

2a65c7db1d96c3e1cea811a279b86209.ppt
- Количество слайдов: 40
 Cryptogenic Stroke and PFO: The Hole Story: Anthony J Furlan MD Gilbert W Humphrey Professor Chairman Department of Neurology University Hospitals Case Medical Center
Cryptogenic Stroke and PFO: The Hole Story: Anthony J Furlan MD Gilbert W Humphrey Professor Chairman Department of Neurology University Hospitals Case Medical Center
 DISCLOSURES • Principal Investigator – CLOSURE I • NMT Medical, Boston
DISCLOSURES • Principal Investigator – CLOSURE I • NMT Medical, Boston
 PFO in Embolic Stroke PFO in stroke: The principle is sound. How real is the problem? PRA RA PLA LA
PFO in Embolic Stroke PFO in stroke: The principle is sound. How real is the problem? PRA RA PLA LA
 TEE
TEE
 Kaplan-Meier curves of cumulative risk") Patent foramen ovale In Cryptogenic Stroke Study (PICSS) Kaplan-Meier curves of cumulative risk of recurrent stroke or death stratified by baseline PFO status. Homma: Circulation, Volume 105(22). June 4, 2002. 2625 -2631
Patent foramen ovale In Cryptogenic Stroke Study (PICSS) Kaplan-Meier curves of cumulative risk of recurrent stroke or death stratified by baseline PFO status. Homma: Circulation, Volume 105(22). June 4, 2002. 2625 -2631
 Probability That Patients Will Remain Free from Recurrent Stroke or TIA The log-rank test was used to calculate the P value. Mas: N Engl J Med, Volume 345(24). December 13, 2001. 1740 -1746
Probability That Patients Will Remain Free from Recurrent Stroke or TIA The log-rank test was used to calculate the P value. Mas: N Engl J Med, Volume 345(24). December 13, 2001. 1740 -1746
 Kaplan-Meier estimate of survival free of cerebrovascular events in 577 subjects according to TEE presence of patent foramen ovale (PFO) SPARC Mayo METHODS: The use of transesophageal echocardiography to identify PFO was performed by a single echocardiographer using standardized definitions in 585 randomly sampled, Olmsted County (Minnesota) subjects age 45 years or older participating in the Stroke Prevention: Assessment of Risk in a Community (SPARC) study. Meissner, I. et al. J Am Coll Cardiol 2006; 47: 440 -445
Kaplan-Meier estimate of survival free of cerebrovascular events in 577 subjects according to TEE presence of patent foramen ovale (PFO) SPARC Mayo METHODS: The use of transesophageal echocardiography to identify PFO was performed by a single echocardiographer using standardized definitions in 585 randomly sampled, Olmsted County (Minnesota) subjects age 45 years or older participating in the Stroke Prevention: Assessment of Risk in a Community (SPARC) study. Meissner, I. et al. J Am Coll Cardiol 2006; 47: 440 -445
 PICSS 2 -Year Stroke or Death Rate Warfarin versus Aspirin 20% 18% 16. 50% 16% 14% 13. 20% 17. 40% 17. 90% 16. 30% 13. 40% 12% 9. 50% 10% 8% 8. 30% ASA Warfarin 6% 4% 2% 0% With PFO N=203 (P=0. 49) No PFO N=398 (P=0. 40) With PFO (cryptogenic) No PFO (cryptogenic) N=98 (P=0. 28) N=152 (P=0. 16) Homma S et al. Circulation. 2002; 105: 2625 -2631.
PICSS 2 -Year Stroke or Death Rate Warfarin versus Aspirin 20% 18% 16. 50% 16% 14% 13. 20% 17. 40% 17. 90% 16. 30% 13. 40% 12% 9. 50% 10% 8% 8. 30% ASA Warfarin 6% 4% 2% 0% With PFO N=203 (P=0. 49) No PFO N=398 (P=0. 40) With PFO (cryptogenic) No PFO (cryptogenic) N=98 (P=0. 28) N=152 (P=0. 16) Homma S et al. Circulation. 2002; 105: 2625 -2631.
 PFO & Stroke: Metanalysis Outcomes Transcatheter Closure vs. Medical Therapy of PFO and presumed Paradoxical event: A systematic review. Landzberg, et al. Annals of Internal Medicine 2003 Recurrent event rates @ 1 Yr. Complication rates Key Data Weaknesses Medical Therapy 3. 8 – 12. 0% Major: 1%/yr on warfarin Poor match to PFO population. Significant variation in INR targets. Catheter Closure 0% - 4. 9% Major: 1. 5% Minor: 7. 9% Significant selection bias. Significant variation in post implant pharm.
