

541e05ef0936cbb6d8c5e43525101e3c.ppt
- Количество слайдов: 26
 Ivor") CPOE in Critical Care Andy Steele, MD, MPH (Director, Medical Informatics, Denver Health) Ivor Douglas, MD, (Director, MICU, Denver Health) AHRQ Patient Safety Conference June 6 th, 2005
CPOE in Critical Care Andy Steele, MD, MPH (Director, Medical Informatics, Denver Health) Ivor Douglas, MD, (Director, MICU, Denver Health) AHRQ Patient Safety Conference June 6 th, 2005
 Outline • • WHY CPOE? CPOE in the Critical Care Unit MICU CPOE Lessons Learned Questions
Outline • • WHY CPOE? CPOE in the Critical Care Unit MICU CPOE Lessons Learned Questions
 - WHY? • Improved Patient Care – Patient Safety") Computerized Provider Order Entry (CPOE) - WHY? • Improved Patient Care – Patient Safety (medication errors) – Improved Efficiency and Quality of Care • • Support of Compliance Efforts Support of Provider Billing Activities External Forces: Payers-Leapfrog, Legislation Marketing Advantage
Computerized Provider Order Entry (CPOE) - WHY? • Improved Patient Care – Patient Safety (medication errors) – Improved Efficiency and Quality of Care • • Support of Compliance Efforts Support of Provider Billing Activities External Forces: Payers-Leapfrog, Legislation Marketing Advantage
 Critical Care Impact on Health Care Resources • 15 -20% of health care expenditures (1. 5% GNP) • 10 -25% of all hospital beds and increasing • Postoperative management accounts for 65% of all ICU admissions. • ICU’s are usually money-losing operation due to “outliers” (10% patients account for 67% of costs) • Large shortage of “skilled” critical care providers
Critical Care Impact on Health Care Resources • 15 -20% of health care expenditures (1. 5% GNP) • 10 -25% of all hospital beds and increasing • Postoperative management accounts for 65% of all ICU admissions. • ICU’s are usually money-losing operation due to “outliers” (10% patients account for 67% of costs) • Large shortage of “skilled” critical care providers
 CPOE Benefits in Critical Care BWH Experience With CPOE Medication Error Rate (#/1, 000 patient days) JAMIA. 1999; 6: 313 -321
CPOE Benefits in Critical Care BWH Experience With CPOE Medication Error Rate (#/1, 000 patient days) JAMIA. 1999; 6: 313 -321
 CPOE Benefits in Critical Care BWH Experience With CPOE Medication Error Rate (#/1, 000 patient days) JAMIA. 1999; 6: 313 -321
CPOE Benefits in Critical Care BWH Experience With CPOE Medication Error Rate (#/1, 000 patient days) JAMIA. 1999; 6: 313 -321
 CPOE Benefits in Critical Care Improved Quality and Efficiency of Care – Lab collection - 77 down to 21. 5 min. – Radiology Exams - 96. 5 down to 29. 5 min. • Crit Care Med 2004; 32: 1306 – 1309 – NICU medication turn-around times- 10. 5 down to 2. 8 hours – Improved NICU accuracy of gentamicin dosing-12% over/under dosages decreased to 0% • Journal of Perinatology (2004) 24, 88– 93.
CPOE Benefits in Critical Care Improved Quality and Efficiency of Care – Lab collection - 77 down to 21. 5 min. – Radiology Exams - 96. 5 down to 29. 5 min. • Crit Care Med 2004; 32: 1306 – 1309 – NICU medication turn-around times- 10. 5 down to 2. 8 hours – Improved NICU accuracy of gentamicin dosing-12% over/under dosages decreased to 0% • Journal of Perinatology (2004) 24, 88– 93.
 Denver Health Clinical Statistics • 20, 000 admissions annually • 75% minority population • MICU-24 beds (Step-down Unit-8 beds) • 2, 000 Admissions annually • CPOE In Use For 23 months – ~500 providers/users trained – ~6, 000 orders input/week – ~30 standardized care order sets being used
Denver Health Clinical Statistics • 20, 000 admissions annually • 75% minority population • MICU-24 beds (Step-down Unit-8 beds) • 2, 000 Admissions annually • CPOE In Use For 23 months – ~500 providers/users trained – ~6, 000 orders input/week – ~30 standardized care order sets being used
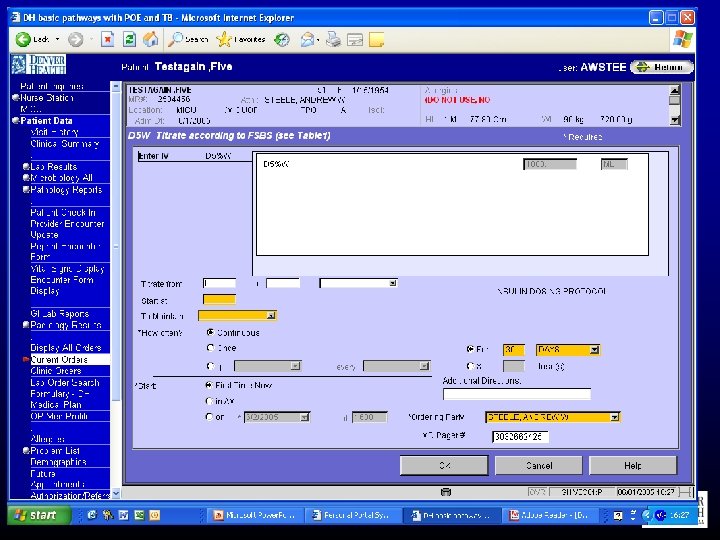
 CPOE/CDSS : Protocol Driven Aggressive Correction Of Diabetic Emergencies • Diabetic Emergencies – – Diabetic Ketoacidosis Hyperglycemic hyperosmolar syndrome 5 -18% of admission to MICU Aggressive “tight” blood sugar control in other critical illness (sepsis) reduced mortality • Principles of management – Multiple differing strategies, very little rigorous prospective evaluation • Correct metabolic abnormalities • Correct precipitant • Aggressive IV fluid resuscitation • Insulin, Potassium
