Анемия_Ждать_ФАР2014.ppt
- Количество слайдов: 48



Дебаты Острая анемия: ждать не нужно восполнять… ЭМ Николаенко

АНГЕЛЫ или ДЕМОНЫ

Что делает гемоглобин ?

0 лёгочные капилляры альвеолярный газ увлажнённый воздух атмосфера дриях он митох р. О 2 в рт стткани м < 1 м ткани артерия к. Па мм рт ст Кислородный каскад РО 2 150 100 50
 и потребление (VO 2) кислорода Система транспорта О 2 5")
Доставка (DO 2) и потребление (VO 2) кислорода Система транспорта О 2 5
 и потребление (VO 2) кислорода В норме DO 2= 500 -700")
Доставка (DO 2) и потребление (VO 2) кислорода В норме DO 2= 500 -700 мл/м 2 VO 2= 120 -140 мл/м 2 DO 2 = CO x Hb x Кx. SO 2+Pa. O 2 xk DO 2 VO 2 КЭО 2=25% (1/4) Резерв О 2 = 3/4 от DO 2 сердце кровь легкие С(а-в)О 2 х СВ КЭО 2 = VO 2 /DO 2 = Са. О х СВ = С(а-в)О 2 / Са. О 6
 и потребление (VO 2) кислорода IDO 2 = ICO x Hb")
Доставка (DO 2) и потребление (VO 2) кислорода IDO 2 = ICO x Hb x Кx. SO 2+Pa. O 2 xk DO 2 2, 0 х 70 х 1, 34 х 0, 98 +2 = 185 VO 2 =120 КЭ = 65% Резерв 45 Sv. O 2 = 66% Повышение СВ на 0, 5 DO 2 235 Эр. М 0, 5 л (+100 г Нв ) КЭО 2=25% (1/4) Резерв О 2 = 3/4 от DO 2 235 7

доставка О 2 Оптимум доставки О 2 СВ гемоглобин 100 г/л КЁ

Что делает гемоглобин ? Формула НВ +О 2

МЕТОДЫ ПРЕДОТВРАЩЕНИЯ ПЕРИОПЕРАЦИОННОЙ КРОВОПОТЕРИ И ПОСЛЕОПЕРАЦИОННОЙ АНЕМИИ «Сухое операционное поле» - Управляемая артериальная гипотензия - Возвышенное положение зоны операции Гипотермия Периоперационная изоволемическая гемодилюция Сохранение клеток крови (CELLSAVER) Эритропоэтин Методичное, малотравматичное оперирование

1960 -ые годы «правило 10/30» - не брать больного на операционный стол, если Нв < 10 г% и Ht < 30 Valeri CR et al. The red cell transfusion trigger: Has a sin of commission now become a sin of omission? Transfusion 1998; 38: 602 -610 …: «Грех деяния теперь стал грехом упущения? »

«Естественная» гемодилюция, возникающая вследствие хирургической кровопотери, почему-то пугает не так сильно. Предубеждённость анестезиологов и хирургов в отношении ИГД связана с опасениями гипокоагуляции и ишемии (гипоксии)
 ?")
ишемия (гипоксия) ?
 с помощью масс-спектрографа, газоанализатора в наркозном")
• Измерение потребления кислорода (VO 2 ) с помощью масс-спектрографа, газоанализатора в наркозном аппарате или капнографа. РСО 2 РЕЕСО 2 =37 РЕСО 2 = 21, 5 50 0 VD / VT ~ 0, 4 VO 2 = VE F(I – E)О 2 Рi. О 2 =145 РЕО 2 =125 РЕЕО 2 =110 РО 2 100 VO 2 = 173, 2 мл/мин VE – минутная вентиляция лёгких F(I – E)О 2 – разница концентраций О 2 во вдыхаемой и смешанной выдыхаемой газовой смеси
» IVO 2 ml/min/m 2")
«ПОТРЕБЛЕНИЕ КИСЛОРОДА ВО ВРЕМЯ ПЕРИОПЕРАЦИОННОЙ ОСТРОЙ ИЗОВОЛЕМИЧЕСКОЙ ГЕМОДИЛЮЦИИ (ИГД)» IVO 2 ml/min/m 2 ИГД Абсцисса - этапы исследования Ордината - IVO 2 ml/min/m 2 - контрольная группа - группа ИГД У больных под общей анестезией снижение VО 2 при ИГД происходит в такой же степени, как и без ИГД. Не наблюдается существенных различий между группами больных в изменениях метаболизма и питания миокарда во время операции. Полученные данные свидетельствуют о достаточном уровне доставки О 2 при используемой методике ИГД на всех этапах периоперационного периода. Николаенко ЭМ, и соавт. 2002. Nicolayenko E. et al, 2001.

