

Death_of_Genius_Imangali_Maira.pptx
- Количество слайдов: 25
 Department of Pathological Anatomy IWS death of the Genius Prepared by: Imangali Maira The faculty of General medicine Group: __14 -24 -2___ Checked by Head of the department: Sapargaliyeva A. D.
Department of Pathological Anatomy IWS death of the Genius Prepared by: Imangali Maira The faculty of General medicine Group: __14 -24 -2___ Checked by Head of the department: Sapargaliyeva A. D.
 plan Introduction Development of a stroke Potential causes Morphological manifestations Morphological changes in carotid and vertebral arteries Willis circle First 24 hours Stroke was peculiar? Morphological patterns of the stroke in elderly patients References
plan Introduction Development of a stroke Potential causes Morphological manifestations Morphological changes in carotid and vertebral arteries Willis circle First 24 hours Stroke was peculiar? Morphological patterns of the stroke in elderly patients References
 Introduction Patient Name: Leonardo di ser Piero da Vinci Age: 67 years Cause of death: Stroke
Introduction Patient Name: Leonardo di ser Piero da Vinci Age: 67 years Cause of death: Stroke
 Development of stroke Incident stroke in Leonardo has also been associated with: depression negative feelings stressors, like life events age gender (male sex)
Development of stroke Incident stroke in Leonardo has also been associated with: depression negative feelings stressors, like life events age gender (male sex)
 Potential causes Atherosclerosis Hypertension
Potential causes Atherosclerosis Hypertension
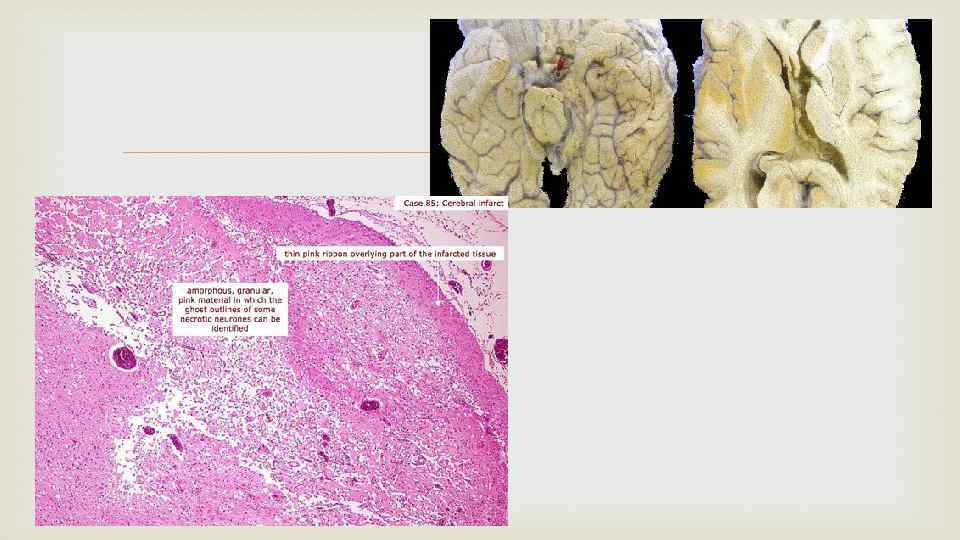
 MORPHOLOGICAL MANIFESTATIONS In ischemic stroke infarcts are formed, i. e. foci of necrosis of the brain caused by insufficient blood flow. In the early stages of ischemic stroke revealed a morphologically region blanching and swelling of the brain substance, a fuzzy structure of the perifocal zone. Microscopic examination can detect symptoms of cerebral oedema, and necrotic changes in the nerve cells. The neurons are swollen, poorly stained cells dramatically changed. At a later date in the area of infarction revealed a softening of the grey, crumbling mass