PFO & Stroke: Metanalysis Outcomes Transcatheter Closure vs. Medical Therapy of PFO and presumed Paradoxical event: A systematic review. Landzberg, et al. Annals of Internal Medicine 2003 Recurrent event rates @ 1 Yr. Complication rates Key Data Weaknesses Medical Therapy 3. 8 – 12. 0% Major: 1%/yr on warfarin Poor match to PFO population. Significant variation in INR targets. Catheter Closure 0% - 4. 9% Major: 1. 5% Minor: 7. 9% Significant selection bias. Significant variation in post implant pharm.
 What WAS* the HDE Indication for PFO Device Closure? The Cardio. SEAL Septal Occlusion System is indicated for closure of PFO in: a Patients with recurrent cryptogenic stroke due to presumed paradoxical embolus through the PFO who have failed medical therapy. Cryptogenic stroke is defined as a stroke occurring in the absence of potential phanerogenic, cardiac, pulmonary, vascular, or neurological sources. Conventional drug therapy is defined as a therapeutic INR on oral anticoagulants. The effectiveness of this device in this indication has not been demonstrated. HDE did not include TIA, migraine, or first stroke and required warfarin failure *HDE withdrawn by CMS October 2006 with no impact on CLOSURE recruitment rate
What WAS* the HDE Indication for PFO Device Closure? The Cardio. SEAL Septal Occlusion System is indicated for closure of PFO in: a Patients with recurrent cryptogenic stroke due to presumed paradoxical embolus through the PFO who have failed medical therapy. Cryptogenic stroke is defined as a stroke occurring in the absence of potential phanerogenic, cardiac, pulmonary, vascular, or neurological sources. Conventional drug therapy is defined as a therapeutic INR on oral anticoagulants. The effectiveness of this device in this indication has not been demonstrated. HDE did not include TIA, migraine, or first stroke and required warfarin failure *HDE withdrawn by CMS October 2006 with no impact on CLOSURE recruitment rate

 Original N = 1600 Revised N = 900") CLOSURE I Cumulative Enrollment (87 sites) Original N = 1600 Revised N = 900 HDE 2/00 N revised HDE removed 10/06
CLOSURE I Cumulative Enrollment (87 sites) Original N = 1600 Revised N = 900 HDE 2/00 N revised HDE removed 10/06
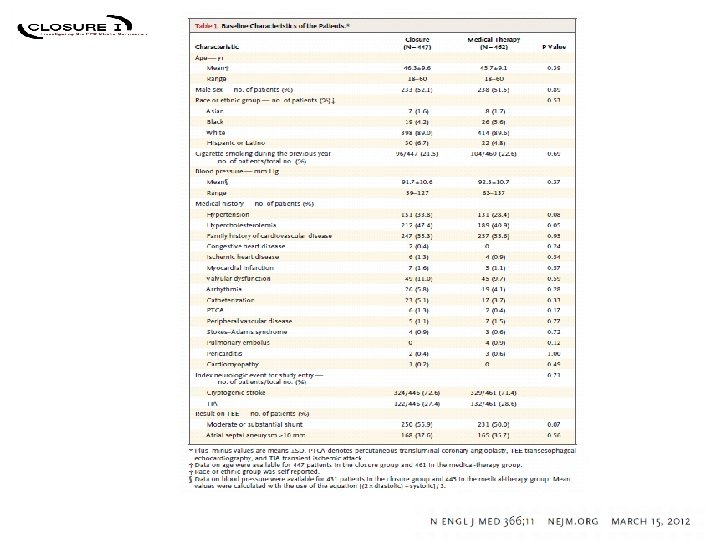
 6") Randomization 1 : 1 N = 909 N=447 STARFlex® Closure (within 30 Days) 6 Months Aspirin and Clopidigrel followed by 18 Months Aspirin N=462 Best Medical Therapy 24 Months Aspirin Or Warfarin Or Combination Between June 23, 2003 and October 24, 2008, 909 patients were randomized at 87 sites in the United States and Canada. Block randomization with stratification by study site and by the presence or absence of an ASA viewed by TEE.
Randomization 1 : 1 N = 909 N=447 STARFlex® Closure (within 30 Days) 6 Months Aspirin and Clopidigrel followed by 18 Months Aspirin N=462 Best Medical Therapy 24 Months Aspirin Or Warfarin Or Combination Between June 23, 2003 and October 24, 2008, 909 patients were randomized at 87 sites in the United States and Canada. Block randomization with stratification by study site and by the presence or absence of an ASA viewed by TEE.
