

98500e118325c4ee8dbb07b383c0c412.ppt
- Количество слайдов: 32
 CRT 2010 Imaging Requirements and Interpretation in Acute Stroke Allan L. Brook, M. D. Director, Interventional Neuroradiology Montefiore Medical Center Associate Professor of Clinical Radiology and Neurosurgery Albert Einstein College of Medicine
CRT 2010 Imaging Requirements and Interpretation in Acute Stroke Allan L. Brook, M. D. Director, Interventional Neuroradiology Montefiore Medical Center Associate Professor of Clinical Radiology and Neurosurgery Albert Einstein College of Medicine
 DISCLOSURES Allan L. Brook, MD I have no real or apparent conflicts of interest to report.
DISCLOSURES Allan L. Brook, MD I have no real or apparent conflicts of interest to report.
 Stroke Facts • Stroke is a leading cause of death and disability worldwide with far reaching consequences for society • Burden of stroke is high and is likely to increase in future decades as a result of demographic and epidemiological transitions in populations Feigin et al. , Lancet Neurology 2003; 2: 43– 53
Stroke Facts • Stroke is a leading cause of death and disability worldwide with far reaching consequences for society • Burden of stroke is high and is likely to increase in future decades as a result of demographic and epidemiological transitions in populations Feigin et al. , Lancet Neurology 2003; 2: 43– 53
 Origins
Origins
 Imaging of Acute Stroke Overview Practical Theory • CTA/CTP • What are the goals of imaging? • MRI • MRA • DWI & perfusion imaging • DSA • Complimentary modalities …. not exclusive
Imaging of Acute Stroke Overview Practical Theory • CTA/CTP • What are the goals of imaging? • MRI • MRA • DWI & perfusion imaging • DSA • Complimentary modalities …. not exclusive
 Imaging Goals • To exclude pathology that needs acute intervention • Localize • • Acute hemorrhage Tumor Infection Herniation syndromes
Imaging Goals • To exclude pathology that needs acute intervention • Localize • • Acute hemorrhage Tumor Infection Herniation syndromes
 on CT • Can predict both functional outcome and") Importance of Early Ischemic Changes(EIC) on CT • Can predict both functional outcome and the risk of cerebral hemorrhage AJNR: 22, September 2001
Importance of Early Ischemic Changes(EIC) on CT • Can predict both functional outcome and the risk of cerebral hemorrhage AJNR: 22, September 2001
 Dense MCA Sign • Clot vs calcium • Predictor of large vessel occlusion Srinivasan et al October 2006 Radio. Graphics, 26, S 75 -S 9
Dense MCA Sign • Clot vs calcium • Predictor of large vessel occlusion Srinivasan et al October 2006 Radio. Graphics, 26, S 75 -S 9
 Basics: CT of Acute Stroke • Evaluating earliest subtle findings to severe & chronic changes Posterior putamen Loss of gw distinction Srinivasan et al October 2006 Radio. Graphics, 26, S 75 -S 9
Basics: CT of Acute Stroke • Evaluating earliest subtle findings to severe & chronic changes Posterior putamen Loss of gw distinction Srinivasan et al October 2006 Radio. Graphics, 26, S 75 -S 9
 Spectrum • Dense MCA sign- M 1 or distal M 2 • Subtle loss of grey white distinction in basal ganglia, perisylvian, or cortical edema
Spectrum • Dense MCA sign- M 1 or distal M 2 • Subtle loss of grey white distinction in basal ganglia, perisylvian, or cortical edema
 CTA
CTA
 False Positive • 52 -year-old man with a history of patent foramen ovale presented with diplopia, a left facial droop, and mild left-side weakness CTA helps exclude clot • Small infarct in the medial right thalamus on MRI
False Positive • 52 -year-old man with a history of patent foramen ovale presented with diplopia, a left facial droop, and mild left-side weakness CTA helps exclude clot • Small infarct in the medial right thalamus on MRI
 MCA Territory & Safety for Revascularization? Less than 1/3 rd Greater than 1/3 rd Gadda et al. , Eur Radiol (2005) 15: 2387– 2395