Гематокрит и кислородный бюджет при ИГД До анестезии p < - Ht% - IVO 2 - Pv. O 2 40, 5 ± - КЭO 2 6, 2 0, 05 146, 2 41, 2 ± ± 16, 7 4, 9 p < 0 При ИГД , 05 25, 6 ± 2, 9 29, 1 ± 4, 6 98, 1 ± 12, 2 39, 2 ± 4, 4 23, 7 ± 3, 1 Эксфузия - 12, 7 ± 2, 2 мл/кг (n=57) - 18% от расчетного ОЦК - 70 мл /кг - возмещение 2, 2: 1 (ГЭК 130/0, 4 + Кристаллоиды) снижение КЕ на 28, 1% Снижение Ht на 27% больше расчетного – эффект гемодилюции

При ИГД со снижением Нв до 50 г/л не наблюдается перехода метаболизма на анаэробный путь – снижения потребления кислорода (VO 2 ) и/или развития лактатацидоза. Madjdpour C et al: Anemia and perioperative red blood cell transfusion: A matter of tolerance. Crit Care Med 2006; 34: S 102–S 108

после периоперац. гемотрансфузии 1 п. о. день ИК % Периоперационный е и период шен яции ч Улу ркул ение и ш кроц овы ми ем п ита ч +50 ее, атокр важн гем после ИГД Реинфузия - 50 Плазмозамен 0 Эксфузия % от этапа стабилизации анестезии Периферическое кровообращение при ИГД в периоперационный и ранний п. о. периоды ИК = h f / k

При повышении потребления О 2 миокардом вследствие увеличения нагрузки на сердце гемодилюция до Ht < 29% у больных с атеросклеротическим поражением венечных сосудов может сопровождаться ишемическими эпизодами. Christopherson R et al. Low postoperative hematocrit is associated with cardiac ischemia in high-risk patients. Anesthesiology 1991; 75: A 99 Больные с коронарной недостаточностью хорошо переносят гемодилюцию. Spahn DR et al. Acta Anaesth Scand 1992; 36: 628 Необходим периоперационный мониторинг состояния миокарда !
, оттекающей от различных органов Сa-v. O 2")
Насыщение кислородом венозной крови (Sv. O 2%), оттекающей от различных органов Сa-v. O 2 мл/л кожа, почки – 10; печень – 40; мозг – 60; мышцы – 80; сердце – 110. 37% Для миокарда характерны: наиболее высокий КЭО 2 (> 50%) наиболее низкое Sv. O 2 наиболее низкий резерв О 2 миокард является наиболее чувствительным к снижению доставки кислорода и, соответственно, кислородной ёмкости крови.

838 пациентов в ОИТ. Гемотрансфузия. Гр либеральной стратегии – Нв 90 г/л Гр рестриктивной стратегии – Нв <70 г/л Летальность рестриктивная гр либеральная гр - 22, 2% - 28, 1% (p < 0, 05) ЗАКЛЮЧЕНИЕ рестриктивная стратегия вероятно превосходит либеральную, за исключением пациентов с ОИМ и с коронарной недостаточностью.

Chatteriee S et al. Association of blood transfusion with increased mortality in myocardial infarction: a metaanalysis and diversity-adjusted study sequential analysis. JAMA 2013 Jan 28; 173(2): 132 -9 Среди пациентов с ИМ при трансфузии крови летальность выше, чем без - 18. 2% vs 10. 2% (risk ratio, 2. 91; 95% CI, 2. 46 -3. 44; P <. 001), Повышение риска инфаркта миокарда достоверно связано с трансфузией крови (risk ratio, 2. 04; 95% CI, 1. 06 -3. 93; P =. 03).

Rivers E, et al: Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001, 345: 1368 Рекомендации Rivers E по гемотрансфузии не убедительны Отношение к гемотрансфузии с целью улучшения доставки О 2 противоречиво, поскольку известны неблагоприятные последствия либеральной стратегии. Кислородтранспортная функция консервированных эритроцитов существенно нарушена. Marik PE, Sibbald WJ: Effect of stored-blood transfusion on oxygen delivery in patients with sepsis. JAMA 1993, 269: 3024 -3029
 Переливание крови")
Blood transfusion harmful, even deadly, in some patients with GI bleeds (RCT) Переливание крови вредно и даже смертельно у некоторых пациентов с ЖКК 921 пациент с о. ЖКК (анализ 45 -дн летальности) 1 гр – ограниченная стратегия – Нв < 6, 9 23 человека (5%) умерли 2 гр – либеральная стратегия – Нв > 6, 9 41 человек (9%) умерли При Нв < 6, 9 - снижение относительного риска смерти – 45%, абсолютного – 4% Càndid Vilueva, et al. Transfusion Strategies for Acute Upper Gastrointestinal Bleeding. NEJM 2013; 368^1121.

