a2e30ce785594c30032fe2310b77f941.ppt
- Количество слайдов: 38



CPC November 27, 2007 Michael J. Choi, M. D. Division of Nephrology Johns Hopkins University SOM mchoi 3@jhmi. edu

CPC p E-mail from C Weiner to discuss CPC n n Acute renal failure Electrolyte disturbance

Case: Renal mass

Progressive renal mass: History p HIV since 1997 n p ESRD n p Acquired cystic renal disease – multiple small cysts Pulmonary mass 12/03 dx after (7/02) n n p Lymphoma Metastasis? But chest lesion stable/improving Sarcoid – retroperitoneal lymph nodes involved Mycobacterium Avium Complex

Progressive renal mass: p p PMH: Hepatitis B, C FH: no cancer, sickle cell n n n p p Von Hippel Lindau (AD) mutiple bilat renal cysts/RCC Tuberous sclerosis - multiple bilateral angiomyolipomas Sickle cell trait - Renal medullary CA → aggressive SH: remote IVDU, smoker Meds: no contribution Up to Date

Progressive renal mass: p PE: n n p Gen: somnolent, requires O 2? Febrile? basilar rhonchi, rales 1+ edema No skin lesions (Tub sclerosis, melanoma) Labs: n n n BUN/Cr =24/5. 1 - compatible with dialysis pt Hypercalcemia? (RCC, lymphoma) Total protein 7. 2 and albumin 2. 9 HIV, hepatitis - polyclonal gammopathy p Myeloma - monoclonal gammopathy p

Renal biopsy
 → non diagnostic <33% p")
Renal biopsy: avoid nephrectomy Fine needle aspiration (>20 guage) → non diagnostic <33% p Biopsy (<18 guage): 89 -100% sensitivity for malignancy p n n n 97. 7% sensitive, 100% specific 4% non diagnostic Adverse effects Hemorrhage 1. 3%, 0. 7% delayed retroperitoneal hemorrhage from pseudoaneurysm rupture, p Tumor seeding- none (0. 01% in literature) p Matauren et al. AJR 2007; 188: 563 -570.

Kidney Anatomy Paspulati et al. Radiol Clin N Am 2006; 44: 787 -803

Mass: Differential Diagnosis Renal cell cancer p Angiomyolipoma, Oncocytoma, others p Metastasis p Renal cysts p Lymphoma p Inflammatory mass - Renal abscess p n May be indisinguishable from cancer Paspulati et al. Radiol Clin N Am 2006; 44: 787 -803

CT scan of Mass p Does it enhance with contrast on imaging? n p Enhancement. If ↑>20 HU → malignancy Calcifications n Indicates stone, inflammation or bleed

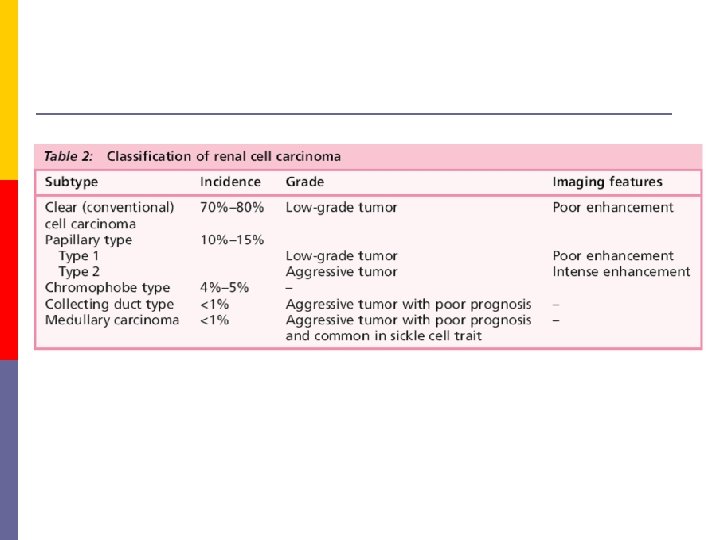
Renal cell Equal W and AA, Historically M> F but now more equal, age 60 -80 p Classic triad of hematuria, abdominal pain, abdominal mass < 10% p Paraneoplastic syndrome in 20 -40% p n p Fever, hypercalcemia Case: n n n Renal biopsy usually diagnostic. Not just a solitary mass Slow

Other masses p Angiomyolipoma n n p Oncocytoma n n p Central stellate scar Homogenous enhancement Leiomyoma n p Fat > 4 cm may rupture Benign tumor of smooth muscle origin Women 20 -50 Variable radiologic presentation ( cystic/solid) Hemangiomas Reninoma n HTN, hypokalemia

Malignancy p Metastasis n Lung, breast, GI tract, melanoma Wagle et al J Urol 1975; 114: 3032 n n p seen in 7 -13% on autopsy Usually bilateral, multiple masses Not here

Bosniak Cyst Classification I Simple cyst. No septations, calcifications, or enhancement. Low density of cyst like water No Rx II Few thin septa, may see enhancement of septa, not cyst No Rx IIF Multiple septa, septa may be calcificied and thick. Follow up studies III Thick irregular walls with septa enhancement (hemorrhagic or infected cysts, 40 -60% cystic neoplasm) Surgery? IV + soft tissue enhancement Surgery

