

71f99e0b5181606ccd5b444810fe6c20.ppt
- Количество слайдов: 27
-DMS & CONNECT MAQUET – JOCAP MEDTRONIC –VIPER…VISION TERUMO-TLINK") DATA CAPTURE AND MANAGEMENT SORIN/DIDECO(LIVA NOVA)-DMS & CONNECT MAQUET – JOCAP MEDTRONIC –VIPER…VISION TERUMO-TLINK
DATA CAPTURE AND MANAGEMENT SORIN/DIDECO(LIVA NOVA)-DMS & CONNECT MAQUET – JOCAP MEDTRONIC –VIPER…VISION TERUMO-TLINK

 •") Perfusion electronic recording system history • First platform –Computer aided perfusion system (CAPS) • DMS developed following CAPS by Sorin in the early 90’s • First UK implementation 1997 St George’s and built on Windows platform. Peak commissioning number at 22 centres nationally before being superseded again by the CONNECT system • JOCAP version 1 also commissioned in 1996/7 and newer versions rolled out (Windows based) to present day • Terumo Tlink DMS available since 2010 • Viper Vision perfusion data management system
Perfusion electronic recording system history • First platform –Computer aided perfusion system (CAPS) • DMS developed following CAPS by Sorin in the early 90’s • First UK implementation 1997 St George’s and built on Windows platform. Peak commissioning number at 22 centres nationally before being superseded again by the CONNECT system • JOCAP version 1 also commissioned in 1996/7 and newer versions rolled out (Windows based) to present day • Terumo Tlink DMS available since 2010 • Viper Vision perfusion data management system
 CONSIDERATIONS OF A SYSTEM • • CHOICE OF SYSTEM MANUFACTURER KNOW HOW/EXPERTISE COMPREHENSIVENESS OF CONNECTIVITY ARCHITECTURE HOST ORGANISATION ICT SUPPORT/EXPERTISE RELIABILITY/RESILIENCE DATA INTEGRITY/STORAGE/ACCESSIBILITY EASE OF USE (plug in and play)
CONSIDERATIONS OF A SYSTEM • • CHOICE OF SYSTEM MANUFACTURER KNOW HOW/EXPERTISE COMPREHENSIVENESS OF CONNECTIVITY ARCHITECTURE HOST ORGANISATION ICT SUPPORT/EXPERTISE RELIABILITY/RESILIENCE DATA INTEGRITY/STORAGE/ACCESSIBILITY EASE OF USE (plug in and play)
 CENTRAL SYSTEM AND PERIPHERAL DEVICE CONNECTIVITY • • RS 232 AUX PC USB DONGLE WI-FI Ethernet Serial device servers
CENTRAL SYSTEM AND PERIPHERAL DEVICE CONNECTIVITY • • RS 232 AUX PC USB DONGLE WI-FI Ethernet Serial device servers
