

f50d98fb9f291970c0b13fe30c331704.ppt
- Количество слайдов: 70

 CPC Department of Neurosurgery RMC n Allied Hospitals Dr Osama Ahmad Registrar Dr Soban Sarwar Gondal Senior Registrar Prof. Dr Nadeem Akhter Head of Department
CPC Department of Neurosurgery RMC n Allied Hospitals Dr Osama Ahmad Registrar Dr Soban Sarwar Gondal Senior Registrar Prof. Dr Nadeem Akhter Head of Department
 DEMOGRAPHIC DETAILS Name : Father name : Age/Sex : R/O : Occupation : D. O. A : M. O. A : Rizwan Saeed Mohd Saeed 34 years/ M Rawalpindi Employee in oil and gas company 19 -6 -16 Emergency
DEMOGRAPHIC DETAILS Name : Father name : Age/Sex : R/O : Occupation : D. O. A : M. O. A : Rizwan Saeed Mohd Saeed 34 years/ M Rawalpindi Employee in oil and gas company 19 -6 -16 Emergency
 Ear discharge 3 days. 1 week. 3") PRESENTING COMPLAINTS Altered Sensorium Headache Fever (R) Ear discharge 3 days. 1 week. 3 months.
PRESENTING COMPLAINTS Altered Sensorium Headache Fever (R) Ear discharge 3 days. 1 week. 3 months.
 HISTORY OF PRESENTING ILLNESS Headache continuous, generalized, moderate to severe in intensity , partially relieved by analgesics, associated with nausea and vomiting. No associated fits. Fever off and on , low grade (unrecorded) with no associated features. Drowsy and disoriented for the last 3 days.
HISTORY OF PRESENTING ILLNESS Headache continuous, generalized, moderate to severe in intensity , partially relieved by analgesics, associated with nausea and vomiting. No associated fits. Fever off and on , low grade (unrecorded) with no associated features. Drowsy and disoriented for the last 3 days.
 ear discharge for the last") HISTORY OF PRESENTING ILLNESS Previous h/o of intermittent (R) ear discharge for the last 1 year with recent intermittent exacerbation for the last 3 months , purulent, yellowish in color , foul smelling with associated impaired hearing on that side. He consulted multiple local doctors regarding the ear discharge and took off and on treatment
HISTORY OF PRESENTING ILLNESS Previous h/o of intermittent (R) ear discharge for the last 1 year with recent intermittent exacerbation for the last 3 months , purulent, yellowish in color , foul smelling with associated impaired hearing on that side. He consulted multiple local doctors regarding the ear discharge and took off and on treatment
 SYSTEMIC REVIEW CNS : GIT : Chest : Genitourinary : CVS : Locomotor : Endocrine : Drowsiness NAD NAD NAD
SYSTEMIC REVIEW CNS : GIT : Chest : Genitourinary : CVS : Locomotor : Endocrine : Drowsiness NAD NAD NAD
 PAST HISTORY Medicine : Off and on treatment for ear discharge from local doctor (No record available). Took analgesics for headache. No pre-morbidity. Surgical No past surgical history.
PAST HISTORY Medicine : Off and on treatment for ear discharge from local doctor (No record available). Took analgesics for headache. No pre-morbidity. Surgical No past surgical history.
 HISTORY Personal Non smoker. Non addict Employee at oil and gas company. Married with two daughters. Socioeconomic Middle class family.
HISTORY Personal Non smoker. Non addict Employee at oil and gas company. Married with two daughters. Socioeconomic Middle class family.
 GENERAL PHYSICAL EXAMINATION Young patient with altered sensorium lying in his bed. Pallor º Jaundiceº Dyspneaº Clubbingº Cyanosis º Vitals Pulse : 94/min B. P : 110/70 R. R : 20/min Temp : 100 ˚F
GENERAL PHYSICAL EXAMINATION Young patient with altered sensorium lying in his bed. Pallor º Jaundiceº Dyspneaº Clubbingº Cyanosis º Vitals Pulse : 94/min B. P : 110/70 R. R : 20/min Temp : 100 ˚F
 CENTRAL NERVOUS SYSTEM GCS: 12/15. Higher Mental functions : Patient was drowsy and disoriented. Apathic Cranial Nerves: Fundoscopy: Cranial nerves: Grade 2 papilledema bilaterally Grossly normal.