MORPHOLOGICAL MANIFESTATIONS In ischemic stroke infarcts are formed, i. e. foci of necrosis of the brain caused by insufficient blood flow. In the early stages of ischemic stroke revealed a morphologically region blanching and swelling of the brain substance, a fuzzy structure of the perifocal zone. Microscopic examination can detect symptoms of cerebral oedema, and necrotic changes in the nerve cells. The neurons are swollen, poorly stained cells dramatically changed. At a later date in the area of infarction revealed a softening of the grey, crumbling mass
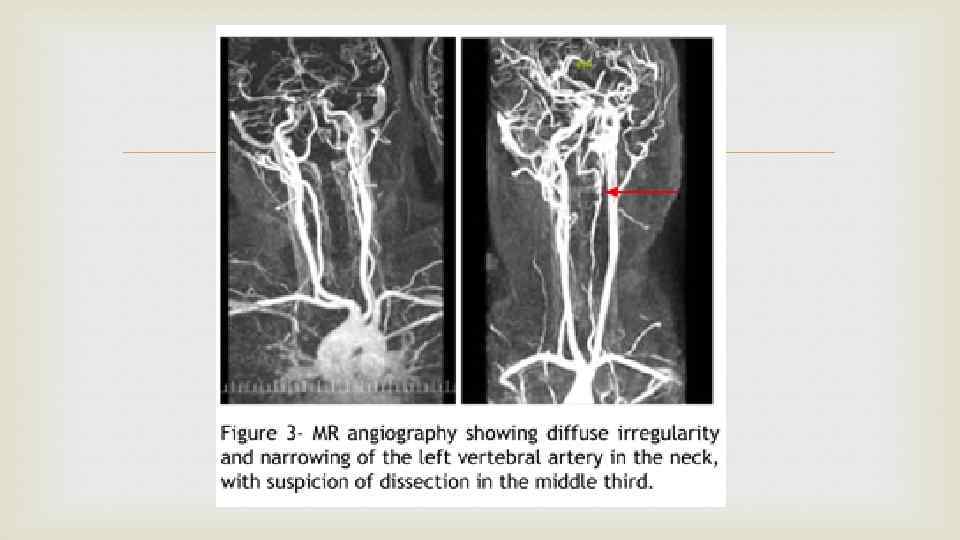
 Morphological changes in carotid and vertebral arteries blood The brain derives its supply of arterial from the carotid arteries (front of the neck) and vertebral arteries (back of the neck) and the branches of these arteries. Any significant narrowing of these arteries and/or total blockage by a clot will deprive the brain of blood. When blood supply is cut off, the brain tissue is deprived of oxygen (hypoxia) and this leads to tissue injury known as ischemia.
Morphological changes in carotid and vertebral arteries blood The brain derives its supply of arterial from the carotid arteries (front of the neck) and vertebral arteries (back of the neck) and the branches of these arteries. Any significant narrowing of these arteries and/or total blockage by a clot will deprive the brain of blood. When blood supply is cut off, the brain tissue is deprived of oxygen (hypoxia) and this leads to tissue injury known as ischemia.
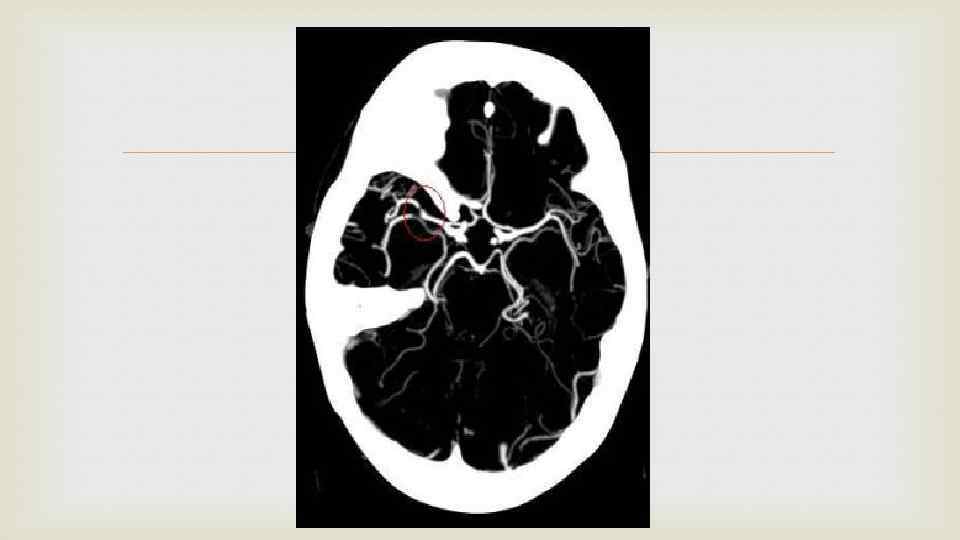
 Willis circle At the base of the brain, these arteries form a circular network known as the circle of Willis, which ensures that the brain is constantly fed with oxygen and nutrient-rich blood. There is a narrowing of the vessel due to the atherosclerotic plaques.