 STARFlex® • Double umbrella comprised of MP 35 N framework with attached polyester fabric • 23 mm, 28 mm, 33 mm 17
STARFlex® • Double umbrella comprised of MP 35 N framework with attached polyester fabric • 23 mm, 28 mm, 33 mm 17
 STARFlex Technical Success STARFlex n=402 Procedural success Thrombus by TEE 95% CI 90. 0% (86. 7% - 92. 8%) 1. 0% (n=4; stroke in 2 at days 4, 52) Effective closure No recurrent stroke or TIA in patients with residual leaks TEE 6 mos 86. 1% closed (82. 1% - 89. 4%) TEE 12 mos 86. 4% closed (82. 5% - 89. 8%) 86. 7% closed (82. 8% - 90. 0%) TEE 24 mos Procedural success was defined as successful delivery of one or more STARFlex devices to the site during the index procedure, deployment of the device at the intended site, and removal of the delivery system without a major procedural complication prior to discharge. Effective closure was defined as procedural success with either grade 0 (none) or 1 (trace) residual shunt by TEE.
STARFlex Technical Success STARFlex n=402 Procedural success Thrombus by TEE 95% CI 90. 0% (86. 7% - 92. 8%) 1. 0% (n=4; stroke in 2 at days 4, 52) Effective closure No recurrent stroke or TIA in patients with residual leaks TEE 6 mos 86. 1% closed (82. 1% - 89. 4%) TEE 12 mos 86. 4% closed (82. 5% - 89. 8%) 86. 7% closed (82. 8% - 90. 0%) TEE 24 mos Procedural success was defined as successful delivery of one or more STARFlex devices to the site during the index procedure, deployment of the device at the intended site, and removal of the delivery system without a major procedural complication prior to discharge. Effective closure was defined as procedural success with either grade 0 (none) or 1 (trace) residual shunt by TEE.
 DM/CABG/valve/CVA day 627 index. ACA Age 60 multiple TIA spells/30 sec focal with DW+/TEE neg Index punctate MCA Etiology unclear Afib/Laclot on day 16/stroke day 52 Multiple punctate Afibflutter/CVA day 22 PAF/valve disease/day 238 Star. Flex Arm Recurrent DWMR+ infarcts (n= 7/12; wnl 2; not done 3) heart cath with 3 stents on day 232 LA clot on TEE day 4 Multiple punctate Afib 3/ LA clot 1/ heart cath 1/ ASO 1 5/7 different area from index 4/7 single territory 2/7 multiple same territory 1/7 multiple territories
DM/CABG/valve/CVA day 627 index. ACA Age 60 multiple TIA spells/30 sec focal with DW+/TEE neg Index punctate MCA Etiology unclear Afib/Laclot on day 16/stroke day 52 Multiple punctate Afibflutter/CVA day 22 PAF/valve disease/day 238 Star. Flex Arm Recurrent DWMR+ infarcts (n= 7/12; wnl 2; not done 3) heart cath with 3 stents on day 232 LA clot on TEE day 4 Multiple punctate Afib 3/ LA clot 1/ heart cath 1/ ASO 1 5/7 different area from index 4/7 single territory 2/7 multiple same territory 1/7 multiple territories
 Medical Arm - Recurrent DW+ Infarcts Age 43/day 32/ multiple subcortical/ ? MS ? Vasculitis Clinical TIA Age 35/d 1 y 122/migraine/ clinical TIA NIH 0/ Angio neg/ multiple DW+ BG, IC, cerebellum ? paradoxical Age 42/day 146/migraine/clinical TIA/NIH 0/warfarin/? paradoxical Age 60/migraine with aura/ Day 143 sudden left fingers only NIH 0/old lac unes Age 59/day 143/htn; smoker; hpl NIH 3 Age 31/migraine/day 367 Index cerebellar/ ? coincidental / Age 42/index Rparietal /recur L parietal day 150 Switch to warfarin/ ? paradoxical Day 15/htn/hpl/mitral regurg/ possible extension/age 50 Age 53/Day 635/ASO/LCEA (n= 9/13; WNL 4: retinal 1/IV tpa 1/minor sxs >24 hr ? ? migraine 2 6/9 different territory than index ; 5/9 multiple infarcts same territory; 1/9 multiple territories