.") DATA AND CAPTURE • SOPGBI Recommendations for Standards of Monitoring during cardiopulmonary bypass (2007). • “where a variable is monitored it should be regularly recorded” • “All units should have electronic acquisition and storage of this data including the ability to produce a printout” • “ Records should be retained in the patients notes and electronically”
DATA AND CAPTURE • SOPGBI Recommendations for Standards of Monitoring during cardiopulmonary bypass (2007). • “where a variable is monitored it should be regularly recorded” • “All units should have electronic acquisition and storage of this data including the ability to produce a printout” • “ Records should be retained in the patients notes and electronically”
 versus Automated (Ottens et al; 2005) • “Manual cannot offer the complete picture") Manual(Handwritten) versus Automated (Ottens et al; 2005) • “Manual cannot offer the complete picture of what has happened during the bypass period” • “Anaesthesia: reported a bias in the handwritten record and data were normalised toward expected rather than actual” • Results demonstrated a statistically significant difference
Manual(Handwritten) versus Automated (Ottens et al; 2005) • “Manual cannot offer the complete picture of what has happened during the bypass period” • “Anaesthesia: reported a bias in the handwritten record and data were normalised toward expected rather than actual” • Results demonstrated a statistically significant difference
 PERCEIVED ADVANTAGES/DISADVANTAGES OF DATA MANAGEMENT SYSTEMS TO THE PERFUSION SCIENTIST ADVANTAGES DISADVANTAGES EVENT RECORDING FREQUENCY OF RECORDING REDUCED WRITING CUSTOMISED REPORTING CONTINUOUS RECORDING RETROSPECTIVE ANALYSIS/COMMENTING ENDLESS PARAMETER TRACKING PROTECTIVE CUSTOMISATION QUALITY INDICATORS TRUE UNADULTERATED DATA “CHANGE” CONNECTIVITY RELIABILITY CHARTING BIG BROTHER ELEMENT DEPENDENCY “HEAT OF THE MOMENT PROBLEMS” ORGANISATIONAL ICT SUPPORT CUSTOMISATION THAT SUITS ALL THE PERFUSION DEPARTMENT STAFF