Willis circle At the base of the brain, these arteries form a circular network known as the circle of Willis, which ensures that the brain is constantly fed with oxygen and nutrient-rich blood. There is a narrowing of the vessel due to the atherosclerotic plaques.

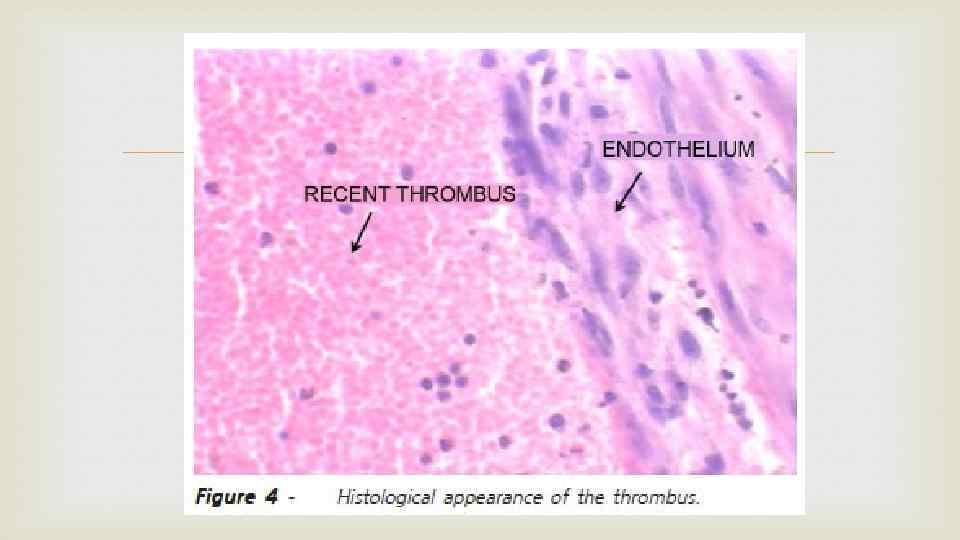
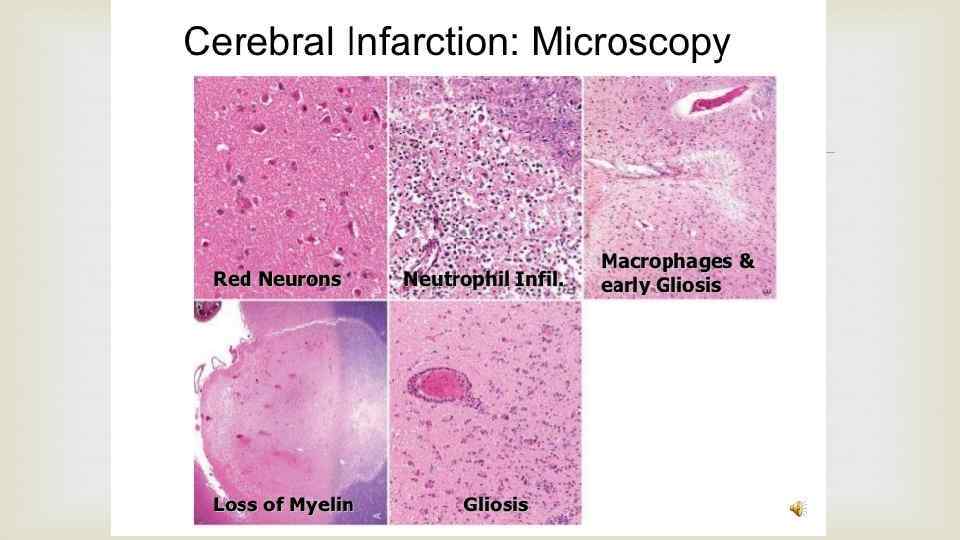
 Cytotoxic and vasogenic edema There is") First 24 hours Ischemic neuronal change (red neurons) Cytotoxic and vasogenic edema There is loss og the usual tinctorial characteristics of white and gray matter strustures Endothelial and glial cells, mainly astrocytes, swell Myelinated fibers begin to disintegrate
First 24 hours Ischemic neuronal change (red neurons) Cytotoxic and vasogenic edema There is loss og the usual tinctorial characteristics of white and gray matter strustures Endothelial and glial cells, mainly astrocytes, swell Myelinated fibers begin to disintegrate
 Dynamyics of changes After the first 12 hours, ischemic neuronal and cytotoxic and vasogenic edema predominate. Endothelial and glial cells, mainly astrocytes, swell, and myelinated fibers begin to disintegrate. Up to 48 hours, there is some neutrophilic emigration, which is followed by mononuclear phagocytic cells during the ensuing 2 to 3 weeks. After several months, the striking astrocytic nuclear and cytoplasmic enlargement regresses. In the wall of the cavity, astrocyte processes form a dense feltwork of glial fibers admixed with new capillaries and a few perivascular connective tissue fibers.