Трансфузия эритроцитов и исходы у пациентов с ОПЛ, сепсисом и СШ FACTT post-hoc: меньше жидкости – меньше ОРДС; но, трансфузии ? Parsons et al: база данных FACTT - 285 пациентов с СШ. 85 из них “должны были” получать гемотрансфузию по протоколу EGDT (Scv. О 2 Нв, АД, ЦВД), у всех ОПЛ/ОРДС. 35 - трансфузия, 232 - без трансфузии 23 из 35 умерли (43%) 70 из 232 умерли (30%) (р = 0, 06)

повысить DO 2 не вызвать осложнений
 - нозокомиальные инфекции")
Большой мета-анализ 2014 г: либеральная трансфузионная стратегия (Нв > 80 г/л) - нозокомиальные инфекции (ОШ 1, 8) - ОРДС (ОШ 2, 5) - летальность (ОШ 1, 7)

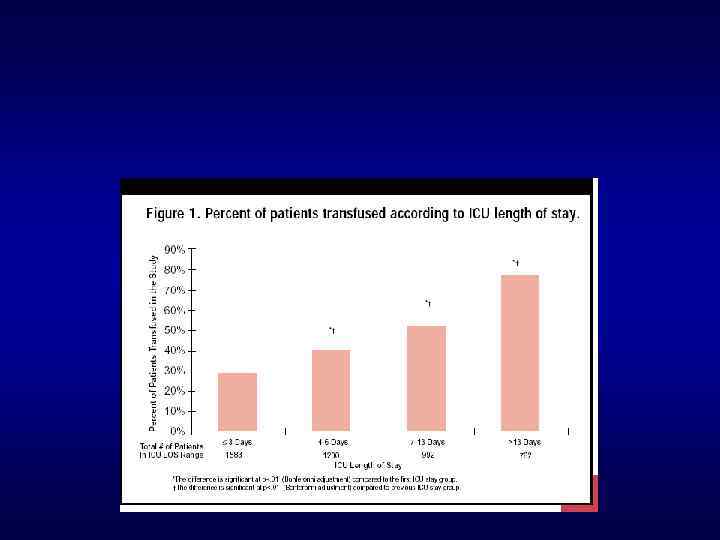
Сроки госпитализации, трансфузии и летальность.

VII. Правила переливания консервированной донорской крови и эритроцитсодержащих компонентов 30. …при острой анемии …снижении уровня гемоглобина ниже 70 - 80 г/л и гематокрита ниже 25% и возникновении циркуляторных нарушений. 32

2014 г: American Association of Blood Banks рекомендует рестриктивную трансфузионную стратегию.
 might become: “Save a Life: Don’t Give Blood. ”")
The new motto (for physicians) might become: “Save a Life: Don’t Give Blood. ” «Сохрани жизнь: не переливай кровь!»


ЗАКЛЮЧЕНИЕ


гипокоагуляция кровоточивость кровопотеря гемотрансфузия

Anemia and Transfusions in the Critically Ill: The Crit Study Congress Review: 31 st Critical Care Congress of the Society of Critical Care Medicine Released May 2002 A prospective, multicenter, observational cohort study of 4, 892 patients from 284 intensive care units (ICUs) at 213 United States hospitals documented anemia in all patients and transfusions in slightly more than 40%. A total of 19% of participating hospitals had documented institutional transfusion protocols or triggers, with the most common trigger for general ICU patients being a hemoglobin level of 8 g/d. L. The most common transfusion trigger for ICU patients who had cardiovascular disease was 10 g/d. L

The mean baseline hemoglobin level was 11. 0± 2. 4 g/d. L, with 32% having levels of ≥ 12 g/d. L, 14. 9% having 11 to 12 g/d. L, 17. 8% having 10 to 11 g/d. L, 17. 1% having 9 to 19 g/d. L, and 18% having <9 g/d. L A total of 44. 1% of patients had transfusions during their ICU stays, receiving an average of 4. 6± 4. 9 units of blood that was a mean of 21. 3± 11. 4 days old at a mean pretransfusion hemoglobin level of 8. 6± 1. 7 g/d. L. Most commonly, they received 2 units of blood. Hemoglobin levels fell throughout the ICU stay from a mean of 11. 0 g/d. L at baseline (4, 892 patients) to <10. 5 g/d. L by days 28 through 30 (207 patients).
 (More Pulm. CCM Topic Updates)")
Anemia in the ICU: Review and Update (Oct 2014) (More Pulm. CCM Topic Updates) Anemia is almost inevitable during many episodes of critical illness, and has been associated with worsened outcomes and prognosis. However, the preponderance of evidence suggests that correcting anemia (by transfusion or with erythropoetin) does not help most critically ill patients. Although a restrictive transfusion threshold of hemoglobin 7 g/d. L is appropriate for most ICU patients, controversy remains as to whether certain patients might benefit from transfusion to higher hemoglobin levels, such as patients with acute coronary syndromes, GI bleeds, or who are unable to wean from mechanical ventilation.
 >95% of patients in the")
Anemia in the ICU: Review and Update (Oct 2014) >95% of patients in the ICU are anemic after their first week in the IC healthy replacement rate for red blood cells is 15 -20 m. L/day, but dai phlebotomy in the ICU steals 40 -70 m. L (of which only about 1 m. L i actually tested inside the machines); this modern-day “bloodletting” responsible for a third of blood transfusions anemia and worsened outcomes, including mortality, failure to wean from mechanical ventilation, and myocardial infarction. However, no study has clearly shown that anemia is directly causative of poor outcomes, or if it is merely a marker for more severe disease; eliminating confounding from such studies is difficult or impossible.