CENTRAL NERVOUS SYSTEM GCS: 12/15. Higher Mental functions : Patient was drowsy and disoriented. Apathic Cranial Nerves: Fundoscopy: Cranial nerves: Grade 2 papilledema bilaterally Grossly normal.
 CENTRAL NERVOUS SYSTEM Motor system Bulk normal B/L Tone normal B/L Power: moving all four limbs. Reflexes Superficial …. . Deep …. . Plantars …. Intact Downgoing B/L
CENTRAL NERVOUS SYSTEM Motor system Bulk normal B/L Tone normal B/L Power: moving all four limbs. Reflexes Superficial …. . Deep …. . Plantars …. Intact Downgoing B/L
 CENTRAL NERVOUS SYSTEM Lobes : Could not be assessed because of decrease level of consciousness. Cerebellar signs: Could not be assessed because of decrease level of consciousness. Sensory system: Could not be assessed because of decrease level of consciousness.
CENTRAL NERVOUS SYSTEM Lobes : Could not be assessed because of decrease level of consciousness. Cerebellar signs: Could not be assessed because of decrease level of consciousness. Sensory system: Could not be assessed because of decrease level of consciousness.
 SYSTEMIC Respiratory : B/L air entry equal GIT : Soft, Nontender B. S+ve CVS : S 1+S 2+0
SYSTEMIC Respiratory : B/L air entry equal GIT : Soft, Nontender B. S+ve CVS : S 1+S 2+0
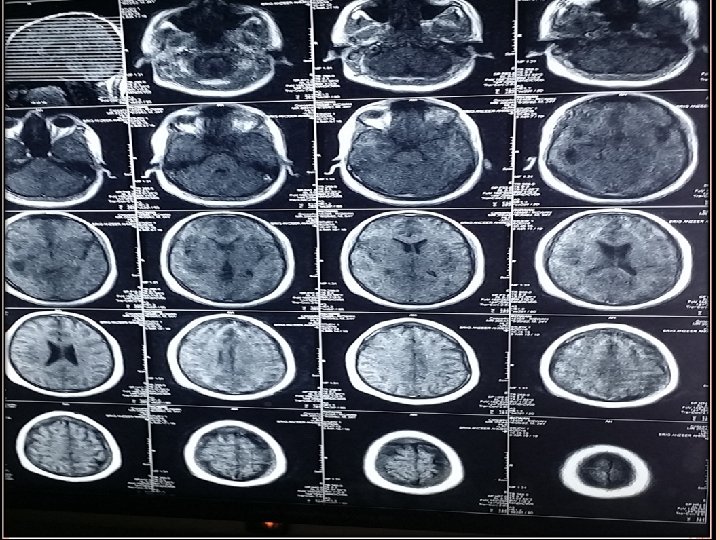
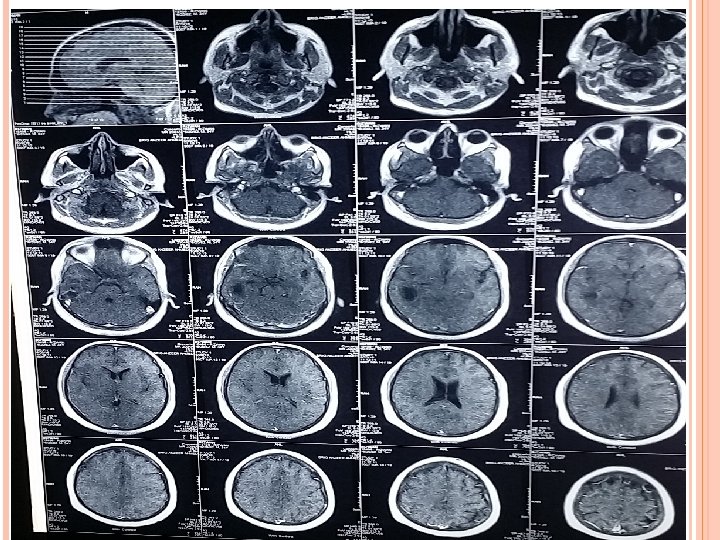
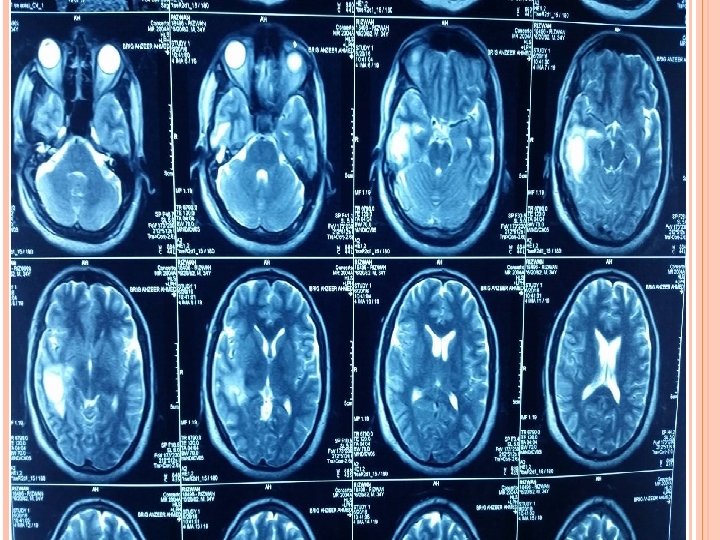
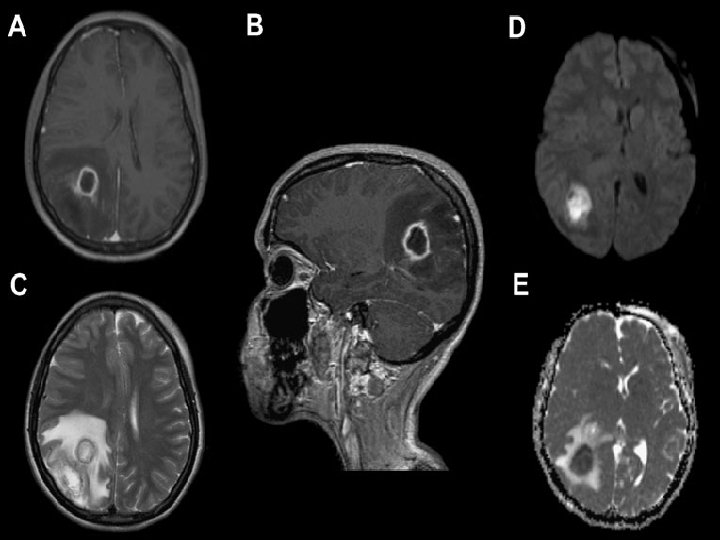
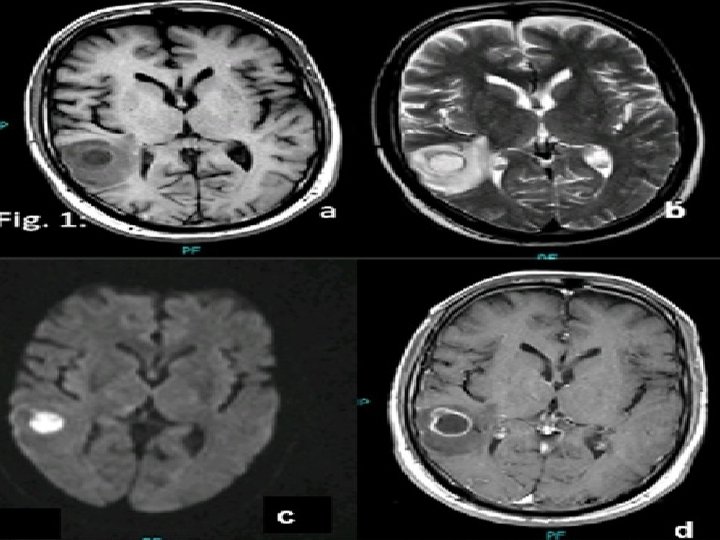
 CRP (3. 2 mg/L) ESR (28 mm/hr). Imaging") INVESTIGATIONS Blood Tests CBC (TLC-12000/u. L) CRP (3. 2 mg/L) ESR (28 mm/hr). Imaging CT scan Brain ( plain ) CT scan Brain with contrast. MRI Brain with contrast.
INVESTIGATIONS Blood Tests CBC (TLC-12000/u. L) CRP (3. 2 mg/L) ESR (28 mm/hr). Imaging CT scan Brain ( plain ) CT scan Brain with contrast. MRI Brain with contrast.