PERCEIVED ADVANTAGES/DISADVANTAGES OF DATA MANAGEMENT SYSTEMS TO THE PERFUSION SCIENTIST ADVANTAGES DISADVANTAGES EVENT RECORDING FREQUENCY OF RECORDING REDUCED WRITING CUSTOMISED REPORTING CONTINUOUS RECORDING RETROSPECTIVE ANALYSIS/COMMENTING ENDLESS PARAMETER TRACKING PROTECTIVE CUSTOMISATION QUALITY INDICATORS TRUE UNADULTERATED DATA “CHANGE” CONNECTIVITY RELIABILITY CHARTING BIG BROTHER ELEMENT DEPENDENCY “HEAT OF THE MOMENT PROBLEMS” ORGANISATIONAL ICT SUPPORT CUSTOMISATION THAT SUITS ALL THE PERFUSION DEPARTMENT STAFF
 SOCIETY CODE REGARDING DATA CAPTURE The member shall maintain an accurate record of all clinical activities
SOCIETY CODE REGARDING DATA CAPTURE The member shall maintain an accurate record of all clinical activities
 MORRISTON HOSPITAL SET UP
MORRISTON HOSPITAL SET UP
 EVENT CUSTOMISATION
EVENT CUSTOMISATION
 CLOSE UP…
CLOSE UP…
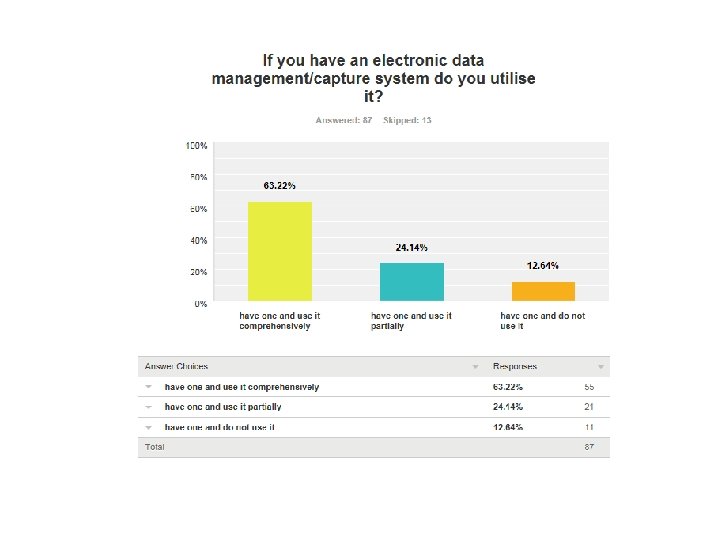
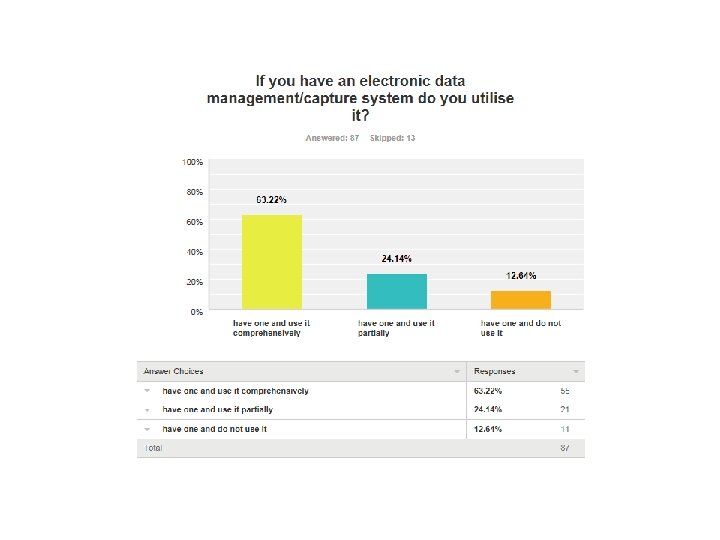
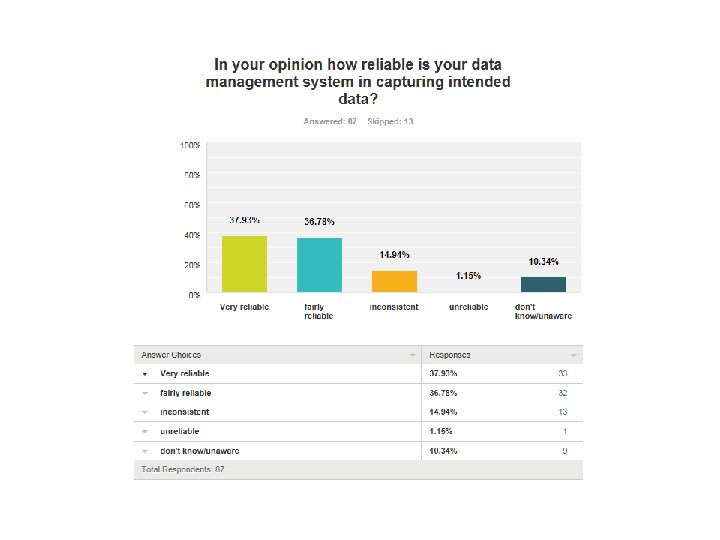
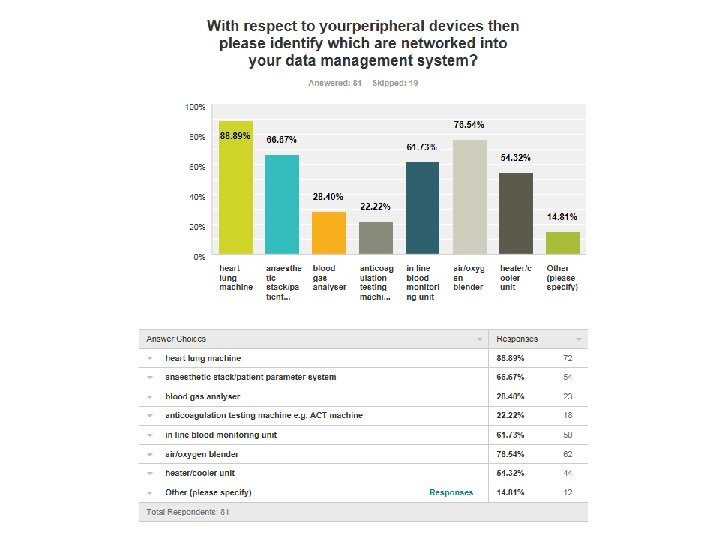
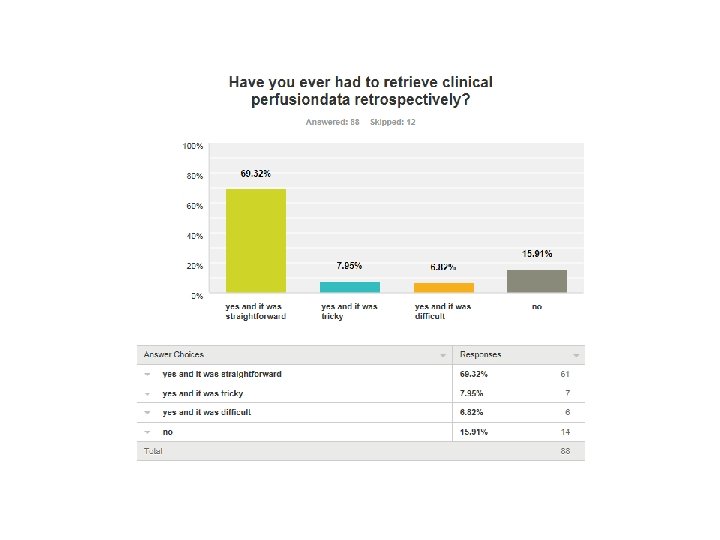
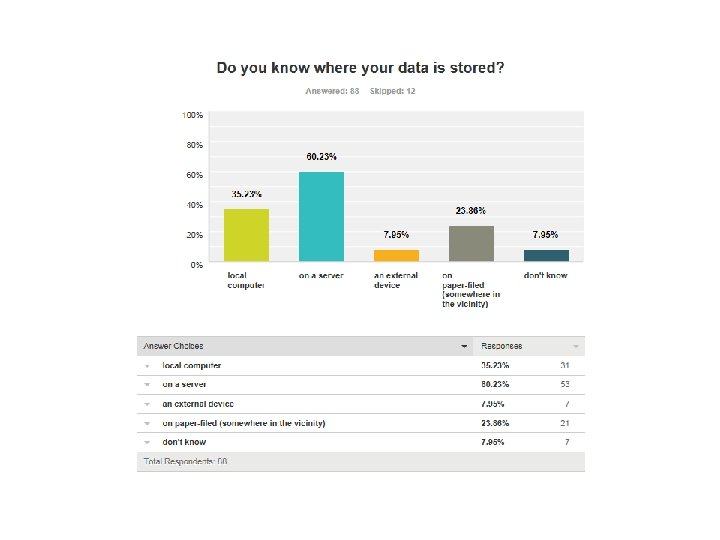
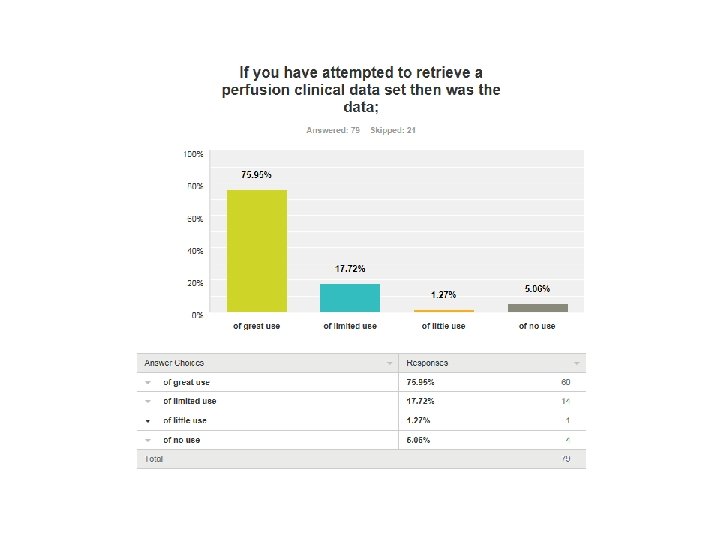
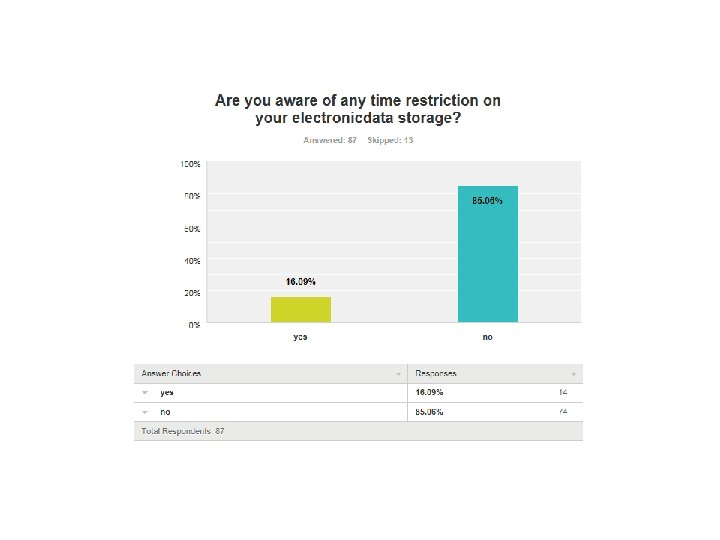
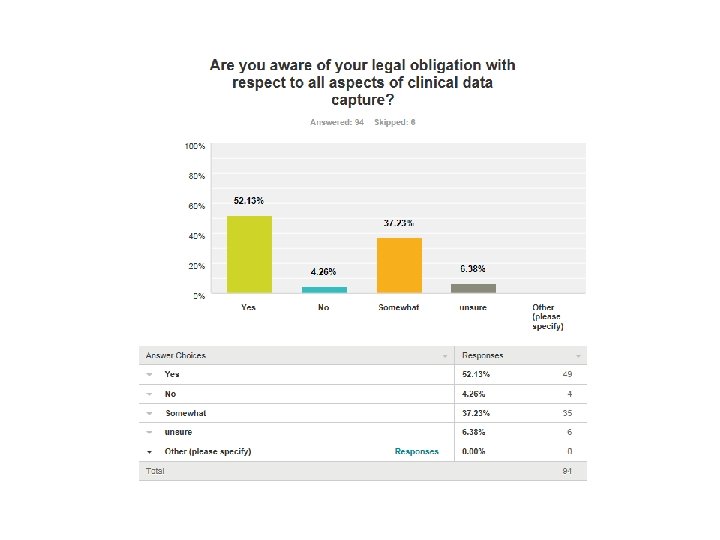
 RECENT SURVEY
RECENT SURVEY
 Some free text and email responses • • • • I like the electronic capture because my handwriting is appalling and not particularly legible plus I think it captures much more information. . . I’m sticking to what I do best. . . manual. . paper chart I am apprehensive about my DMS as it isn’t reliable and if there is a problem I stress and try to remedy it which nearly always means that I miss telling the surgeon the plegia time I find my data management system distracting and I am not an IT wizzard Love my manual record We have half the department using it and half not. No, they/we try but it isn’t reliable and is time consuming I find it very distracting to my clinical practice , period. Love it, wish we could go all electronic!!!great My chart is my pride and joy, I just don’t have the faith or confidence with the system (data management system) I found moving over to the electronic data management system very difficult, not an easy process but I’m glad that I have. I find that I have more in common with my younger colleagues and I have embraced other technologies as well What I find is that I like the concept, all is well with a case then there are major gremlins and I find it so, so distracting and a stressor. My chart is my rock The companies suck. My colleague has spent hundreds of painstaking hours trying to get a “fit” system and my Chief just tolerates it. Its that bunion that won’t get better. Love our new system. It gives me so much information and it reassures me
