - Citalopram Complete absence of symptoms (HDRS < 7 Reduction of 50% in HDRS or QIDS- Remission or QIDS-SR < 5) Recovery Relapse Recurrence SR Response x x Symptoms Syndrome Treatment Phases QIDS-SR: Quick Inventory of Depressive Symptomatology, Self-Report x Acute 6 -12 Weeks Continuation 4 -9 Months STAR*D citalopram trial N=2, 876 Maintenance ? 1 Year Remission rate at 8 weeks was 27. 5%-32. 9 Response rate at 8 weeks was 47% Trivedi MH et al. , Am J Psychiatry 163: 28 -40, 2006

“Targeting multiple components of pathobiology through a single drug molecule is gaining increasing acceptance in the treatment of complex disorders in the CNS (like MDD)” Van Der Schyf and Youdim 2009

• Triple inhibitors of monoamine reuptake • Agents blocking both 5 -HT reuptake and inhibitory 5 -HT autoreceptors. Bimodal antidepressants acting as 5 -HT 2 C or 5 HT 2 A receptor antagonists • Novel antidepressants with antagonist properties at 5 -HT 3 receptors • Dual 2 -AR autoreceptor antagonists/monoamine reuptake inhibitors • Hybrid, monoaminergic/nonmonoaminergic antidepressants – Histamine H 3, nicotinic, and GABAB receptors as targets: improving cognitive function – Glutamatergic receptors as targets: ionotropic and metabotropic hypotheses – Neuropeptidergic receptors as targets: focus on Neurokinin 1 (NK 1) receptor antagonists/SRI • Innovative neuroendocrine mechanisms: calming HPA axis overdrive and recruiting melatonin receptors • Drugs affecting intracellular cascades, BDNF, and more

Recommendation 1: The American College of Physicians recommends that when clinicians choose pharmacologic therapy to treat patients with acute major depression, they select second-generation antidepressants on the basis of adverse effect profiles, cost, and patient preferences Recommendation 2: The American College of Physicians recommends that clinicians assess patient status, therapeutic response, and adverse effects of antidepressant therapy on a regular basis beginning within 1 to 2 weeks of initiation of therapy Recommendation 3: The American College of Physicians recommend that clinicians modify treatment if the patient does not have an adequate response to pharmacotherapy within 6 to 8 weeks of the initiation of therapy for major depressive disorder Recommendation 4: The American College of Physicians recommends that clinicians continue treatment for 4 to 9 months after a satisfactory response in patients with a first episode of major depressive disorder. For patients who have had 2 or more episodes of depression, an even longer duration of therapy may be beneficial

“The available evidence does not support clinically significant differences in efficacy, effectiveness, or quality of life among SSRIs, SNRIs, SSNRIs, or other second generation antidepressants for the treatment of acutephase MDD”

Imipramine treated groups

Therapeutic Neuromodulation: A Welcomed Change in Psychiatry

21 st Century Neuromodulation Therapies in Psychiatry treatment may be at similar threshold as cardiology 25 years ago, in terms of potential for devices to improve our therapeutics Effective medications & psychosocial interventions help many but by no means all of our patients Devices have potential to help our severely ill patients and clearly warrant intensive research going forwards

Definitions Neurotherapeutics Treatments for nervous systems disorders through pharmacological or other modalities Neuromodulation-Neurostimulation The therapeutic alteration of activity in the central, peripheral or autonomic nervous systems, electrically or pharmacologically*, by means of implanted devices. *(today we must add also magnetically, and through light or ultrasound waves)

Neuronetics Positioning System


Paus 2002

A Seizure May Not Be Always. . … Necessary TMS VNS DBS

Lobotomy Goodman and Insel: The scientific and clinical community must assure the public that the kind of mistakes made before are not repeated
 • Transcranial Magnetic Stimulation (TMS) • Magnetic Seizure")
Therapeutic Neuromodulation • Electroconvulsive Therapy (ECT) • Transcranial Magnetic Stimulation (TMS) • Magnetic Seizure Therapy (MST) • Vagus Nerve Stimulation (VNS) • Deep Brain Stimulation (DBS) • Neurofeedback • Low Intensity Low Frequency Ultrasound (Lilfu) • Optogenetics

Variations in electrical treatments • ECT: – Brief pulse ECT – Ultrabrief pulse ECT – Localized seizure ECT • Transcranial direct current stimulation (t. DCS) • Transcranial alternating current stimulation (t. ACS)

Role of ECT in 21 st century ECT remains a gold standard treatment for severe depression and has yet to be superseded by medication or by any other brain stimulation treatment In recent multicenter trials remission rates with ECT are about 75%. This is 3 -4 fold superior to antidepressants Relapse and recurrence rates unreasonably high
 Changes in shape and direction")
Variations of TMS • • Theta burst stimulation (TBS) Changes in shape and direction of magnetic pulse Quadripulse stimulation Paired associative stimulation Magnetic seizure therapy Controllable pulse and shape TMS devices Deep TMS

72924d991613d7c8b90389b5d69d8671.ppt