 TREATMENT Medical Inf N/S 1000 ml iv BD Triple regimen started. Inj ceftriaxone 2 g iv BD Inj Vancomycin 1 g iv TDS Inj metronidazole 500 mg TDS Inj decacdron 4 mg iv TDS Inj epival 500 mg iv BD Inf mannitol 150 ml iv TDS Inj Toradol 30 mg iv TDS Inj Zantac 50 mg iv TDS
TREATMENT Medical Inf N/S 1000 ml iv BD Triple regimen started. Inj ceftriaxone 2 g iv BD Inj Vancomycin 1 g iv TDS Inj metronidazole 500 mg TDS Inj decacdron 4 mg iv TDS Inj epival 500 mg iv BD Inf mannitol 150 ml iv TDS Inj Toradol 30 mg iv TDS Inj Zantac 50 mg iv TDS
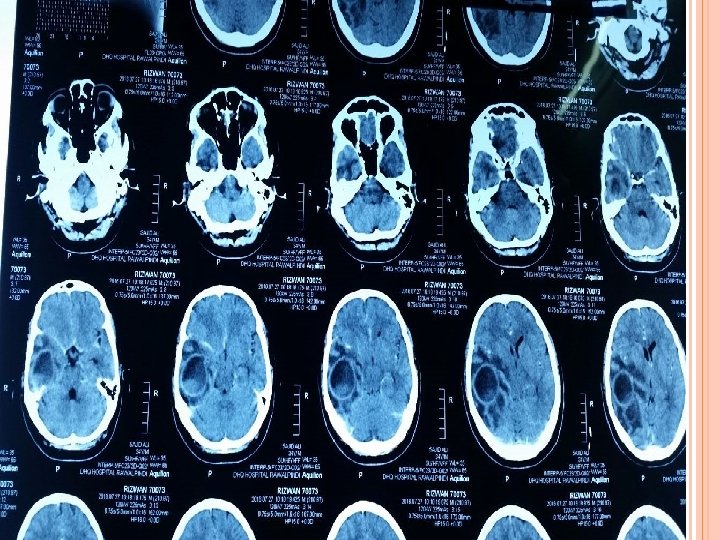
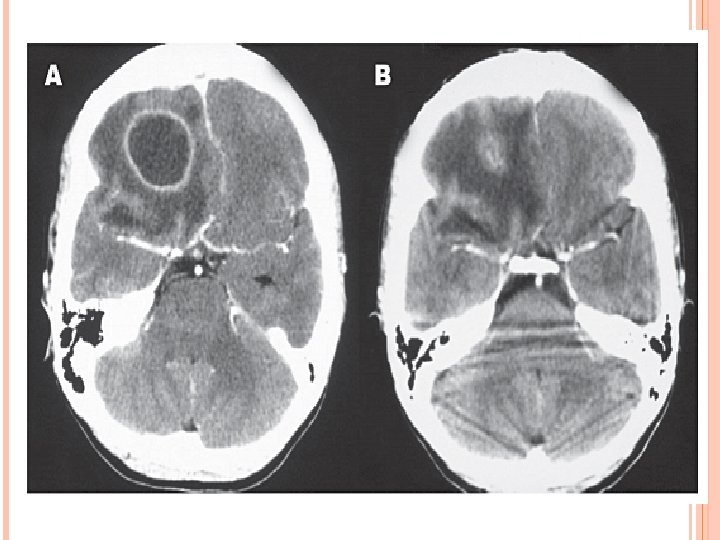
") CT SCAN BRAIN WITH CONTRAST ( AFTER 1 WEEK)
CT SCAN BRAIN WITH CONTRAST ( AFTER 1 WEEK)
 15 ml pus aspirated Pus sent") SURGERY Aspiration thru burr hole (28 -6 -16) 15 ml pus aspirated Pus sent for culture and sensitivity.
SURGERY Aspiration thru burr hole (28 -6 -16) 15 ml pus aspirated Pus sent for culture and sensitivity.
") CHECK CT SCAN ( 1 ST POD)
CHECK CT SCAN ( 1 ST POD)
 POSTOPERATIVE PERIOD Patient conscious oriented Taking orally Pus for C/S showed proteus mirabilis. Discharged on 4 th POD with iv antibiotics ( 4 weeks ). Advised: Wound care Daily dressing OPD follow up after 10 days.
POSTOPERATIVE PERIOD Patient conscious oriented Taking orally Pus for C/S showed proteus mirabilis. Discharged on 4 th POD with iv antibiotics ( 4 weeks ). Advised: Wound care Daily dressing OPD follow up after 10 days.