Medical Arm - Recurrent DW+ Infarcts Age 43/day 32/ multiple subcortical/ ? MS ? Vasculitis Clinical TIA Age 35/d 1 y 122/migraine/ clinical TIA NIH 0/ Angio neg/ multiple DW+ BG, IC, cerebellum ? paradoxical Age 42/day 146/migraine/clinical TIA/NIH 0/warfarin/? paradoxical Age 60/migraine with aura/ Day 143 sudden left fingers only NIH 0/old lac unes Age 59/day 143/htn; smoker; hpl NIH 3 Age 31/migraine/day 367 Index cerebellar/ ? coincidental / Age 42/index Rparietal /recur L parietal day 150 Switch to warfarin/ ? paradoxical Day 15/htn/hpl/mitral regurg/ possible extension/age 50 Age 53/Day 635/ASO/LCEA (n= 9/13; WNL 4: retinal 1/IV tpa 1/minor sxs >24 hr ? ? migraine 2 6/9 different territory than index ; 5/9 multiple infarcts same territory; 1/9 multiple territories
 Exploratory Paradoxical Embolism Analyses 2 Year Composite Primary Endpoint Set ITT ITT Characteristic ≤ 50 minus all subsets <40 P value 0. 14* 0. 61* 0. 10* ITT ITT <40 minus all subsets 0. 40* No HTN history 0. 71 Index crypto stroke minus subcortical 0. 54* ITT No reported afib 0. 10 PP PP PP ≤ 50 ≤ 40 < 50 minus all subsets < 40 minus all subsets No HTN history Index crypto stroke minus subcortical 0. 11* 0. 06* 0. 62* 0. 40* 0. 60 0. 62* PP No reported afib 0. 09 *Adjusting performed using Cox Proportional Hazard Regression and adjusting for related patient characteristics including: age, atrial septal aneurysm, prior TIA/CVA, smoking, hypertension, hypercholesterolemia , subcortical infarcts. ITT = Intent to Treat. PP = Per Protocol
Exploratory Paradoxical Embolism Analyses 2 Year Composite Primary Endpoint Set ITT ITT Characteristic ≤ 50 minus all subsets <40 P value 0. 14* 0. 61* 0. 10* ITT ITT <40 minus all subsets 0. 40* No HTN history 0. 71 Index crypto stroke minus subcortical 0. 54* ITT No reported afib 0. 10 PP PP PP ≤ 50 ≤ 40 < 50 minus all subsets < 40 minus all subsets No HTN history Index crypto stroke minus subcortical 0. 11* 0. 06* 0. 62* 0. 40* 0. 60 0. 62* PP No reported afib 0. 09 *Adjusting performed using Cox Proportional Hazard Regression and adjusting for related patient characteristics including: age, atrial septal aneurysm, prior TIA/CVA, smoking, hypertension, hypercholesterolemia , subcortical infarcts. ITT = Intent to Treat. PP = Per Protocol
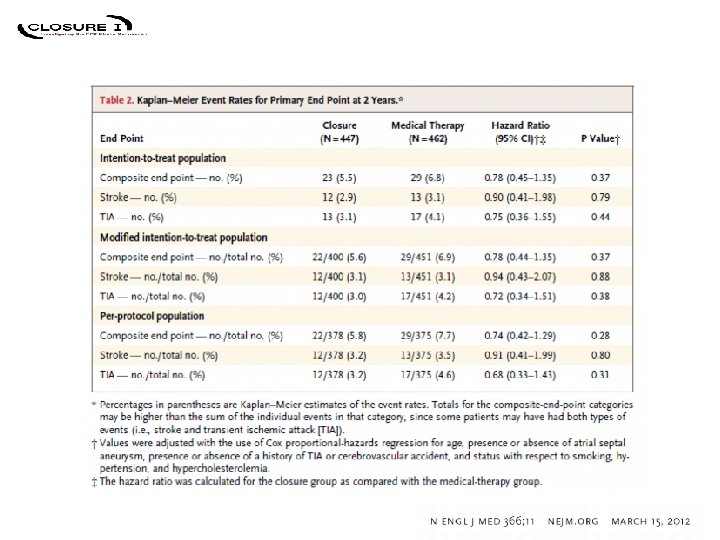
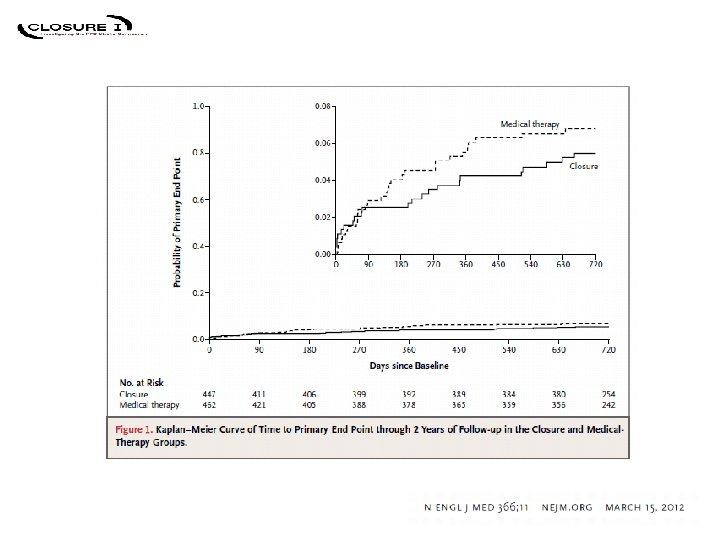
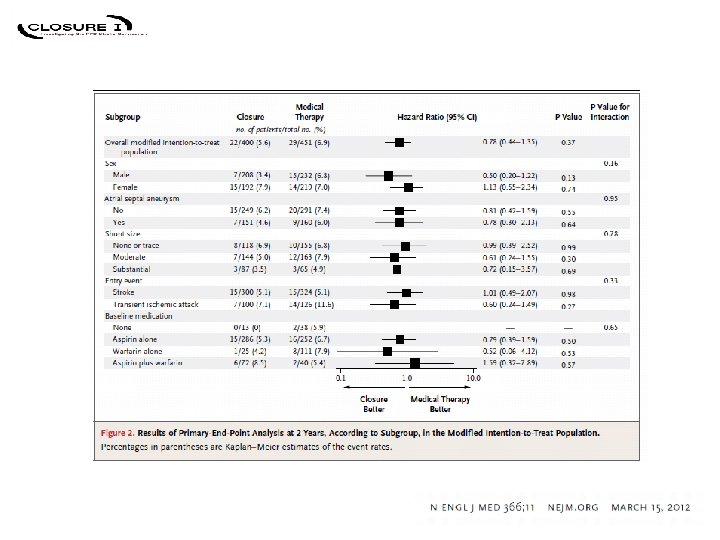
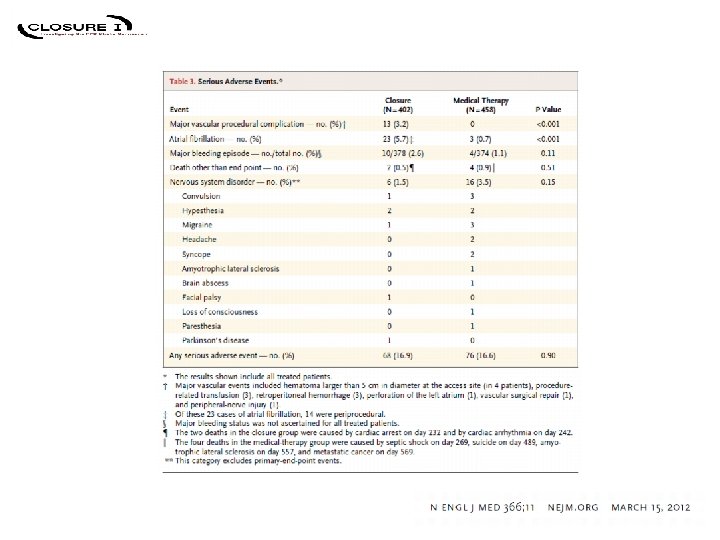
 CONCLUSIONS • CLOSURE I is the first completed, prospective, randomized, independently adjudicated PFO device closure study • Superiority of PFO closure with STARFlex® plus medical therapy over medical therapy alone was not demonstrated – – no significant benefit related to degree of initial shunt no significant benefit with atrial septal aneurysm insignificant trend (1. 8%) favoring device driven by TIA 2 year stroke rate essentially identical in both arms (3%) • Major vascular (procedural) complications in 3% of device arm • Significantly higher rate of atrial fibrillation in device arm (5. 7%) – 60% periprocedural
CONCLUSIONS • CLOSURE I is the first completed, prospective, randomized, independently adjudicated PFO device closure study • Superiority of PFO closure with STARFlex® plus medical therapy over medical therapy alone was not demonstrated – – no significant benefit related to degree of initial shunt no significant benefit with atrial septal aneurysm insignificant trend (1. 8%) favoring device driven by TIA 2 year stroke rate essentially identical in both arms (3%) • Major vascular (procedural) complications in 3% of device arm • Significantly higher rate of atrial fibrillation in device arm (5. 7%) – 60% periprocedural
