

9ebaeb3555cba60dce2f09fc74587c4b.ppt
- Количество слайдов: 37
 Creating Partnerships and Navigating the ‘Culture of Corrections’ November 19, 2013
Creating Partnerships and Navigating the ‘Culture of Corrections’ November 19, 2013
 project n Sarah Cook-Raymond,") Agenda n Introduction to SPNS Integrating HIV Innovative Practices (IHIP) project n Sarah Cook-Raymond, Impact Marketing + Communications n Presentations n Hannah from Zellman, Philadelphia FIGHT n Dr. Linda Rose Frank, PA/Mid. Atlantic AETC n Debra D’Alessandro, PA/Mid. Atlantic AETC n. Q &A
Agenda n Introduction to SPNS Integrating HIV Innovative Practices (IHIP) project n Sarah Cook-Raymond, Impact Marketing + Communications n Presentations n Hannah from Zellman, Philadelphia FIGHT n Dr. Linda Rose Frank, PA/Mid. Atlantic AETC n Debra D’Alessandro, PA/Mid. Atlantic AETC n. Q &A
 IHIP Resources on TARGET Center Website www. careacttarget. org/ihip
IHIP Resources on TARGET Center Website www. careacttarget. org/ihip
 IHIP Jail Linkage Resources: n Lessons Learned Manual n Implementation Guide n Webinar Series n n n HIV and Jails: A Public Health Opportunity –archive available at careacttarget/org/ihip How to Build and Expand a Jail Linkage Program – archive available at careacttarget/org/ihip Creating Partnerships and Navigating the “Culture of Corrections”- November 19, 2013 at 1: 30 pm ET www. careacttarget. org/ihip
IHIP Jail Linkage Resources: n Lessons Learned Manual n Implementation Guide n Webinar Series n n n HIV and Jails: A Public Health Opportunity –archive available at careacttarget/org/ihip How to Build and Expand a Jail Linkage Program – archive available at careacttarget/org/ihip Creating Partnerships and Navigating the “Culture of Corrections”- November 19, 2013 at 1: 30 pm ET www. careacttarget. org/ihip
 Other IHIP Resources n Buprenorphine n Training Manual, Curricula, and Webinars on Implementing Buprenorphine into Primary Care Settings n Engaging Hard-to-Reach Populations n n Training Manual, Curricula, and Webinars on Engaging Hard-to-Reach Populations Oral Health n Forthcoming: Training Manual and Curricula available in December and Webinar series on Oral Health and HIV begins December 13, 2013 at 1 pm ET
Other IHIP Resources n Buprenorphine n Training Manual, Curricula, and Webinars on Implementing Buprenorphine into Primary Care Settings n Engaging Hard-to-Reach Populations n n Training Manual, Curricula, and Webinars on Engaging Hard-to-Reach Populations Oral Health n Forthcoming: Training Manual and Curricula available in December and Webinar series on Oral Health and HIV begins December 13, 2013 at 1 pm ET
 Lessons Learned from a Jail Based HIV Linkage Program Hannah Zellman, MSW Director, Philadelphia FIGHT’s Institute for Community Justice
Lessons Learned from a Jail Based HIV Linkage Program Hannah Zellman, MSW Director, Philadelphia FIGHT’s Institute for Community Justice
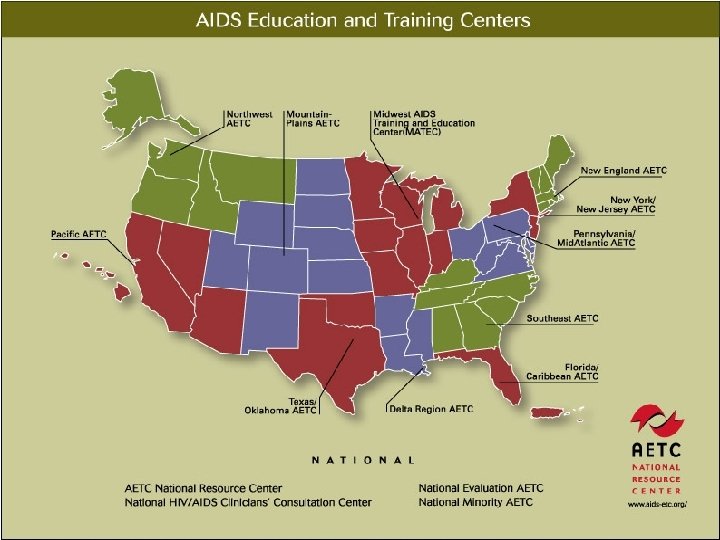
 Enhancing Linkages to HIV Primary Care and Services in Jail Enhancing Linkages was a multisite demonstration and evaluation of HIV service delivery interventions for HIV+ individuals in jail settings who are returning to their communities. The Enhancing Linkages Initiative is sponsored by: US Department of Health and Human Services Health Resources and Services Administration HIV/AIDS Bureau Special Projects of National Significance
Enhancing Linkages to HIV Primary Care and Services in Jail Enhancing Linkages was a multisite demonstration and evaluation of HIV service delivery interventions for HIV+ individuals in jail settings who are returning to their communities. The Enhancing Linkages Initiative is sponsored by: US Department of Health and Human Services Health Resources and Services Administration HIV/AIDS Bureau Special Projects of National Significance
