7dce2fcb6fc3f7395d83fcaef1ab5647.ppt
- Количество слайдов: 31



Department of Obstetrics and Gynecology Residency Program “A-FIT” Report “A-FIT”: Areas For Improvemen. T January 2016

Monthly A-FIT Report • Monthly Updates » Duty Hour “Time-out” » Evaluations / Feedback: • Rotational and my. TIPreport » Continuity Clinic Check-In • Areas for Improvement (A-FIT) report » Updates • Milestone of the Month • Faculty and Resident Development » Topic of the Month

Duty Hour “Time Out”!! AY 2015 -16 Block Number Duty Hour Standard / # Violations 80 hr work week 1 day off in 7 1 and 2 1 2 3 24/28 hr rule 1 10 hrs between shifts In-House Call 1 1 1 2 1 4 3 and 4 1 2 5 2 1 1 4 11 3 2 6 1 5 and 6 5 7 1 8 1 1 1 7 and 8 1 4 3 Total possible number of violations: In 4 week block: 3136 In 7 week block: 5487 Violation Rate: In 4 week block: In 7 week block: 0. 12% 0. 15%

Faculty/Fellow Wednesday Conference Attendance Average Conference Attendance YTD: Actual Body Number! 14 12 10 8 6 4 2 0 FP REI ONC MFM MIGS Faculty Conference Attendance YTD Average: Percentage 80. 00% 60. 00% 40. 00% 20. 00% FP REI ONC MFM Faculty MIGS URO Fellows WPH OTHER Total

Rotation Evaluations: Completed w/i 2 weeks 87. 5% Completion 88% Completion for the last block latest completed block ACGME Requirement

Rotation Evaluations: Completed w/i 2 weeks 3 1/2 - 4 Weeks Rotations 120. 00% 80% Completion for latest completed block 100. 00% ACGME Requirement 80. 00% 60. 00% 40. 00% 20. 00% Overall ACC FP (odd blocks) Block 4 Block 5 GYN (even blocks) Block 6 Block 7 OB - 1 st Years OB - 3 rd Years

Resident Feedback

Resident Feedback

Continuity Clinic Follow-up 1. Educational Sessions 2. Milestone Worksheet Completion Month Total Possible Sessions Completed Sessions Percentage Completed Milestone Feedback Completed January 32 17 53% 17 December -- -- -- 9 November -- -- -- * October 36 22 61% * September 34 24 71% * August 34 19 56% *

Areas for Improvement: 2015 ACGME Survey and Internal Survey • • • QI Training Value of Conferences: » Grand Rounds » M and M Satisfaction with feedback Education not compromised by… » Service » Other trainees Provided data about practice habits Fatigue » Instructed how to manage fatigue » Provided a way to transition care when fatigued

Area #1: QI Training Low = 1, High = 5 1 2 Not bad (34% neutral or low 3 Quality Improvement training and 2 4 10 value responses) but room for involvement (4. 26%) (8. 51%) (21. 28%) improvement… 4 5 18 (38. 30%) 13 (27. 66%) Brimmage QI Project: -First four modules of the QI training released -Participation is open to faculty and fellows -Class QI projects in development -Operationalize -Review results: -Present results: Jan – March, 2016 April, 2016 May, 2016

Area #2: Value of Conferences

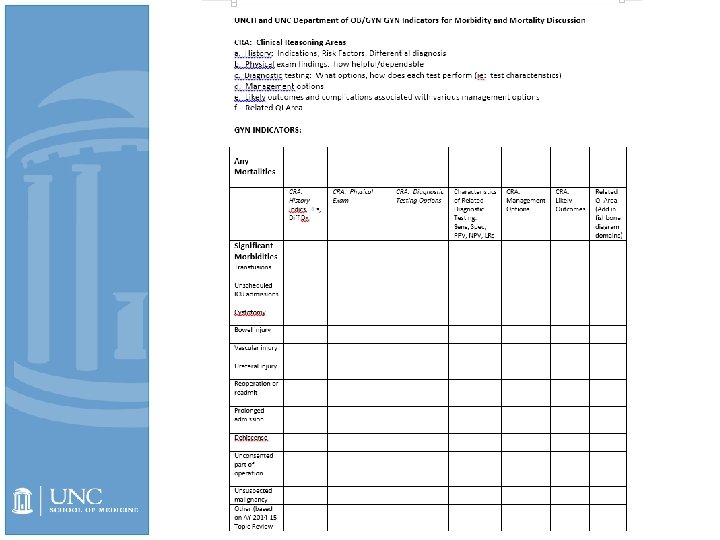
Area #2: Value of Conferences Low = 1, High = 5 1 2 3 4 5 Grand Rounds 3 4 10 (4. 55%) (6. 06%) (15. 15%) Not bad (25 -30% neutral or low 29 (43. 94%) 20 (30. 30%) Morbidity and Mortality value responses) but room for 2 7 12 (2. 99%) improvement… (10. 45%) (17. 91%) 26 (38. 81%) 20 (29. 85%) M&M Conference Focus: Clinical Reasoning Areas Grand Rounds: Proposed: Invited speakers ID’ing how talk content is particularly relevant to Specialist Practice M and M Programming Changes Underway Proposed Improvement Plan: --Programmatic focus on clinical reasoning --4 cases per conference --Active “management” of questions/answer session: ----Discussants ----Presenting Chiefs