 CONCLUSIONS • Alternative explanation unrelated to paradoxical embolism present in 80% of patients with recurrent stroke or TIA – cryptogenic stroke and TIA include multiple etiologies – in many patients with cryptogenic stroke or TIA a PFO may be coincidental – diagnostic criteria for paradoxical embolism are imprecise • Percutaneous closure with STARFlex® plus medical therapy does not offer any significant benefit over medical therapy alone for the prevention of recurrent stroke or TIA in patients < age 60 presenting with cryptogenic stroke or TIA and a PFO – initial medical therapy appropriate in most patients – device specific complications need further study but not likely to explain CLOSURE I results by themselves – potential efficacy of PFO device closure in better defined patient subgroups requires further study
CONCLUSIONS • Alternative explanation unrelated to paradoxical embolism present in 80% of patients with recurrent stroke or TIA – cryptogenic stroke and TIA include multiple etiologies – in many patients with cryptogenic stroke or TIA a PFO may be coincidental – diagnostic criteria for paradoxical embolism are imprecise • Percutaneous closure with STARFlex® plus medical therapy does not offer any significant benefit over medical therapy alone for the prevention of recurrent stroke or TIA in patients < age 60 presenting with cryptogenic stroke or TIA and a PFO – initial medical therapy appropriate in most patients – device specific complications need further study but not likely to explain CLOSURE I results by themselves – potential efficacy of PFO device closure in better defined patient subgroups requires further study
 NMT Medical, Inc. Assigns All of Its Assets for the Benefit of Creditors Company Release - 04/19/2011 16: 05 BOSTON, MA -- (MARKET WIRE) -- 04/19/11 -- NMT Medical, Inc. (OTCQB: NMTI) (PINKSHEETS: NMTI) today announced that, despite the Company's efforts to obtain additional financing and identify potential strategic transactions, it has failed to raise additional funds or enter into such strategic transaction and, therefore, it has entered into an Assignment for the Benefit of Creditors, effective immediately, in accordance with Massachusetts law (the "Assignment"). The purpose of the Assignment is to conclude the Company's operations and provide for an orderly liquidation of its assets. The Company previously disclosed that it did not have resources to sufficiently fund its continuing business operation and additional capital was required to remain a going concern, and the Company had been seeking strategic alternatives, including financings, recapitalization, sale or disposition of one or more corporate assets, a potential merger and/or a strategic business combination, with various third parties over the course of the past year. The Assignment is a common law business liquidation mechanism under Massachusetts law that is an alternative to a formal bankruptcy proceeding. Under the terms of the Assignment, the Company transferred all of its assets to an assignee for orderly liquidation and distribution of the proceeds to the Company's creditors. The designated assignee for the Company is Joseph F. Finn, Jr. For creditors and other affected parties of NMT Medical, Inc. all inquiries related to this action