

30df98c1663a28ef5caa2a2e26520c63.ppt
- Количество слайдов: 28
 Dementia in Clinical Practice • Mary Ann Forciea MD • Clinical Prof of Medicine • Division of Geriatric Medicine • UPHS • Photo: Nat Geographic
Dementia in Clinical Practice • Mary Ann Forciea MD • Clinical Prof of Medicine • Division of Geriatric Medicine • UPHS • Photo: Nat Geographic
 Who has dementia? • 78 yr old retired librarian • Lives alone, children visit on holidays • Family concerned about ‘clutter’ in house, hygiene, unpaid bills • 68 yr old child care worker • Lives with her husband, drives, in charge of ‘house money’ • “Forgot” a child in classroom at end of day
Who has dementia? • 78 yr old retired librarian • Lives alone, children visit on holidays • Family concerned about ‘clutter’ in house, hygiene, unpaid bills • 68 yr old child care worker • Lives with her husband, drives, in charge of ‘house money’ • “Forgot” a child in classroom at end of day
 ? • 84 yr old urology inpatient • 70 yr") Who has dementia (2) ? • 84 yr old urology inpatient • 70 yr old homebound patient – Post op day 1: hostile – Bedbound, mute – Family caregivers – Oral intake decreasing • Attempts to strike nurse with cane • Refusing blood draw • Pulled out catheter
Who has dementia (2) ? • 84 yr old urology inpatient • 70 yr old homebound patient – Post op day 1: hostile – Bedbound, mute – Family caregivers – Oral intake decreasing • Attempts to strike nurse with cane • Refusing blood draw • Pulled out catheter
 Terms • Dementia – Chronic, progressive – Impairment in >1 “domain of cognition” • Memory, language use, executive function(judgment), attention, coordination • Mild cognitive impairment – Impairment in 1 “domain of cognition” – ? “pre-dementia” • Delirium – Short term
Terms • Dementia – Chronic, progressive – Impairment in >1 “domain of cognition” • Memory, language use, executive function(judgment), attention, coordination • Mild cognitive impairment – Impairment in 1 “domain of cognition” – ? “pre-dementia” • Delirium – Short term
 How do we know about Brain Function? • Cell structure – Microscope (biopsy, cell culture) – CT, MRI, PET scans • Brain regions – imaging • “Domains” of cognition – Imaging – Psychological testing
How do we know about Brain Function? • Cell structure – Microscope (biopsy, cell culture) – CT, MRI, PET scans • Brain regions – imaging • “Domains” of cognition – Imaging – Psychological testing
 Cell structure: Neurons • Networks • Grey matter/white matter
Cell structure: Neurons • Networks • Grey matter/white matter
 Brain regions • Regions have different activities
Brain regions • Regions have different activities
 Domains of cognition • • • Memory Calculation Language Orientation Spatial construction Executive function (judgment)
Domains of cognition • • • Memory Calculation Language Orientation Spatial construction Executive function (judgment)
 Mapping Memories Natl Geographic
Mapping Memories Natl Geographic
 What is wrong in dementia? Theories Neurons: waste products, shape of cells, signaling, genetic flaws Regions: biochemistry, structure Domains: communication We don’t yet know.
What is wrong in dementia? Theories Neurons: waste products, shape of cells, signaling, genetic flaws Regions: biochemistry, structure Domains: communication We don’t yet know.
 Clinical observations • All patients with dementias are not alike. – Age of onset – Family history – Initial symptom – Most troublesome symptom – Rate of progression – Response to treatment • Is dementia a symptom, not a disease?
Clinical observations • All patients with dementias are not alike. – Age of onset – Family history – Initial symptom – Most troublesome symptom – Rate of progression – Response to treatment • Is dementia a symptom, not a disease?
 – 15% •") Dementia Subtypes • Alzheimer’s Disease • Fronto-temporal dementia (formerly Pick’s Disease) – 15% • Corticobasilar dementias • Dementia with Lewy Bodies – 20% – Distinguished from Parkinson’s Disease with dementia • Vascular disease
Dementia Subtypes • Alzheimer’s Disease • Fronto-temporal dementia (formerly Pick’s Disease) – 15% • Corticobasilar dementias • Dementia with Lewy Bodies – 20% – Distinguished from Parkinson’s Disease with dementia • Vascular disease
 Alzheimer’s type dementia • Gradual onset • Global impairment in cognition – Usually memory impairment predominant • Increased risk in siblings – Apo e allele risk • Slow progression (5 -7 years) – Predictable course (global deterioration scores)
Alzheimer’s type dementia • Gradual onset • Global impairment in cognition – Usually memory impairment predominant • Increased risk in siblings – Apo e allele risk • Slow progression (5 -7 years) – Predictable course (global deterioration scores)
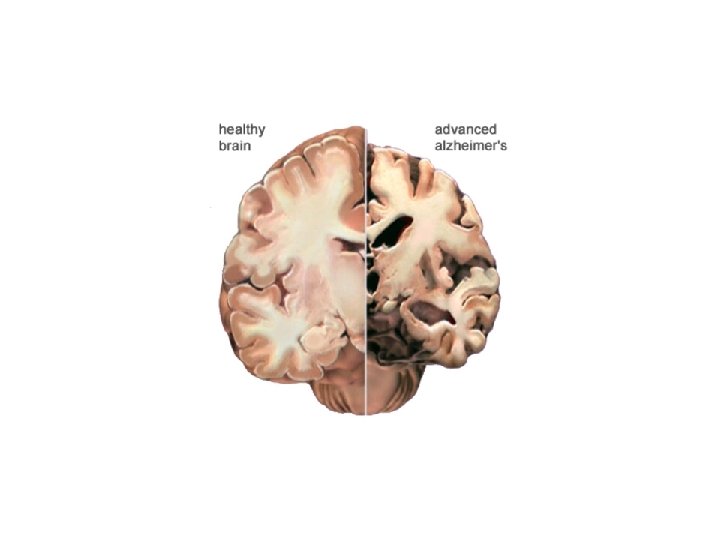
 AD - pathology • Imaging • Neuropathology – quantity and location – Senile plaques • White matter • Amyloid core – Neurofibrillary tangles • Tau protein abnormalities – Initial concentrations highest in hippocampus and temporal lobes