Renal cysts p Bosniak I – simple cyst, thin wall, no septations, calcifications, or enhancement. Density like water www. skeletalscintigraphy. com/fp/images/rcyst. jpg

Renal cysts p Bosniak III – Thickened irregular walls, septa may enhance, not tissue. 40 -60% are malignant Israel GM, Bosniak MA. Radiology 2005: 236: 441 -450

Renal cysts p Bosniak IV – +Soft tissue enhancement p This big - ? metastasis Up to Date
 p B cell non Hodgkins lymphoma")
Lymphoma Kidneys often involved at autopsy (37. 6%) p B cell non Hodgkins lymphoma p n n prevalence in HIV >100 -150 x general population Can be in one or both kidneys, retroperitoneal spread, usually bilateral multiple nodules Enhance < than kidney with contrast Sheth S et al. Radio. Graphics 2006; 26: 1151 -1168

Lymphoma and HIV p Lymphomatous infiltration of the kidneys n n Sx: Flank pain, abdominal mass, + acute renal failure Bilateral, diffuse enlargement Pre therapy Post chemo Adler L et al. Inf Dis Clin Practice. 2000; 9: 378 -383.

Infection: Renal/perirenal abscess p Renal abscess n n n p Ascending infection 75%, 66% have anatomic abnormality (reflux) → medullary abscess Hematogenous spread → cortical abscess. Sx: dysuria, fevers, chills, flank pain, see pyuria Perinephric abscess n n Ascending and hematogenous Worse symptoms

Up to Date Renal abscess Perinephric abscess

Renal abscess p Bacterial n 14% had sterile culture Coehlo et al. World J Surg 2007; 31: 431 -436 n p ESRD – Staph aureus related catheter infection? Fungal – Disseminated disease - Candida, Aspergillus, Histoplasmosis n n Kidney is most common seeded site Presentations p p Nonspecific, may be abscess and fistula formation Acute - bilateral, Chronic –unilateral Urine culture positive This mass is too slow growing

Renal abscess- TB p p p Hematogenous spread Stay in glomeruli → reactivate 10 -15 yrs later, spreads to medulla and collecting system. Presentation n p No specific symptoms UTI sterile pyuria Diagnosis n n AFB sensitivity 22 -78% CT: Kidney scarring and calcification, and small calcified bladder in 1/3

TB Browne RFJ et al. Eur Radiol 2004; 14: E 168 -E 183

Mycobacterium avium complex p Disseminated disease in immunocompromised n n p Lung disease* n n p p Portal possibly gut or lung with hematogenous spread 39% with CD 4 counts < 10 (Pt with 14 -30) Upper lobe cavity in elderly smokers with prior lung damage, Nodules, bronchiectasis Lymphadenitis* Other mycobacteria infection sites: n skin and soft tissue infection, tenosynovitis and osteomyelitis, catheter related, surgical site

2 years of gross hematuria, presents with fever, lethargy. Urine AFB + Our case

Mycobacterium Avium Complex p Rare renal involvement with HIV+ pts n n p Nephrocalcinosis Glomerular disease Interstitial inflammation of renal transplant Abscess Done n Was placed on therapy 2 months ago, sx worse
 p >2/3 of time")
Xanthogranulomatous pyelonephritis Chronic pyelonephritis (sxs 2 days to 5 yrs) p >2/3 of time have infected, obstructing stone p Presentation p n n Women 3: 1. 50 -60 yrs old, h/o UTI Non specific: fever, flank pain malaise, anorexia. No pyuria in one series Secondary amyloidosis with nephrotic syndrome. Urine culture + in 62% in one series

Xanthogranulomatous pyelonephritis Goldman SM et al. AJR 1984; 141: 963 -969 our case Loffroy R et al. Clinical Radiol 2007; 62: 884 -890 p CT n n n See diffuse destruction/ renal enlargement. stone May look like malignancy. Can extend to psoas

Xanthogranulomatous pyelonephritis p Pathology: n n n p p p Kidney replaced by necrotic tissue + fat laden foamy macrophages granulomatous, lymphoplasmacytic infiltrate Infected stone Pathogenesis: ? Treatment: Surgical removal Dx? Xanthogranulomatous pyelonephritis from Mycobacteria
- homogeneous p Hematoma p Anuerysms p")
Hyperattenuating mass Benign cysts (ADPKD, acquired cystic disease)- homogeneous p Hematoma p Anuerysms p If enhance > 10 Housdfield units on CTsolid, probably malignancy p If MRI T 1 nad T 2 with fat supression p n If enhancing hyperattenuating renal mass tha appears hypodens on T 2, do bx to prevent resectinof a bening tumor

Hyperatteunuating renal mass

Oncocytoma p Indistinguishable by imaging

Acquired cystic kidney disease ESRD p Multiple > 4 bilateral cysts, usually small (<0. 5, up to 3 cm) p Incidence of renal cell ca 4 -7% p

Angiomyolipoma: see fat* p p p Harmartoma, > 4 cm → possible rupture 80% sporadic, 20% tuberous sclerosis n Younger age- multiple , bilateral , larger
a2e30ce785594c30032fe2310b77f941.ppt