harms may partially account for the observed association between transfusion and worsened outcomes (pooled odds ratios: mortality 1. 7, ARDS 2. 5, nosocomial infection 1. 8 for transfused patients). A large 2014 meta-analysis provided convincing evidence that libera blood transfusion (to >8 g/d. L) results in nosocomial infections, w a number needed to harm of 20 -40 patients transfused liberally to cau a hospital-acquired infection. Shander A. Crit Care Clin. 2004 Apr; 20(2): 159 -78.

Transfusion Thresholds or “Triggers” in the ICU: TRICC Trial The TRICC trial is the only randomized trial testing transfusion thresholds in critically ill adults. Among 838 euvolemic patients with normal baseline hemoglobin and no active cardiac ischemia or bleeding, there was no difference in all-cause 30 -day mortality between patients transfused to a restrictive threshold or trigger of hemoglobin 7 g/d. L, as compared to those transfused liberally to 10 g/d. L. In post hoc subgroup analyses, theyoungest (<55 years) and least ill (APACHE < 20) patients receiving restrictive . Hebert PC, Wells G, Blajchman MA, et al: A transfusions (who received much less blood) had decreased multicenter, randomized, controlled clinical mortality compared to age- and illness-matched patients transfused trial of transfusion requirements in critical liberally. care: Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. N Engl J Med 1999; 340: 409– 417

mixed venous oxygen saturation. This severe sepsis “early goal directe dle improved mortality and became standard of care, but the relative c sfusion to the observed benefit is unknown, has never been independe monstrated, and is at arguably at odds with the findings of TRICC. A la domized multicenter trial (Pro. CESS) seemed to refute the need for blo necessary part of treatment of sepsis or septic shock. venting Anemia in the ICU ogenic blood loss in critically ill patients should be minimized by: ng small-volume (2 m. L) phlebotomy tubes; ng a closed-system arterial catheter — standard arterial catheters resul od being taken from the patient thanks to convenience and frequent dis hed blood. oiding bleeding the patient with daily blood draws, which are usually u are advised against by Choosing Wisely guidelines for critical care. I , don’t tell, don’t need to transfuse later”). thropoeitin, blood substitutes, and intravenous iron supplementation a troversial, with risks and costs that potentially far outweigh any possib

maintain mean arterial hyperoxia at ssure at _60 mm Hg. In the second clinically relevant levels of tocol, the authors hemodiluted the anemia (70 mals until death, maintaining the g/L) is associated with an arterial pressure at _60 mm Hg in preferential perfusion norepinephrine group. In both experiments, of the renal, splanchnic, and use of norepinephrine significantly hepatic proved or prolonged survival vascular beds at the expense of mpared with controls and increased myocardial tolerated hemodilution before death. and skeletal muscle circulations (12). Гипероксия – смещение кровотока These data suggest that eier J, Pape A, Loniewska D, et al: hyperoxia might not be the most effective orepinephrine creases tolerance to acute anemia. intervention to rit Care Med 2007; 35: 1484– 1492 protect myocardial function during severe

Red cell transfusion is indicated to increase the oxygen delivering capacity of the blood when acute or chronic anaemia contributes to inadequate oxygen delivery to tissues
, оттекающей от различных органов Сa-v. O 2")
Насыщение кислородом венозной крови (Sv. O 2%), оттекающей от различных органов Сa-v. O 2 мл/л кожа, почки – 10; печень – 40; мозг – 60; мышцы – 80; сердце – 110. 37% Для миокарда характерны: наиболее высокий КЭО 2 (> 50%) наиболее низкое Sv. O 2 наиболее низкий резерв О 2 миокард является наиболее чувствительным к снижению доставки кислорода и, соответственно, кислородной ёмкости крови. 51
Анемия_Ждать_ФАР2014.ppt