Dynamyics of changes After the first 12 hours, ischemic neuronal and cytotoxic and vasogenic edema predominate. Endothelial and glial cells, mainly astrocytes, swell, and myelinated fibers begin to disintegrate. Up to 48 hours, there is some neutrophilic emigration, which is followed by mononuclear phagocytic cells during the ensuing 2 to 3 weeks. After several months, the striking astrocytic nuclear and cytoplasmic enlargement regresses. In the wall of the cavity, astrocyte processes form a dense feltwork of glial fibers admixed with new capillaries and a few perivascular connective tissue fibers.
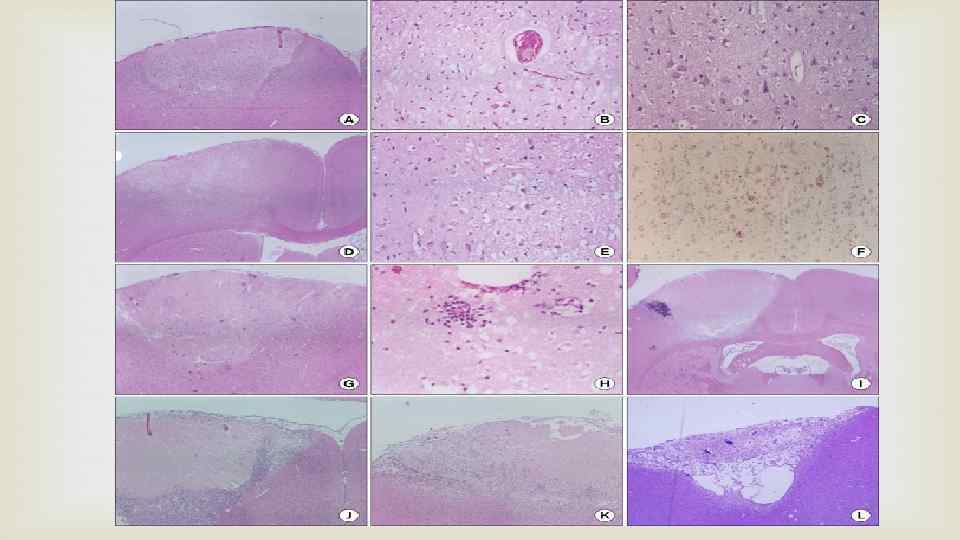
 Half an hour after stroke, wedge shaped edematous lesion consisted of pallor and vacuolation of neuropils at low magnification, high-magnification view revealed dark neurons (A-C). Between 6 -12 hours, eosinophilic neurons appeared, which showed swelling of cytoplasm (D, E). The swollen cytoplasm of eosinophilic neurons was positive for NF immunostainning (F). After one day, neutrophil infiltration was shown at the edges of the infarct, and continued to 2 days (G, H). Between 3 -7 days, the infarct lesion was characterized by central necrosis surrounded by macrophages and newly formed capillaries (I, J). At 2 -4 weeks, cortical necrosis was completely resolved and the lesion was replaced by gliosis and fibrosis (K, L).