Some free text and email responses • • • • I like the electronic capture because my handwriting is appalling and not particularly legible plus I think it captures much more information. . . I’m sticking to what I do best. . . manual. . paper chart I am apprehensive about my DMS as it isn’t reliable and if there is a problem I stress and try to remedy it which nearly always means that I miss telling the surgeon the plegia time I find my data management system distracting and I am not an IT wizzard Love my manual record We have half the department using it and half not. No, they/we try but it isn’t reliable and is time consuming I find it very distracting to my clinical practice , period. Love it, wish we could go all electronic!!!great My chart is my pride and joy, I just don’t have the faith or confidence with the system (data management system) I found moving over to the electronic data management system very difficult, not an easy process but I’m glad that I have. I find that I have more in common with my younger colleagues and I have embraced other technologies as well What I find is that I like the concept, all is well with a case then there are major gremlins and I find it so, so distracting and a stressor. My chart is my rock The companies suck. My colleague has spent hundreds of painstaking hours trying to get a “fit” system and my Chief just tolerates it. Its that bunion that won’t get better. Love our new system. It gives me so much information and it reassures me
 And more. . . • • • Its taken two years to get ours working properly and what a faff. Like the principle though. . Why is it the system always goes down on a difficult, complex case? Believe me Tony, when you have the turnaround we do you do not want or wish to be mucking around with introducing data on a system when it is your only time for a break! The monitors we use are rubbish and are already out of date When it hits the fan you don’t have time