 Overview of our SPNS Project Implemented within our county jail system, the Philadelphia Prison System (PPS) Approximately 40, 000 admissions per year Average daily census between 7, 000 and 8, 000 3% of male prisoners are living with HIV 6% of female prisoners are living with HIV Systems level intervention to strengthen HIV continuity of care and collaboration amongst service providers, including a collaborative multi-disciplinary team approach Establishment of a single point of contact system for referrals Strengthened continuum of care services Utilize official visits, court advocacy, peer leadership models, treatment education Expedited medical linkages upon release Partnership among leading AIDS Service Providers
Overview of our SPNS Project Implemented within our county jail system, the Philadelphia Prison System (PPS) Approximately 40, 000 admissions per year Average daily census between 7, 000 and 8, 000 3% of male prisoners are living with HIV 6% of female prisoners are living with HIV Systems level intervention to strengthen HIV continuity of care and collaboration amongst service providers, including a collaborative multi-disciplinary team approach Establishment of a single point of contact system for referrals Strengthened continuum of care services Utilize official visits, court advocacy, peer leadership models, treatment education Expedited medical linkages upon release Partnership among leading AIDS Service Providers
 Successes of the program Successfully implemented SPOC and fostered trusting relationship amongst service providers Served 342 people over the course of the program Linkage to care for initial appointment 73% Retained in care after 3 visits 88% Increased visibility in the jails and reentry community allowed for program expansion
Successes of the program Successfully implemented SPOC and fostered trusting relationship amongst service providers Served 342 people over the course of the program Linkage to care for initial appointment 73% Retained in care after 3 visits 88% Increased visibility in the jails and reentry community allowed for program expansion
 Collaboration is key Criminal justice system stakeholders Allows us to extend the support network of the client by engaging, with client consent, with prison staff, parole and probation and the courts It’s all about access! Establishing formal mechanisms for communication Avoids confusion and misunderstandings Education for staff Prison staff have decision making power that can affect an individuals’ situation There are opportunities to diffuse best practices amongst staff which will, in turn, benefit the treatment and wellbeing of the client
Collaboration is key Criminal justice system stakeholders Allows us to extend the support network of the client by engaging, with client consent, with prison staff, parole and probation and the courts It’s all about access! Establishing formal mechanisms for communication Avoids confusion and misunderstandings Education for staff Prison staff have decision making power that can affect an individuals’ situation There are opportunities to diffuse best practices amongst staff which will, in turn, benefit the treatment and wellbeing of the client
 Getting inside Jail/prison systems might ask: “What’s in it for us? " Emphasize that this is often a low or no cost to the prison/jail system Use compelling arguments! Point out that community providers and jails share the same goals In-reach and community follow up has the potential to reduce recidivism Controlling the virus is not only cost saving in the community, but can also be potentially cost saving for prisons, since it might reduce urgent or emergency care needs, hospitalizations, etc
Getting inside Jail/prison systems might ask: “What’s in it for us? " Emphasize that this is often a low or no cost to the prison/jail system Use compelling arguments! Point out that community providers and jails share the same goals In-reach and community follow up has the potential to reduce recidivism Controlling the virus is not only cost saving in the community, but can also be potentially cost saving for prisons, since it might reduce urgent or emergency care needs, hospitalizations, etc
 The Culture of Corrections Chain of command Goals of corrections are security, control, safety This can be challenging, but isn’t insurmountable Often, you are a guest in the system You may have limited access to technology You have limited decision making power Remember it’s a jail! It can be jarring to be searched, to be locked in, and to otherwise adjust to a jail based setting if you’re accustomed to a community based setting