Rotation Huddle Items Rotation Service over education Education compromised by other trainees Improve satisfaction with feedback Ares for fatigue teaching and awareness Transition care when fatigue is identified Benign -organizing resident OR schedule (not new problem). Hard time knowing when attendings are available to operate (esp for WPH). Lots of emails back and forth to settle on OR date consider having resident block time – -complicated laparoscopies— keep working on ways to get PGY 2 involved, what steps he/she is going to do -maybe have a surgical curriculum, checklist (like the medical students have— 8 cuffs sewn, 5 ureters dissected out, 3 ligation of uterine at its origin, 3 skeletonizing IP, etc) -Mytipreport is about as good as it gets in terms of ease and simplicity, but we still all find it hard to make sure we stay up on it. -wish they didn’t have vacation as chief during this rotation (lots piles up while he/she is out and it’s a little overwhelming to take care of upon return—>source of fatigue) -not really applicable Wednesdays afternoons: it’s challenging to put the pieces together of what happened during resident didactics. Fellows and attendings need to be diligent about updating GYN team with post- didactic sign-out. -keep the PGY 2 as the primary conduit to sign out to UNC-CH team and hospitalists at HBH Attendings need to respond to mytipreport requests from residents

Rotation Huddle Items Rotation Service over education Education compromised by other trainees Improve satisfaction with feedback Ares for fatigue teaching and awareness Transition care when fatigue is identified REI No issues No problems in clinic setting. In the OR, having multiple levels of trainees including Fellow, 4 th year and 2 nd year can detract from the experience and opportunities of individual trainees. Solution: Depending on the case, consider sending the 4 th year to cover a different Gyn service OR if there is need for coverage and have the fellow and 2 nd year in the REI OR Related to the above suggestion, defining which cases or parts of cases are appropriate for certain levels of training would help with this. Setting expectations prior to the case starting would make it clear what your role should be at the specific level of training. If specific roles are assigned in the OR (as above) then it would be easy to provide feedback on that specific task or portion of the case Consider having a mid rotation checkpoint to receive feedback Consider having "resident patients" (maybe as a part of fellows clinic or a half day of clinic precepted by an attending) so that we could get full history, suggest work up and formulate a plan for a few patients and then have specific feedback on clinical knowledge - This may be difficult logistically but if possible would be great for putting what we learn into practice. No issues

Rotation Huddle Items Rotation OB Service over education 1. Cleaning up patients after delivery, particularly cesarean delivery, but also SVDs. -Currently residents feel they are “expected” to clean patient up after delivery when they have other more pressing clinical responsibilities. Action item: Dr. Strauss scheduled to speak at upcoming nursing meeting on Monday, November 23 rd. Dr. Strauss also to meet with scrub techs. Will propose the below guideline to be shared with both nursing/scrub techs and resident groups: “OB providers should help RN and/or scrub tech clean patient after delivery, unless urgently needed elsewhere; in which case will explain to RN/scrub tech they are unable to help clean the patient because of other immediate responsibilities. ” Metric: Frequency residents clean patient when other immediate responsibilities are present. 2. New anesthesia rotation on L&D. This year, two anesthesia residents have elected to do an OB rotation. Current guidelines exist regarding the role of this anesthesia resident, however they do not offer specific guidelines regarding the type of patients the anesthesia resident can follow, thus leading to some stress placed on the OB chief when they need to supervise that anesthesia resident if/when caring for any “high risk” patients. Action item: Dr. Strauss to meet with current OB chief (Dr. Jarvis) and review anesthesia resident guidelines Follow up: Drs. Strauss and Jarvis met on 10 -15 -15 and updated the guidelines as follows: Anesthesia “ resident on OB would share/split running the board with OB intern but only care for “low risk” patients, as determined by an upper year resident. ” Metric: OB chief feedback in March 2016, when next anesthesia resident scheduled to rotate on L&D