to write but with an electronic system its easy and you can go back and create a narrative or explanation. When our perfusionist colleague who takes the lead with our DMS system is on holiday or day off the rest of us don’t have an appreciable knowledge of the system so we just fumble and focus on the pump chart I get so immersed in our system that sometimes I genuinely focus on the system more than the patient which seems a terrible thing to say. You sort of become a robot We have a data management perfusion system, Jocap but somehow writing a record seems more real and human and more personalised. For me it is necessary I don’t think that any one system is the right one. One should complement the other
And more. . . • • • Its taken two years to get ours working properly and what a faff. Like the principle though. . Why is it the system always goes down on a difficult, complex case? Believe me Tony, when you have the turnaround we do you do not want or wish to be mucking around with introducing data on a system when it is your only time for a break! The monitors we use are rubbish and are already out of date When it hits the fan you don’t have time to write but with an electronic system its easy and you can go back and create a narrative or explanation. When our perfusionist colleague who takes the lead with our DMS system is on holiday or day off the rest of us don’t have an appreciable knowledge of the system so we just fumble and focus on the pump chart I get so immersed in our system that sometimes I genuinely focus on the system more than the patient which seems a terrible thing to say. You sort of become a robot We have a data management perfusion system, Jocap but somehow writing a record seems more real and human and more personalised. For me it is necessary I don’t think that any one system is the right one. One should complement the other
 LET US REFLECT • We have come a long way in relatively short time or have we? • More to manage; hardware, software, connectivity, data protection, more parameters, more analysis of physiological status • From the results of the survey and having met with many perfusionists in many departments I feel that if the implementation and running of data