The Culture of Corrections Chain of command Goals of corrections are security, control, safety This can be challenging, but isn’t insurmountable Often, you are a guest in the system You may have limited access to technology You have limited decision making power Remember it’s a jail! It can be jarring to be searched, to be locked in, and to otherwise adjust to a jail based setting if you’re accustomed to a community based setting
 In Reach Experience has shown us that linkage programs are more successful with an inside-outside approach. Builds long term trust Allows for monitoring of medical care on the inside for increased continuity upon release Increases the likelihood that someone will present after release At it’s most basic level, this approach allows service providers to walk with the client through their entire interaction with the criminal justice system
In Reach Experience has shown us that linkage programs are more successful with an inside-outside approach. Builds long term trust Allows for monitoring of medical care on the inside for increased continuity upon release Increases the likelihood that someone will present after release At it’s most basic level, this approach allows service providers to walk with the client through their entire interaction with the criminal justice system
 Collaboration and continuity of care Relationships with jail medical staff are essential – continuity relies on communication and collaboration Medication – corrections settings have different standards for medications upon discharge Leave with a 30 day supply Leave with the remainder of your current meds Leave with an Rx Insurance Prisons vs. Jails
Collaboration and continuity of care Relationships with jail medical staff are essential – continuity relies on communication and collaboration Medication – corrections settings have different standards for medications upon discharge Leave with a 30 day supply Leave with the remainder of your current meds Leave with an Rx Insurance Prisons vs. Jails
 Follow up and retention The period of time following release is one of increased vulnerability. Best practices can include: Expedited medical appointments Incentives Inside-out staffing/familiar advocates One stop shopping models Multiple ways to contact Thorough assessment of vulnerabilities and triggers Be flexible and open to new, innovative strategies to meet people where they’re at and support them in making their healthcare a priority.
Follow up and retention The period of time following release is one of increased vulnerability. Best practices can include: Expedited medical appointments Incentives Inside-out staffing/familiar advocates One stop shopping models Multiple ways to contact Thorough assessment of vulnerabilities and triggers Be flexible and open to new, innovative strategies to meet people where they’re at and support them in making their healthcare a priority.
 Successful Linkage – Varying Definitions There were variations across SPNS demonstration sites Consistent with the HRSA definition - three medical visits in a 12 month period of time One medical visit within 30 days of release, or within 90 days of release Milestones in service linkage and stability in the community
Successful Linkage – Varying Definitions There were variations across SPNS demonstration sites Consistent with the HRSA definition - three medical visits in a 12 month period of time One medical visit within 30 days of release, or within 90 days of release Milestones in service linkage and stability in the community
 Know the population Redefining “success” Developing a trusting relationship with providers so that linkage is maintained in spite of repeated interruptions due to re-incarceration. Employing harm reduction strategies that support individuals in active addiction to keep them in care and use creative strategies to support adherence. Building flexibility into the program to ensure that we’re meeting participants where they’re at.