CPOE/CDSS : Protocol Driven Aggressive Correction Of Diabetic Emergencies • Diabetic Emergencies – – Diabetic Ketoacidosis Hyperglycemic hyperosmolar syndrome 5 -18% of admission to MICU Aggressive “tight” blood sugar control in other critical illness (sepsis) reduced mortality • Principles of management – Multiple differing strategies, very little rigorous prospective evaluation • Correct metabolic abnormalities • Correct precipitant • Aggressive IV fluid resuscitation • Insulin, Potassium









 Post CPOE (N=111) P 39. 9± 1.") CPOE Driven DKA/HHS Protocol Pre CPOE (N=131) Post CPOE (N=111) P 39. 9± 1. 16 39. 3± 1. 19 NS 59% 63% NS Anion Gap (mmol/L) 27. 9± 0. 54 28. 2± 0. 6 NS Bl Sugar (mg/d. L) 565. 1± 17. 5 588. 3± 23. 2 NS 2. 6± 0. 06 2. 6± 0. 07 NS Age Male (%) Ketone (1 -3 U)
CPOE Driven DKA/HHS Protocol Pre CPOE (N=131) Post CPOE (N=111) P 39. 9± 1. 16 39. 3± 1. 19 NS 59% 63% NS Anion Gap (mmol/L) 27. 9± 0. 54 28. 2± 0. 6 NS Bl Sugar (mg/d. L) 565. 1± 17. 5 588. 3± 23. 2 NS 2. 6± 0. 06 2. 6± 0. 07 NS Age Male (%) Ketone (1 -3 U)
 ICU LOS (hrs) Total LOS (hrs)") CPOE Driven DKA/HHS Protocol Outcomes Pre CPOE (N=131) ICU LOS (hrs) Total LOS (hrs) Time to Anion gap clearance (hrs) Time to Ketone clearance (hrs) Hypoglycemic Episodes (BS<55) Post CPOE (N=111) P 44. 3 ± 2. 43 91. 3 ± 6. 4 34. 2 ± 1. 74 64. 3 ± 3. 9 0. 007 0. 001 15. 4 ± 1. 16 10. 3 ± 0. 44 0. 001 56. 4 ± 5. 45 37. 3 ± 3. 4 0. 003 15 ± 0. 04% 14 ± 0. 04 % 0. 969
CPOE Driven DKA/HHS Protocol Outcomes Pre CPOE (N=131) ICU LOS (hrs) Total LOS (hrs) Time to Anion gap clearance (hrs) Time to Ketone clearance (hrs) Hypoglycemic Episodes (BS<55) Post CPOE (N=111) P 44. 3 ± 2. 43 91. 3 ± 6. 4 34. 2 ± 1. 74 64. 3 ± 3. 9 0. 007 0. 001 15. 4 ± 1. 16 10. 3 ± 0. 44 0. 001 56. 4 ± 5. 45 37. 3 ± 3. 4 0. 003 15 ± 0. 04% 14 ± 0. 04 % 0. 969
 MICU CPOE Lessons Learned • Organizational/Physician Resistance – Executive staff commitment – Physician champions – Address workflow and policy changes (physician, nursing participation is critical) • Cost – Single Vendor (interoperability) – Focus on safety – Measure impact • Product Immaturity – Establish long-term relationship with vendor – Expect to use resources to “customize” application
MICU CPOE Lessons Learned • Organizational/Physician Resistance – Executive staff commitment – Physician champions – Address workflow and policy changes (physician, nursing participation is critical) • Cost – Single Vendor (interoperability) – Focus on safety – Measure impact • Product Immaturity – Establish long-term relationship with vendor – Expect to use resources to “customize” application
 MICU CPOE Lessons Learned • Training – Universal computer literacy – Flexibility to meet house staff needs • Time efficiency is critical – Sign-on – User acceptance testing • CPOE can drive critical care performance improvement – Protocolization/guideline implementation with order sets – Integrate Evidence Based Medicine – IS staff need clinical experience
MICU CPOE Lessons Learned • Training – Universal computer literacy – Flexibility to meet house staff needs • Time efficiency is critical – Sign-on – User acceptance testing • CPOE can drive critical care performance improvement – Protocolization/guideline implementation with order sets – Integrate Evidence Based Medicine – IS staff need clinical experience
 MICU CPOE Lessons Learned • Appropriate support important – On Site Command post – 24/7 Tech Support During go-live • Project Management – Issue escalation process – Address the technology and integration issue first • Measuring up to the VA system
MICU CPOE Lessons Learned • Appropriate support important – On Site Command post – 24/7 Tech Support During go-live • Project Management – Issue escalation process – Address the technology and integration issue first • Measuring up to the VA system
 CPOE System Requirements for Intensive Care Unit Use • http: //www. sccm. org/corpor ate_resources/coalition_for_ critical_care_excellence/ Documents/cpoe. pdf Questions Andy Steele Andy. Steele@dhha. org
CPOE System Requirements for Intensive Care Unit Use • http: //www. sccm. org/corpor ate_resources/coalition_for_ critical_care_excellence/ Documents/cpoe. pdf Questions Andy Steele Andy. Steele@dhha. org
 Questions? Contact Information Andy Steele, MD Andy. Steele@dhha. org
Questions? Contact Information Andy Steele, MD Andy. Steele@dhha. org