should be addressed to Joseph F. Finn, Jr. at Finn, Warnke and Gayton, 167 Worcester Street, Suite 201, Wellesley Hills, MA 02481 (781 -237 -8840). Following the liquidation of the Company's assets and distribution of proceeds by the assignee, the Company does not expect that there will be any proceeds for distribution to the Company's stockholders. As part of the Assignment, the Company has terminated the employment of all of its employees. This news release contains express or implied forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995 that are based on current expectations of management. These statements relate to, among other things, expectations concerning the transfer of all of the Company's Assets to an assignee under and Assignment for the Benefit of Creditors and matters relating to the payment of creditors. These statements are neither promises nor guarantees, but are subject to a variety of risks and uncertainties, many of which are beyond our control, and which could cause actual results to differ materially from those contemplated in these forward-looking statements. Existing and prospective investors are cautioned not to place undue reliance on these forward-looking statements, which speak only as of the date hereof. We undertake no obligation to update or revise the information contained in this press release, whether as a result of new information, future events or circumstances or otherwise. For additional information regarding these and other risks that we face, see the disclosure contained in our filings with the Securities and Exchange Commission, including our most recent Annual Report on Form 10 -K and subsequent Quarterly Reports on Form 10 -Q. Source: NMT Medical
NMT Medical, Inc. Assigns All of Its Assets for the Benefit of Creditors Company Release - 04/19/2011 16: 05 BOSTON, MA -- (MARKET WIRE) -- 04/19/11 -- NMT Medical, Inc. (OTCQB: NMTI) (PINKSHEETS: NMTI) today announced that, despite the Company's efforts to obtain additional financing and identify potential strategic transactions, it has failed to raise additional funds or enter into such strategic transaction and, therefore, it has entered into an Assignment for the Benefit of Creditors, effective immediately, in accordance with Massachusetts law (the "Assignment"). The purpose of the Assignment is to conclude the Company's operations and provide for an orderly liquidation of its assets. The Company previously disclosed that it did not have resources to sufficiently fund its continuing business operation and additional capital was required to remain a going concern, and the Company had been seeking strategic alternatives, including financings, recapitalization, sale or disposition of one or more corporate assets, a potential merger and/or a strategic business combination, with various third parties over the course of the past year. The Assignment is a common law business liquidation mechanism under Massachusetts law that is an alternative to a formal bankruptcy proceeding. Under the terms of the Assignment, the Company transferred all of its assets to an assignee for orderly liquidation and distribution of the proceeds to the Company's creditors. The designated assignee for the Company is Joseph F. Finn, Jr. For creditors and other affected parties of NMT Medical, Inc. all inquiries related to this action should be addressed to Joseph F. Finn, Jr. at Finn, Warnke and Gayton, 167 Worcester Street, Suite 201, Wellesley Hills, MA 02481 (781 -237 -8840). Following