Know the population Redefining “success” Developing a trusting relationship with providers so that linkage is maintained in spite of repeated interruptions due to re-incarceration. Employing harm reduction strategies that support individuals in active addiction to keep them in care and use creative strategies to support adherence. Building flexibility into the program to ensure that we’re meeting participants where they’re at.
 Best practices One stop shopping model/ Medical Home Model Multidisciplinary team of jail and community providers characterized by increased communication and formalized structures Capitalizing on the strength and power of peer leadership and mutual support Knowing that the intersection of the parallel crises of HIV and mass imprisonment is a critical juncture – we need to work at this intersection to end the epidemic Understanding that what people need first is safe space
Best practices One stop shopping model/ Medical Home Model Multidisciplinary team of jail and community providers characterized by increased communication and formalized structures Capitalizing on the strength and power of peer leadership and mutual support Knowing that the intersection of the parallel crises of HIV and mass imprisonment is a critical juncture – we need to work at this intersection to end the epidemic Understanding that what people need first is safe space
 Questions?
Questions?
 Jail Linkage: Creating Partnerships and Navigating the Culture of Corrections Dissemination of SPNS Best Practices Linda Rose Frank, Ph. D, MSN, ACRN, FAAN Associate Professor of Public Health, Graduate School of Public Health Associate Professor, Center for Translational Science Institute, School of Medicine Associate Professor, Community and Health Systems, School of Nursing University of Pittsburgh Principal Investigator and Executive Director Pennsylvania/Mid. Atlantic AIDS Education & Training Center and Telehealth AETC Appalachian Project
Jail Linkage: Creating Partnerships and Navigating the Culture of Corrections Dissemination of SPNS Best Practices Linda Rose Frank, Ph. D, MSN, ACRN, FAAN Associate Professor of Public Health, Graduate School of Public Health Associate Professor, Center for Translational Science Institute, School of Medicine Associate Professor, Community and Health Systems, School of Nursing University of Pittsburgh Principal Investigator and Executive Director Pennsylvania/Mid. Atlantic AIDS Education & Training Center and Telehealth AETC Appalachian Project
 pamaaetc. org 21
pamaaetc. org 21
 Domestic Violence Substance Use, Mental illness HIV/AIDS Homelessness Incarceration Copyright: Linda Frank, Ph. D, MSN, ACRN, FAAN, University of Pittsburgh, 2005
Domestic Violence Substance Use, Mental illness HIV/AIDS Homelessness Incarceration Copyright: Linda Frank, Ph. D, MSN, ACRN, FAAN, University of Pittsburgh, 2005
 Pennsylvania/Mid. Atlantic AETC Jail and Prison Intervention since 1990 n Training of prison and jail q q n Peer-based HIV education for inmates q n q q HIV-related policies and procedures HIV testing and prevention HIV treatment Telemedicine consultation with prisons and jails q q n Statewide in PA Technical assistance to prisons and jails: q n administration and leadership physicians, nurses, counselors, and clergy corrections officers probation and parole personnel HIV treatment Treatment of co-morbidities On-site consultation to prisons and jails
Pennsylvania/Mid. Atlantic AETC Jail and Prison Intervention since 1990 n Training of prison and jail q q n Peer-based HIV education for inmates q n q q HIV-related policies and procedures HIV testing and prevention HIV treatment Telemedicine consultation with prisons and jails q q n Statewide in PA Technical assistance to prisons and jails: q n administration and leadership physicians, nurses, counselors, and clergy corrections officers probation and parole personnel HIV treatment Treatment of co-morbidities On-site consultation to prisons and jails
 Pennsylvania/Mid. Atlantic AETC Prison/Jail Related Work n n n APHA Jail and Prison Health Committee State-related committees, forums on corrections Local jail, prison committees National and international presentations Testimony for legislators, policy forums, etc.