MCA Territory & Safety for Revascularization? Less than 1/3 rd Greater than 1/3 rd Gadda et al. , Eur Radiol (2005) 15: 2387– 2395
 33% vs 50% ? ? ? • MCA territory regions according to ASPECTS • • • Alberta Stroke Program Early CT Score MCA territory is allotted 10 points, each territory corresponding to a region One point is subtracted for any infarcted area A score of 10 points means no ischemic areas 0 points that the whole MCA territory is affected A sharp increase in dependence and death occurs with an ASPECTS of 7 or less AJNR: 22, September 2001
33% vs 50% ? ? ? • MCA territory regions according to ASPECTS • • • Alberta Stroke Program Early CT Score MCA territory is allotted 10 points, each territory corresponding to a region One point is subtracted for any infarcted area A score of 10 points means no ischemic areas 0 points that the whole MCA territory is affected A sharp increase in dependence and death occurs with an ASPECTS of 7 or less AJNR: 22, September 2001
 MRI & Acute Stroke Imaging Exclude Mimics & Hem! • • • T 1 W, T 2 W FLAIR DWI FFE Gd enhancement Perfusion Slow flow Cortical edema AJR: 179, July 2002
MRI & Acute Stroke Imaging Exclude Mimics & Hem! • • • T 1 W, T 2 W FLAIR DWI FFE Gd enhancement Perfusion Slow flow Cortical edema AJR: 179, July 2002
 Enhancement MRI Stroke • Hyperacute • Acute • Subacute and chronic • Intravascular-hours • Meningeal-1 -3 days • Parenchymal->3 days MRA
Enhancement MRI Stroke • Hyperacute • Acute • Subacute and chronic • Intravascular-hours • Meningeal-1 -3 days • Parenchymal->3 days MRA
 DWI Has Revolutionized Imaging of Acute Stroke • Is The Gold Standard … seen in black and white DWI ADC
DWI Has Revolutionized Imaging of Acute Stroke • Is The Gold Standard … seen in black and white DWI ADC
 MRI with diffusion weighted imaging Isolated weakness right index finger JS Kim, Neurology, 2002
MRI with diffusion weighted imaging Isolated weakness right index finger JS Kim, Neurology, 2002
 Where is the stroke?
Where is the stroke?
 Natural history ~ 7 Hour F/U Small DWI lesion in deep MCA terrirtory with extensive area of prolonged time to peak (ie, mismatch) M 1 occlusion 1 -Hour 7 -Hour F/U Neurology thelancet Vol 5 September 2006
Natural history ~ 7 Hour F/U Small DWI lesion in deep MCA terrirtory with extensive area of prolonged time to peak (ie, mismatch) M 1 occlusion 1 -Hour 7 -Hour F/U Neurology thelancet Vol 5 September 2006
 The Crux • Recanalization does not always produce good clinical outcome • Imaging can be achieved in reasonable time • Patient selection by imaging will hopefully identify those who will benefit from early reperfusion • Limit risk by proper stratification
The Crux • Recanalization does not always produce good clinical outcome • Imaging can be achieved in reasonable time • Patient selection by imaging will hopefully identify those who will benefit from early reperfusion • Limit risk by proper stratification
 The DEFUSE Study • Identified a “target mismatch” profile based on MRI • Patients had a robust clinical response after early reperfusion Stroke. 2007; 38: 1826 -1830 Ann. Neurol. 2006; 60: 508 – 517
The DEFUSE Study • Identified a “target mismatch” profile based on MRI • Patients had a robust clinical response after early reperfusion Stroke. 2007; 38: 1826 -1830 Ann. Neurol. 2006; 60: 508 – 517
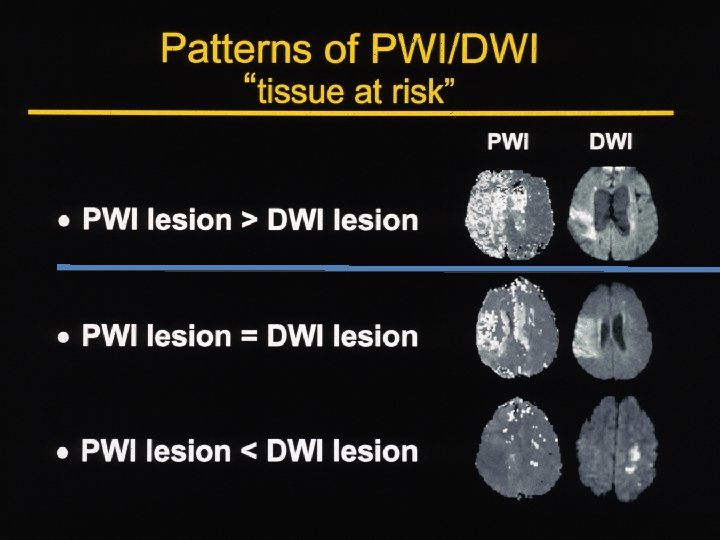
 Mismatch/Penumbra Core Irreversibly injured tissue Penumbra At risk, but salvageable, if reperfusion occurs Benign Oligemia Decreased flow but not at risk of infarction m. L/100 g/min Neurology thelancet Vol 5 September 2006
Mismatch/Penumbra Core Irreversibly injured tissue Penumbra At risk, but salvageable, if reperfusion occurs Benign Oligemia Decreased flow but not at risk of infarction m. L/100 g/min Neurology thelancet Vol 5 September 2006