the liquidation of the Company's assets and distribution of proceeds by the assignee, the Company does not expect that there will be any proceeds for distribution to the Company's stockholders. As part of the Assignment, the Company has terminated the employment of all of its employees. This news release contains express or implied forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995 that are based on current expectations of management. These statements relate to, among other things, expectations concerning the transfer of all of the Company's Assets to an assignee under and Assignment for the Benefit of Creditors and matters relating to the payment of creditors. These statements are neither promises nor guarantees, but are subject to a variety of risks and uncertainties, many of which are beyond our control, and which could cause actual results to differ materially from those contemplated in these forward-looking statements. Existing and prospective investors are cautioned not to place undue reliance on these forward-looking statements, which speak only as of the date hereof. We undertake no obligation to update or revise the information contained in this press release, whether as a result of new information, future events or circumstances or otherwise. For additional information regarding these and other risks that we face, see the disclosure contained in our filings with the Securities and Exchange Commission, including our most recent Annual Report on Form 10 -K and subsequent Quarterly Reports on Form 10 -Q. Source: NMT Medical
 RESPECT Amplatzer® Occluder REDUCE Clinical Study HELEXR occluder
RESPECT Amplatzer® Occluder REDUCE Clinical Study HELEXR occluder
 RESPECT
RESPECT
 PC TRIAL
PC TRIAL
 CLOSURE v RESPECT v PC CLOSURE n=909 RESPECT n=980 PC N=414 Inclusion TIA, stroke (MR+”TIA”) “TIA” (MR+) stroke, peripheral Device Starflex clamshell Amplatzer plug Medical aspirin warfarin aspirin, clopidogrel, aggrenox warfarin aspirin, ticlopidine, clopidogrel, warfarin Outcome 2 years TIA/stroke 8 years Event driven 4 years “TIA”/stroke/ peripheral Intent to Treat Primary result negative
CLOSURE v RESPECT v PC CLOSURE n=909 RESPECT n=980 PC N=414 Inclusion TIA, stroke (MR+”TIA”) “TIA” (MR+) stroke, peripheral Device Starflex clamshell Amplatzer plug Medical aspirin warfarin aspirin, clopidogrel, aggrenox warfarin aspirin, ticlopidine, clopidogrel, warfarin Outcome 2 years TIA/stroke 8 years Event driven 4 years “TIA”/stroke/ peripheral Intent to Treat Primary result negative
 PFO Trials: What Went Wrong • The question implies we knew the answer – preconceived biases were not confirmed • Off label bias caused major recruitment problems – need to link device IND with RCT (eg stents) • Industry disappointed – NMT went bankrupt – St Jude FDA pending – market smaller than industry (and interventionalists) had hoped
PFO Trials: What Went Wrong • The question implies we knew the answer – preconceived biases were not confirmed • Off label bias caused major recruitment problems – need to link device IND with RCT (eg stents) • Industry disappointed – NMT went bankrupt – St Jude FDA pending – market smaller than industry (and interventionalists) had hoped
 PFO Trials: What Went Wrong • Any benefit of device likely small – device specific (thrombus, erosion, afib, residual shunt) – subgroup specific – long followup required – difficult (? impossible) to power a single trial • Best medical therapy is unknown – may be subgroup specific like device – antiplatelet versus antithrombotic • role of new antithrombotics unknown