Rotation Huddle Items Rotation Education compromised by other trainees OB 3. Missed opportunities to participate in more advanced OB procedures (ie, rescue cerclage, forceps, breech extraction) because of MFM fellow participation Action item: Dr. Strauss to meet with MFM fellows and discuss at next fellows meeting on Monday, November 30 th. In addition, the following statement has been added to the fellows Rotation “ Guidelines”: “MFM fellow has first right of refusal over chief resident in performing more advanced procedures (ie, rescue cerclage, forceps, breech extraction), however, the fellow is expected to inform the chief resident of the procedure and allow the resident the opportunity to assist/participate/observe the procedure. ” Metric: OB chief resident feedback regarding opportunities to participate in more advanced OB procedures.

Rotation Huddle Items Rotation Improve satisfaction with feedback Ares for fatigue teaching and awareness OB Encourage both faculty and residents to take advantage of the smart phone App available for My. TIPReport. Chief resident or OB Attending could ask OB team members each day at lunchtime if any concerns over fatigue. In addition, the Antepartum Attending could ask team members during antepartum rounds if any concerns over fatigue. Transition care when fatigue is identified When fatigue identified, OB chief could determine which resident available to cover the resident experiencing fatigue, so that individual could go home at lunchtime.

Rotation Huddle Items Rotation Service over education Education compromised by other trainees Wake. Med Rachel/Sharon: Seeing all consults who are stable but need 48 hour quants in clinic Assisting private attendings on cesareans at night Covering triage when midlevels are out Covering an entire clinic schedule when midlevels are out. Esper: I believe since we have a large volume of patients service can supercede education. I think that we try to balance it out during the week by having providers in triage and also in clinic. In addition, we have a provider that helps with rounding in the AM (Mac Pannill), Perhaps when we split antepartum rounding with the MFMs then walk rounds can occur so there is one-onone teaching. Not an issue Rachel No fellows - gives us more exposure to patients and cases. Enough deliveries that EM and FM interns don't compromise number Esper: We do have off service residents however now that an intern takes vacation on the rotation, it decreases the number of bodies on the floor. This does not play a role in surgical exposure, which is important but can reflect the number of deliveries and repair. I believe our volume is great that everyone should feel proficient with low risk deliveries and repairs by the end of the rotation. Sharon I don’t think our training is compromised by the presence of other trainees (EM/FM residents). There’s plenty of volume for everyone.

Rotation Huddle Items Rotation Improve satisfaction with feedback Ares for fatigue teaching and awareness Wake. Med Not an issue Rachel Not sure that we need to do anything else here Esper We do not address this however, we do have a buddy car pool in place. In addition, residents are encouraged to sleep at the hospital if overly fatigued. We have a night float system for the interns. We can try to institute that for the upper level residents however in years past, the residents did not like the idea of night float. Sharon: Rachel: Already doing a good job of giving inperson mid-rotation and post-rotation feedback. Attendings are doing a good job of My. Tip reports after cases Esper: We are all trying to participate in My. Tip report. In addition, we make time for one on one feedback mid- rotation and at the termination of the rotation. Sharon: Attendings are all very good at completing My. Tips after cases, and everyone meets with Dr. Esper in person at least twice to receive inperson feedback during the rotation. The carpool is great, but it usually tends to work in the upperlevels favor because they don’t have to drive home after being on a 24+ hr call. However, upper-levels often elect to stay postcall to write notes and/or do procedures, and the intern has to stay late in the morning to drive the upper-level home. I know of interns who have left as late as 12 -1 pm (even though signout is at 8: 15 AM) when they have to come back in at 8 pm for a night call. When this happens repeatedly, it contributes to fatigue and should be discouraged, either by having the oncoming team round on antes/gyns instead of the off-going resident, or by having upperlevels drive themselves if they intend on staying post-call to operate.

Rotation Huddle Items Rotation Transition care when fatigue is identified Wake. Med Rachel: Could we ever consider doing a night float for upper levels? Could we ever consider having 2 day interns/ 2 night interns rather than 3/1? Could we ever have the oncoming team round on the antes/gyns, so that the off-going resident doesn't have to stay post-rounds to finish notes? Sharon: The EM/FM residents have a lot of restrictions on their work schedules secondary to didactics and clinic hours, leaving the OB residents to cover many more night shifts and calls. If we sacrifice our didactic time on Wednesdays and our clinic hours in order to fully commit ourselves to our patients at Wake, I think the EM and FM residents should be held to the same standard.