Half an hour after stroke, wedge shaped edematous lesion consisted of pallor and vacuolation of neuropils at low magnification, high-magnification view revealed dark neurons (A-C). Between 6 -12 hours, eosinophilic neurons appeared, which showed swelling of cytoplasm (D, E). The swollen cytoplasm of eosinophilic neurons was positive for NF immunostainning (F). After one day, neutrophil infiltration was shown at the edges of the infarct, and continued to 2 days (G, H). Between 3 -7 days, the infarct lesion was characterized by central necrosis surrounded by macrophages and newly formed capillaries (I, J). At 2 -4 weeks, cortical necrosis was completely resolved and the lesion was replaced by gliosis and fibrosis (K, L).
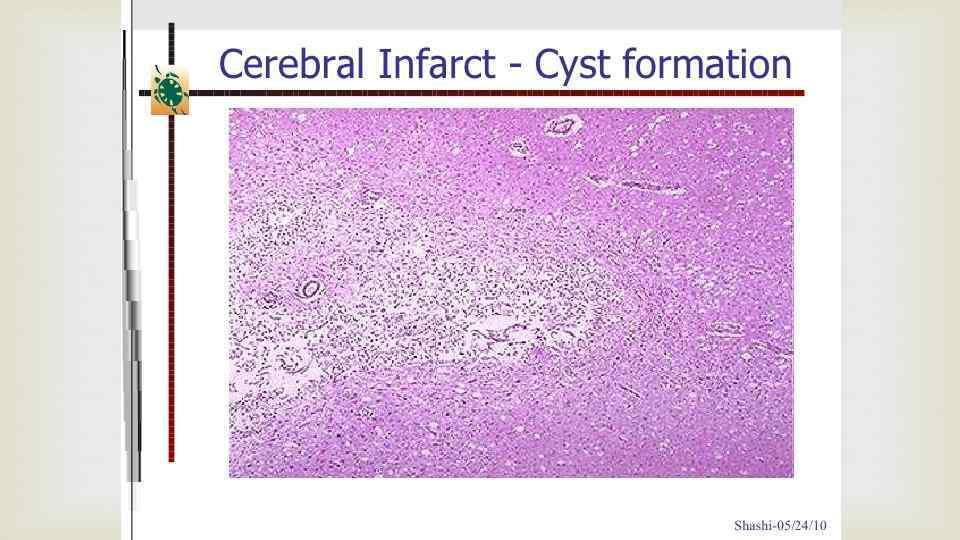
 STAGES OF STROKE Stage 1 - the acute phase of stroke up to 21 days. Fresh necrosis is formed in 3 - 5 days, this acute phase of stroke, there is shrinkage of the cytoplasm and karyoplasm develops perifocal edema. Stage 2 - early recovery period of up to 6 months. Pannecrose happens all the cellular elements, and astroglial proliferation of small vessels. Possible regression of neurological deficit. Developed collateral circulation Stage 3 - late recovery period of 6 to 12 months, develop glial scarring or cystic defects of the brain tissue. Stage 4 - after 1 year - residual effects of a stroke
STAGES OF STROKE Stage 1 - the acute phase of stroke up to 21 days. Fresh necrosis is formed in 3 - 5 days, this acute phase of stroke, there is shrinkage of the cytoplasm and karyoplasm develops perifocal edema. Stage 2 - early recovery period of up to 6 months. Pannecrose happens all the cellular elements, and astroglial proliferation of small vessels. Possible regression of neurological deficit. Developed collateral circulation Stage 3 - late recovery period of 6 to 12 months, develop glial scarring or cystic defects of the brain tissue. Stage 4 - after 1 year - residual effects of a stroke
 Stroke was peculiar? Leonardo da Vinci has a moderate ishemic stroke of middle cerebral artery so he lived for 2 years, with the right hemiparesis upper extremity. Ischemic stroke on the grounds stenosing atherosclerosis of cerebral arteries leads to degeneration and atrophy of the cerebral cortex, to the development of atherosclerotic dementia, but Leonardo remained in good health of his mind.