Pennsylvania/Mid. Atlantic AETC Prison/Jail Related Work n n n APHA Jail and Prison Health Committee State-related committees, forums on corrections Local jail, prison committees National and international presentations Testimony for legislators, policy forums, etc.
 Approach to Dissemination n Convene PA/MA AETC team to review materials q n Reviewed materials with HRSA SPNS and HRSA AETC leadership q q n n included PA/MA AETC representatives from Philadelphia, Pittsburgh, DC, West Virginia, Ohio, Maryland Direction Scope of work Developed methods for dissemination which may include: q Development of print and electronic pocket guide on best practices q Related slide sets for training Posting of materials developed on q q q AETC National Resource Center (NRC) website Regional AETC websites HRSA Target Center website
Approach to Dissemination n Convene PA/MA AETC team to review materials q n Reviewed materials with HRSA SPNS and HRSA AETC leadership q q n n included PA/MA AETC representatives from Philadelphia, Pittsburgh, DC, West Virginia, Ohio, Maryland Direction Scope of work Developed methods for dissemination which may include: q Development of print and electronic pocket guide on best practices q Related slide sets for training Posting of materials developed on q q q AETC National Resource Center (NRC) website Regional AETC websites HRSA Target Center website
 Debra D’Alessandro, MPH Public Health Program Manager, Health Federation of Philadelphia, Local Performance Site Pennsylvania/Mid. Atlantic AETC
Debra D’Alessandro, MPH Public Health Program Manager, Health Federation of Philadelphia, Local Performance Site Pennsylvania/Mid. Atlantic AETC
 Pennsylvania/Mid. Atlantic AETCs Ongoing technical assistance with Philadelphia Prisons: before, during & after SPNS n n Since 2000, bringing onsite CME accredited lunchtime clinical updates for correctional health providers Since 2007, convening HIV Discharge Planning Committee – Phila. Dept of Public Health (AACO), behavioral and physical health contractors, prison admin, two ASOs w/onsite case managers (Action. AIDS & Phila FIGHT)
Pennsylvania/Mid. Atlantic AETCs Ongoing technical assistance with Philadelphia Prisons: before, during & after SPNS n n Since 2000, bringing onsite CME accredited lunchtime clinical updates for correctional health providers Since 2007, convening HIV Discharge Planning Committee – Phila. Dept of Public Health (AACO), behavioral and physical health contractors, prison admin, two ASOs w/onsite case managers (Action. AIDS & Phila FIGHT)
 Pennsylvania/Mid. Atlantic AETC activity in Phila. Prison System since 2000 n Onsite training of correctional health staff, 3 -6 times a year: q q q n When needed, training for non-medical prison audience: q q n TB and occupational post-exposure prophylaxis education for CO supervisors Women’s health series, taught by community NPs, for female inmates Technical assistance: q q n Annual needs assessment with administration and leadership Physicians, nurses, PAs, MAs target, admin & others invited Accredited lunchtime sessions on HIV issues, co-morbidities and other public health topics (STDs, TB, MRSA and other skin infections) Opt-out HIV testing at intake – policy development, pilot, training Consultation regarding keep-on-person policy for HIV meds Since 2007, bi-monthly HIV Prison Discharge Planning Meetings
Pennsylvania/Mid. Atlantic AETC activity in Phila. Prison System since 2000 n Onsite training of correctional health staff, 3 -6 times a year: q q q n When needed, training for non-medical prison audience: q q n TB and occupational post-exposure prophylaxis education for CO supervisors Women’s health series, taught by community NPs, for female inmates Technical assistance: q q n Annual needs assessment with administration and leadership Physicians, nurses, PAs, MAs target, admin & others invited Accredited lunchtime sessions on HIV issues, co-morbidities and other public health topics (STDs, TB, MRSA and other skin infections) Opt-out HIV testing at intake – policy development, pilot, training Consultation regarding keep-on-person policy for HIV meds Since 2007, bi-monthly HIV Prison Discharge Planning Meetings