Rotation Huddle Items Rotation Service over education Education compromis ed by other trainees Improve satisfaction with feedback Ares for fatigue teaching and awareness Transition care when fatigue is identified Onc 3 possible areas of improvement could be: (1)coordination with our nurse clinicians to keep a better list of patients who are to be admitted for chemotherapy (2)much time spent working on prior authorization for discharge medications (3)much time spent coordinating appointments for patients with their outside cardiologists, PCPs etc. The AIs are very helpful with #2 and #3, but we don’t always have AIs on our service. Our nurse clinicians may be able to help with #2. Not a prob w/ Fellows. Increase the use of my tip report, especially in areas outside of surgical feedback (this would be particularly nice for the interns who are not typically in the OR). I thought that I could come up with a list of the topics in my tip report that would be applicable during this rotation to send out to the fellows and attendings – this may encourage increase use. Signout happening later than 5: 30 pm: -work to signout at prescribed time to ensure duty hour compliance and address fatigue Some of the stress/fatigue from being the intern on gyn onc is related to continuity clinic – prepping clinic Monday night and doing notes on Tuesday night, after a long day on the floor. We thought that on Tuesdays (usually a lighter day in the OR), maybe the intern could get a extra hour before coming back to the floor to work on notes. We do think that 3 AIs on service can be difficult, Could work to keep this to 2 AIs at a time, if possible.

Rotation Huddle Items Rotation Service over education Education compromised by other trainees Improve satisfaction with feedback Ares for fatigue teaching and awareness Transition care when fatigue is identified Urogyn N/A N/A N/A
 Provided")
Area #5: Provided data about practice habits “Yes” (UNC ‘ 14 -’ 15) Provided data about practice habits Proposed Improvement Plan: “Yes” (UNC ‘ 14 -’ 15) “Yes” (National) 50% 68% -Rotation Directors to discuss -May have a LOT to do with “labeling” work regarding Practice Based Learning and Improvement

Area #6: Mitigating effects of fatigue and excessive stress “Yes” (UNC ‘ 14 -’ 15) “Yes” (National) Instructed on how to manage fatigue 79% 82% 92% Provided a way to transition care when fatigued 64% 61% 80% “Resiliency corner”: Feature of new monthly Residency Program Update (The next issue will be arriving in your inbox this week, keep an eye out!) Proposed Improvement Plan: Reinstitute twice yearly programming with Dr. Meltzer-Brody “Departmental engagement” work in AY 15 -16

Professional Development Opportunities… • Get to know our Milestones! • Professional Development Topic-of-the-Month

Professional Development Opportunities… • Get to know our Milestones! » Care of Patients in the Intrapartum Period • Professional Development Topic-of-the-Month » Identifying and addressing fatigue and impairment

Milestone of the Month Care of Patients in the Intrapartum Period: • Demonstrates basic knowledge of routine/uncomplicated intrapartum obstetrical care including, conduct of normal labor • Provides intrapartum obstetrical care for women with uncomplicated pregnancies (e. g. , identification of fetal lie, interpretation of fetal heart rate monitoring, and tocodynamometry) • Differentiates between normal and abnormal labor • Recognizes intrapartum complications (e. g. , chorioamnionitis, shoulder dystocia) • Manages abnormal labor • Manages intrapartum complications (e. g. , cord prolapse, placental abruption) • Provides care for women with complex intrapartum complications and conditions • Identifies indications for consultation, referral, and/or transfer of care for patients with intrapartum complications • Effectively supervises and educates lower-level residents in intrapartum care • Collaborates and provides consultation to other members of the health care team in intrapartum care • Applies innovative approaches to complex and atypical intrapartum conditions and implements treatment plans based on emerging evidence

Identifying and addressing fatigue and impairment If you have were not able to attend the January 27 th Grand Rounds with Dr. Meltzer-Brody, here is the link to her presentation: http: //www. med. unc. edu/obgyn/events/grand-rounds 21? utm_source=meetings&utm_medium=email&utm_campaign=4

Department of Obstetrics and Gynecology Residency Program “a-FIT” Report “a-FIT”: areas For Improvemen. T Thank you for all you do!
7dce2fcb6fc3f7395d83fcaef1ab5647.ppt