PFO Trials: What Went Wrong • Any benefit of device likely small – device specific (thrombus, erosion, afib, residual shunt) – subgroup specific – long followup required – difficult (? impossible) to power a single trial • Best medical therapy is unknown – may be subgroup specific like device – antiplatelet versus antithrombotic • role of new antithrombotics unknown
 PFO Trials: What Went Wrong • What endpoint? – only CLOSURE included classic TIA endpoint • well defined TIA versus ill defined spell – but all 3 trials included imaging positive “TIA” • early MR not routine for TIA • Evaluation of cryptogenic stroke not standardized – cortical v subcortical infarcts – “hypercoagulopathy” – atrial fibrillation
PFO Trials: What Went Wrong • What endpoint? – only CLOSURE included classic TIA endpoint • well defined TIA versus ill defined spell – but all 3 trials included imaging positive “TIA” • early MR not routine for TIA • Evaluation of cryptogenic stroke not standardized – cortical v subcortical infarcts – “hypercoagulopathy” – atrial fibrillation
 PFO Trials: What Went Right • PFO coincidental in many patients with TIA or stroke – indiscriminate device closure halted – annual stroke risk is low – patient selection criteria being refined • PFO is more likely related in some patients compared to others • ROPE – evaluation of cryptogenic stroke being reassessed
PFO Trials: What Went Right • PFO coincidental in many patients with TIA or stroke – indiscriminate device closure halted – annual stroke risk is low – patient selection criteria being refined • PFO is more likely related in some patients compared to others • ROPE – evaluation of cryptogenic stroke being reassessed
 “The margin of potential benefit for PFO closure is narrow. ”
“The margin of potential benefit for PFO closure is narrow. ”
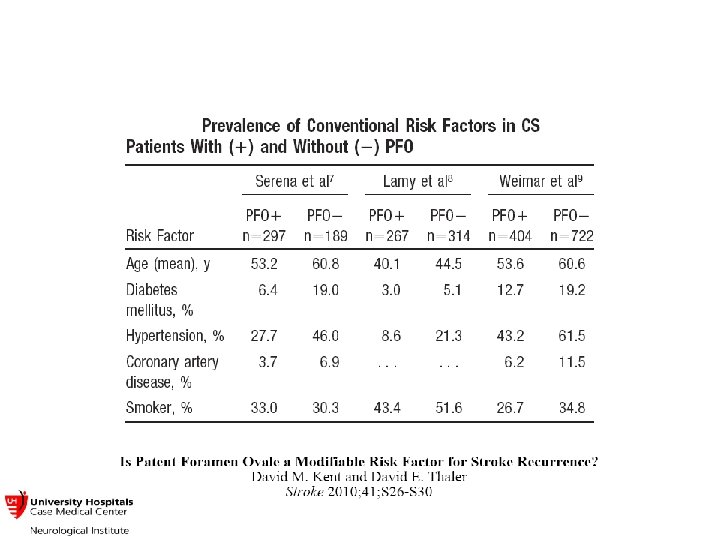
 Score Kent D etal") 6 single subcortical lacune Risk of Paradoxical Embolism (Ro. PE) Score Kent D etal Stroke. 2012; 43: A 84 Variables negatively associated with the presence of a PFO included: age (odds ratio [OR] = 0. 97 per 1 year increase, p <0. 0001); diabetes (OR= 0. 65, p < 0. 001); hypertension (OR =0. 68, p < 0. 0001); smoking (OR = 0. 70, p<0. 60); prior stroke or TIA (OR = 0. 78, p=0. 04). Cortical stroke on neuroimaging (OR = 1. 46, p < 0. 001) was also associated with PFO. Based on this, a simple index was created in which the absence of each stroke risk factor was assigned a point, with age dichotomized at 50 years. PFO prevalence in each stratum is shown in the table for patients < age 60, i. e. the subset of patients likely to be considered for PFO closure trials.
6 single subcortical lacune Risk of Paradoxical Embolism (Ro. PE) Score Kent D etal Stroke. 2012; 43: A 84 Variables negatively associated with the presence of a PFO included: age (odds ratio [OR] = 0. 97 per 1 year increase, p <0. 0001); diabetes (OR= 0. 65, p < 0. 001); hypertension (OR =0. 68, p < 0. 0001); smoking (OR = 0. 70, p<0. 60); prior stroke or TIA (OR = 0. 78, p=0. 04). Cortical stroke on neuroimaging (OR = 1. 46, p < 0. 001) was also associated with PFO. Based on this, a simple index was created in which the absence of each stroke risk factor was assigned a point, with age dichotomized at 50 years. PFO prevalence in each stratum is shown in the table for patients < age 60, i. e. the subset of patients likely to be considered for PFO closure trials.