 Zones of Ischemia Imaging-Guided Acute Ischemic Stroke Therapy: From "Time Is Brain" to "Physiology Is Brain" R. G. Gonzáleza AJNR 27: 728 -736 c/o Kristine Blackham MD
Zones of Ischemia Imaging-Guided Acute Ischemic Stroke Therapy: From "Time Is Brain" to "Physiology Is Brain" R. G. Gonzáleza AJNR 27: 728 -736 c/o Kristine Blackham MD
 Imaging Modalities used to Identify The Ischemic Penumbra and Core • • • CTPerfusion CT-Xe MR-DWI/PWI MR-Spectroscopy PET- 15 O 2 SPECT-TC-HMPAO CBF, CBV, MTT, TTP, ADC NAA, Lactate CBF, CBV, MTT, CMRO 2, OEF • CBF • • • Positron emission tomography (PET) has bee particularly instrumental in these developments and continues to be the gold standard in stroke imaging CTP & MRP Correlation with PET is far from perfect!!!!!!!
Imaging Modalities used to Identify The Ischemic Penumbra and Core • • • CTPerfusion CT-Xe MR-DWI/PWI MR-Spectroscopy PET- 15 O 2 SPECT-TC-HMPAO CBF, CBV, MTT, TTP, ADC NAA, Lactate CBF, CBV, MTT, CMRO 2, OEF • CBF • • • Positron emission tomography (PET) has bee particularly instrumental in these developments and continues to be the gold standard in stroke imaging CTP & MRP Correlation with PET is far from perfect!!!!!!!
 When Exact time is unknown Can we utilize imaging to triage? • 38 -year-old man who was found with a severe left hemiparesis Pt wakes up with deficit Gonzalez AJNR 27 Apr 2006
When Exact time is unknown Can we utilize imaging to triage? • 38 -year-old man who was found with a severe left hemiparesis Pt wakes up with deficit Gonzalez AJNR 27 Apr 2006
 Neuro. Imaging Goals • Findings from a physical examination and patient history cannot always help determine diagnosis (accurate time and anatomic localization) • Decipher & triage quickly which patients have the option of medical or interventional recanalization
Neuro. Imaging Goals • Findings from a physical examination and patient history cannot always help determine diagnosis (accurate time and anatomic localization) • Decipher & triage quickly which patients have the option of medical or interventional recanalization
 Comparison of CT and MR Perfusion l MR: l l Whole head Conspicuous lacunar infarcts on diffusion Use TTP primarily l CT l l l Relative values only Ostensibly better quantification Closer to ER Limited FOV by detector thickness l l Distal, posterior fossa or watershed infarcts Radiation! Both can function well-------utilize what is available and best in your institute!
Comparison of CT and MR Perfusion l MR: l l Whole head Conspicuous lacunar infarcts on diffusion Use TTP primarily l CT l l l Relative values only Ostensibly better quantification Closer to ER Limited FOV by detector thickness l l Distal, posterior fossa or watershed infarcts Radiation! Both can function well-------utilize what is available and best in your institute!
 Conclusion • Diagnostic imaging in acute stroke is a prerequisite for successful acute stroke therapy (IV & IA) • The severity of the early ischemic edema has prognostic relevance for hemorrhagic complications after thrombolysis
Conclusion • Diagnostic imaging in acute stroke is a prerequisite for successful acute stroke therapy (IV & IA) • The severity of the early ischemic edema has prognostic relevance for hemorrhagic complications after thrombolysis
 Conclusion • Structural, vascular, and physiological imaging of acute stroke continue to be studied in clinical trials • It is likely that both CT and MRI-based techniques will be more widely applied in future, & should be regarded as complementary rather than competing • This is the Genesis in Acute Stroke Therapy not the end!
Conclusion • Structural, vascular, and physiological imaging of acute stroke continue to be studied in clinical trials • It is likely that both CT and MRI-based techniques will be more widely applied in future, & should be regarded as complementary rather than competing • This is the Genesis in Acute Stroke Therapy not the end!
 Thank You
Thank You