management systems had been a more smooth and reliable experience then we wouldn’t have what appears to be a very cynical view in many respects. • Any approach that demonstrates accuracy and strengthens clinical performance through data capture should be welcome but not at the expense of safety. • Reliability and faith is extremely important as is competence with the “system”. • RONSEAL principle: Does it do what it says on the tin!
LET US REFLECT • We have come a long way in relatively short time or have we? • More to manage; hardware, software, connectivity, data protection, more parameters, more analysis of physiological status • From the results of the survey and having met with many perfusionists in many departments I feel that if the implementation and running of data management systems had been a more smooth and reliable experience then we wouldn’t have what appears to be a very cynical view in many respects. • Any approach that demonstrates accuracy and strengthens clinical performance through data capture should be welcome but not at the expense of safety. • Reliability and faith is extremely important as is competence with the “system”. • RONSEAL principle: Does it do what it says on the tin!
 conclusion • Do we all carry on with the status quo? • There are clearly some minor and major issues in some centres with data management systems. • Is poor connectivity down to reliability or system design • Should we treat an ICT fault the same as a hardware fault? • What are the barriers? • Should the companies do more? ? • Do hospital ICT departments have more of an obligation to help? • Should the membership or society consider exemplar units to advertise their ICT success/prowess?
conclusion • Do we all carry on with the status quo? • There are clearly some minor and major issues in some centres with data management systems. • Is poor connectivity down to reliability or system design • Should we treat an ICT fault the same as a hardware fault? • What are the barriers? • Should the companies do more? ? • Do hospital ICT departments have more of an obligation to help? • Should the membership or society consider exemplar units to advertise their ICT success/prowess?
 THANK YOU
THANK YOU