 FOLLOW UP Presented on 11 th POD Conscious , oriented Wound … healthy. Stitches removed IV antibiotics ( 4 weeks ) ENT consultation
FOLLOW UP Presented on 11 th POD Conscious , oriented Wound … healthy. Stitches removed IV antibiotics ( 4 weeks ) ENT consultation
 ENT Advised: Admission Plan of Mastoidectomy.
ENT Advised: Admission Plan of Mastoidectomy.
") SURGERY Modified radical mastoidectomy by ENT department (19 -7 -16)
SURGERY Modified radical mastoidectomy by ENT department (19 -7 -16)
 FOLLOW UP Patient remain well for 1 week again started having the same symptoms. Presented in emergency with decreased level of consciousness. After initial management CT scan was performed which showed re-accumulation of abscess.
FOLLOW UP Patient remain well for 1 week again started having the same symptoms. Presented in emergency with decreased level of consciousness. After initial management CT scan was performed which showed re-accumulation of abscess.
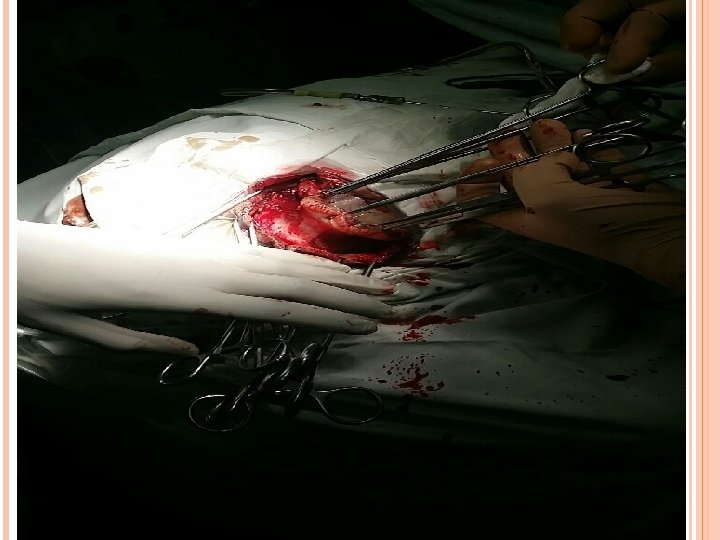
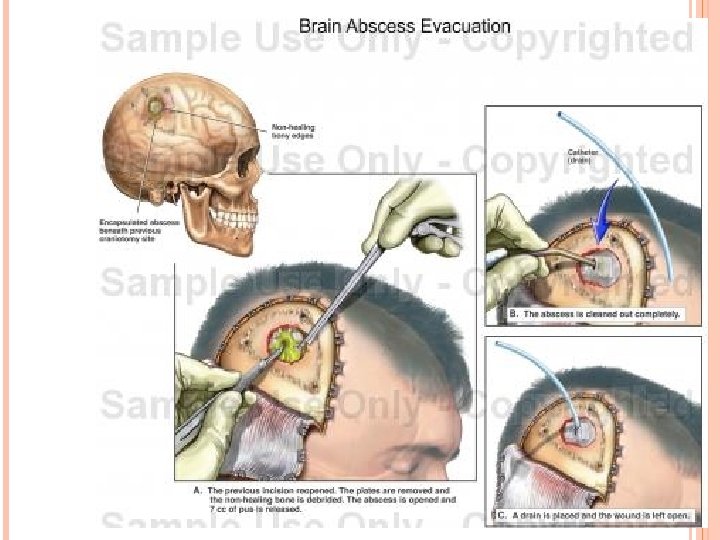
") SURGERY Total excision along with capsule ( 2 -8 -16)
SURGERY Total excision along with capsule ( 2 -8 -16)
 PER OP
PER OP


 PER OP
PER OP
") POSTOP SCAN ( 1 ST POD)
POSTOP SCAN ( 1 ST POD)
 HISTOPATHOLOGY Specimen : Wall Biopsy of Brain Abscess Diagnosis Abscess wall Showing xanthogranulomatous inflammation Negative for Granulomatous inflammation Negative for malignancy
HISTOPATHOLOGY Specimen : Wall Biopsy of Brain Abscess Diagnosis Abscess wall Showing xanthogranulomatous inflammation Negative for Granulomatous inflammation Negative for malignancy
 FOLLOW UP Discharged on 5 th POD with iv antibiotics. Advised OPD follow up after 1 week.