 Lessons Learned from Philadelphia HIV Discharge Planning Committee n Face-to-face, multi-disciplinary case discussions can speed problem solving q q n Regular review of policy vs. practice can reveal need for procedure adjustments and ongoing training q q n M&M (morbidity and mortality) Reviewed cases when releasees NOT connected to care as missed opportunities what could be different next time Recent Example: medication upon discharge changes Opt-out testing at intake Referral to linkage staff for new or out-of-care positives Staff turnover means work is never “once and done” q Administrative and clinical staff changes can lead to confusion and/or apathy about testing and referral
Lessons Learned from Philadelphia HIV Discharge Planning Committee n Face-to-face, multi-disciplinary case discussions can speed problem solving q q n Regular review of policy vs. practice can reveal need for procedure adjustments and ongoing training q q n M&M (morbidity and mortality) Reviewed cases when releasees NOT connected to care as missed opportunities what could be different next time Recent Example: medication upon discharge changes Opt-out testing at intake Referral to linkage staff for new or out-of-care positives Staff turnover means work is never “once and done” q Administrative and clinical staff changes can lead to confusion and/or apathy about testing and referral
 Working in the Jail: Initial Questions to Consider n n n What is the jail’s view of HIV in comparison to other chronic health issues? Determine the composition of jail health professionals: how many, and what disciplines? How can you be “value added? ” How do inmates request health & social services? How can you fit into this process?
Working in the Jail: Initial Questions to Consider n n n What is the jail’s view of HIV in comparison to other chronic health issues? Determine the composition of jail health professionals: how many, and what disciplines? How can you be “value added? ” How do inmates request health & social services? How can you fit into this process?
 More Lessons from Enhance. Link grantees: n n Relationship building takes time. Account for this in your timeline and rollout of your program. Know what services you hope to refer inmates to upon release, and create partnerships with those organizations. Memoranda of Understanding are just the beginning. There needs to be follow-through. (“MOUs are paper, not partnerships. ”) n
More Lessons from Enhance. Link grantees: n n Relationship building takes time. Account for this in your timeline and rollout of your program. Know what services you hope to refer inmates to upon release, and create partnerships with those organizations. Memoranda of Understanding are just the beginning. There needs to be follow-through. (“MOUs are paper, not partnerships. ”) n
 Lessons from Enhance. Link grantees, cont… n n n Do your homework. Know what services are in the jail and who is delivering them. How can you fill in service gaps? Listen and learn. Organizations already in the jail know how to work in this setting without interfering with Dept. Corrections operations and protocols. Be on everyone’s radar. To avoid “turf wars, ” embrace transparency.
Lessons from Enhance. Link grantees, cont… n n n Do your homework. Know what services are in the jail and who is delivering them. How can you fill in service gaps? Listen and learn. Organizations already in the jail know how to work in this setting without interfering with Dept. Corrections operations and protocols. Be on everyone’s radar. To avoid “turf wars, ” embrace transparency.
 Questions?
Questions?
 Q&A To be informed when these upcoming IHIP resources are ready, sign up for the IHIP listserv by emailing scook@impactmc. net. Connect with Us Sarah Cook-Raymond, Managing Director |Impact Marketing + Communications | Twitter: @impactmc 1| Facebook: Impact. Mar. Com |www. impactmc. net | 202 -588 -0300
Q&A To be informed when these upcoming IHIP resources are ready, sign up for the IHIP listserv by emailing scook@impactmc. net. Connect with Us Sarah Cook-Raymond, Managing Director |Impact Marketing + Communications | Twitter: @impactmc 1| Facebook: Impact. Mar. Com |www. impactmc. net | 202 -588 -0300