AD - pathology • Imaging • Neuropathology – quantity and location – Senile plaques • White matter • Amyloid core – Neurofibrillary tangles • Tau protein abnormalities – Initial concentrations highest in hippocampus and temporal lobes
 Plaques
Plaques
 Tangle
Tangle
 What clinical problems do patients with Alzheimer’s Dementia Encounter? • Diagnosis • Symptom Management • End of life care
What clinical problems do patients with Alzheimer’s Dementia Encounter? • Diagnosis • Symptom Management • End of life care
 Case 1 NC • 64 yr old retired OR nurse • Referred for evaluation of impaired memory – Birthdates, telephone numbers – Impaired job performance for 1 -2 yrs prior – Inability to ‘balance checkbook’ • Gradual decline over 5 years • Died of pneumonia
Case 1 NC • 64 yr old retired OR nurse • Referred for evaluation of impaired memory – Birthdates, telephone numbers – Impaired job performance for 1 -2 yrs prior – Inability to ‘balance checkbook’ • Gradual decline over 5 years • Died of pneumonia
 Diagnosis • • Largely on history Exclude other conditions Role for biomarkers in near future Staging – Mental status testing (MMSE, MOCA, Mini. Cog) – Functional status staging (FAST, GDR)
Diagnosis • • Largely on history Exclude other conditions Role for biomarkers in near future Staging – Mental status testing (MMSE, MOCA, Mini. Cog) – Functional status staging (FAST, GDR)
 Biomarkers for Alzheimer’s Dementia • Apo lipo protein E subtypes – Apo E-2, E-3, E-4 • 2 copies of E 4 increases risk in some populations • Spinal fluid ‘tau’ protein levels • PET scans for amyloid – People with unexplained MCI – Patients with an unusual course – Early onset dementia
Biomarkers for Alzheimer’s Dementia • Apo lipo protein E subtypes – Apo E-2, E-3, E-4 • 2 copies of E 4 increases risk in some populations • Spinal fluid ‘tau’ protein levels • PET scans for amyloid – People with unexplained MCI – Patients with an unusual course – Early onset dementia
 Concerns about PET scans • How specific is an abnormal test? • May not be useful for staging – (how advanced is the disease) • Will abnormal scans result in ‘overdiagnosis’ employment or insurance implications?
Concerns about PET scans • How specific is an abnormal test? • May not be useful for staging – (how advanced is the disease) • Will abnormal scans result in ‘overdiagnosis’ employment or insurance implications?
 FAST • • The FAST scale has seven stages: 1 which is normal adult 2 which is normal older adult 3 which is early dementia 4 which is mild dementia 5 which is moderate dementia 6 which is moderately severe dementia 7 which is severe dementia
FAST • • The FAST scale has seven stages: 1 which is normal adult 2 which is normal older adult 3 which is early dementia 4 which is mild dementia 5 which is moderate dementia 6 which is moderately severe dementia 7 which is severe dementia
 7 a. speaking limited to 6 words or fewer in an average day b. Speech ability limited to the use of a single intelligible word in an average day c. Ambulatory ability lost (cannot walk without personal assistance). d. Ability to sit up without assistance lost (e. g. , the individual will fall over if there are no lateral rests [arms] on the chair). e. Loss of the ability to smile.
7 a. speaking limited to 6 words or fewer in an average day b. Speech ability limited to the use of a single intelligible word in an average day c. Ambulatory ability lost (cannot walk without personal assistance). d. Ability to sit up without assistance lost (e. g. , the individual will fall over if there are no lateral rests [arms] on the chair). e. Loss of the ability to smile.
 AD - treatment • Improve all co-existing conditions! • Specific treatments – Cholinesterase inhibitors • Donepazil, rivastigmine – Adrenergic stimulants • Memantine • Treatment of associated symptoms – Agitated behaviors • Non pharmacologic, environmental • drugs
AD - treatment • Improve all co-existing conditions! • Specific treatments – Cholinesterase inhibitors • Donepazil, rivastigmine – Adrenergic stimulants • Memantine • Treatment of associated symptoms – Agitated behaviors • Non pharmacologic, environmental • drugs
 End of life issues • Should be anticipated – Advance Directives, conversations with proxies • Goals of care – Nutrition – Hospitalization – Caregiver burdens – Hospice involvement
End of life issues • Should be anticipated – Advance Directives, conversations with proxies • Goals of care – Nutrition – Hospitalization – Caregiver burdens – Hospice involvement
 Summary • “Dementia” is a symptom complex • We are in the early stages of understanding the pathology, and discovering effective treatment • Optimal care requires advance planning, caregiver involvement, and a team of professionals
Summary • “Dementia” is a symptom complex • We are in the early stages of understanding the pathology, and discovering effective treatment • Optimal care requires advance planning, caregiver involvement, and a team of professionals