Stroke was peculiar? Leonardo da Vinci has a moderate ishemic stroke of middle cerebral artery so he lived for 2 years, with the right hemiparesis upper extremity. Ischemic stroke on the grounds stenosing atherosclerosis of cerebral arteries leads to degeneration and atrophy of the cerebral cortex, to the development of atherosclerotic dementia, but Leonardo remained in good health of his mind.
 Morphological patterns of the stroke in elderly patients With age there is loss of volume and weight of the brain mainly through the cortex and the hippocampus. During aging the brain is not only neuronal atrophy, there also degenerative changes in the white matter of the brain, and astrocytic hyperactivity microglobulin. Reduced cerebral perfusion of more than 50% decreases the functional activity of neurons and over 80% in acute cerebral ischemia leads to electrolyte imbalance and neuronal death. With age this increases the permeability of the bloodbrain barrier, allowing plasma proteins to enter the blood in the perivascular space and cause glial and neuronal damage. Age-related changes in the brain reduce cerebrovascular reserves and increase its sensitivity to ischemia.
Morphological patterns of the stroke in elderly patients With age there is loss of volume and weight of the brain mainly through the cortex and the hippocampus. During aging the brain is not only neuronal atrophy, there also degenerative changes in the white matter of the brain, and astrocytic hyperactivity microglobulin. Reduced cerebral perfusion of more than 50% decreases the functional activity of neurons and over 80% in acute cerebral ischemia leads to electrolyte imbalance and neuronal death. With age this increases the permeability of the bloodbrain barrier, allowing plasma proteins to enter the blood in the perivascular space and cause glial and neuronal damage. Age-related changes in the brain reduce cerebrovascular reserves and increase its sensitivity to ischemia.
 hippocampal sclerosis neuronphagia
hippocampal sclerosis neuronphagia
 References http: //www. preventaf-strokecrisis. org/report/chapter 2 http: //www. foods-healing-power. com/causes-of-stroke. html http: //www. merckmanuals. com/professional/neurologic-disorders/stroke(cva)/ischemic-stroke http: //www. neuroanatomy. ca/stroke_model/mca_info. html http: //www. healthhype. com/stroke-cva-ischemic-hemorrhagic-types-andmini-strokes. html#pretty. Photo Bard G, Hirschberg GG: Recovery of voluntary motion in upper extremity following hemiplegia. Arch Phys Med Rehabil 1965; 46: 567 -572. Sunderland A, Tinson D, Bradley L, Hewer R: Arm function after stroke: An evaluation of grip strength as a measure of recovery and a prognostic indicator. J Neurol, Neurosurg, and Psych 1989; 52: 1267 -1272
References http: //www. preventaf-strokecrisis. org/report/chapter 2 http: //www. foods-healing-power. com/causes-of-stroke. html http: //www. merckmanuals. com/professional/neurologic-disorders/stroke(cva)/ischemic-stroke http: //www. neuroanatomy. ca/stroke_model/mca_info. html http: //www. healthhype. com/stroke-cva-ischemic-hemorrhagic-types-andmini-strokes. html#pretty. Photo Bard G, Hirschberg GG: Recovery of voluntary motion in upper extremity following hemiplegia. Arch Phys Med Rehabil 1965; 46: 567 -572. Sunderland A, Tinson D, Bradley L, Hewer R: Arm function after stroke: An evaluation of grip strength as a measure of recovery and a prognostic indicator. J Neurol, Neurosurg, and Psych 1989; 52: 1267 -1272
 THANK YOU FOR ATTENTION!
THANK YOU FOR ATTENTION!