FOLLOW UP Discharged on 5 th POD with iv antibiotics. Advised OPD follow up after 1 week.
 `
`
 TOPIC DISCUSSION
TOPIC DISCUSSION
 (Subcontinent) Decreased incidence (because of") INCIDENCE 1 -2% 8% of SOL in brain (USA) (Subcontinent) Decreased incidence (because of antibiotic and improved life) Increased patient. incidence in immune compromised
INCIDENCE 1 -2% 8% of SOL in brain (USA) (Subcontinent) Decreased incidence (because of antibiotic and improved life) Increased patient. incidence in immune compromised
 ETIOLOGY 1. Infection : o From PNS , middle ear and mastoid o Characterized by solitary and located superficially o Infection spread by either direct or through veins (thrombophlibitis of diploic vein) o PNS (frontal and temporal lobe ) o Middle ear (temporal lobe) o mastoid (temporal lobe and cerebellum)
ETIOLOGY 1. Infection : o From PNS , middle ear and mastoid o Characterized by solitary and located superficially o Infection spread by either direct or through veins (thrombophlibitis of diploic vein) o PNS (frontal and temporal lobe ) o Middle ear (temporal lobe) o mastoid (temporal lobe and cerebellum)
 2. Heamatogenous Dissemination of microorganism from remote site of infection Multiple and deeply located Mostly located in the frontal and parietal lobe Primary foci include (skin pustule , pulmonary infection , diverticulitis) Most common type of CHD is TOF 50% Brain abscess in CHD are generally solitary
2. Heamatogenous Dissemination of microorganism from remote site of infection Multiple and deeply located Mostly located in the frontal and parietal lobe Primary foci include (skin pustule , pulmonary infection , diverticulitis) Most common type of CHD is TOF 50% Brain abscess in CHD are generally solitary
 3. Penetrating trauma : o Can occur within days or years o Contaminated bone fragments and debris provide a nidus for infection o Lodged bullet may be source of infection o Basal skull fracture with CSF leak and meningitis cause post traumatic abscess
3. Penetrating trauma : o Can occur within days or years o Contaminated bone fragments and debris provide a nidus for infection o Lodged bullet may be source of infection o Basal skull fracture with CSF leak and meningitis cause post traumatic abscess
 4. Previous craniotomy Because of : A. Introduce of micro-organisms at time of surgery B. Or spread of intracranialy through the wound C. Bone flap infection 5. Immune compromised person
4. Previous craniotomy Because of : A. Introduce of micro-organisms at time of surgery B. Or spread of intracranialy through the wound C. Bone flap infection 5. Immune compromised person
 MICROBIOLOGY Otogenic and dental infection caused by anaerobic organism Sinusitis caused by staph aureus, aerobic streptococci CHD caused by strep. In immune deficiency caused by fungus In AIDS by toxoplasma gondi Incidence of –ve culture is 25 -30%
MICROBIOLOGY Otogenic and dental infection caused by anaerobic organism Sinusitis caused by staph aureus, aerobic streptococci CHD caused by strep. In immune deficiency caused by fungus In AIDS by toxoplasma gondi Incidence of –ve culture is 25 -30%
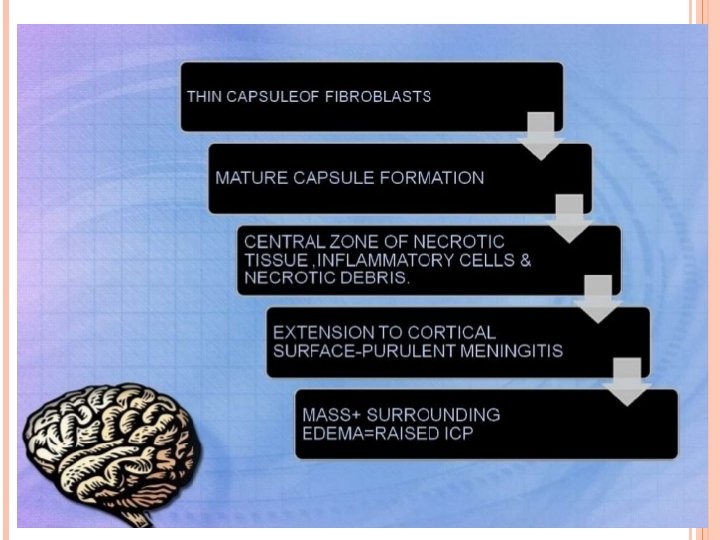
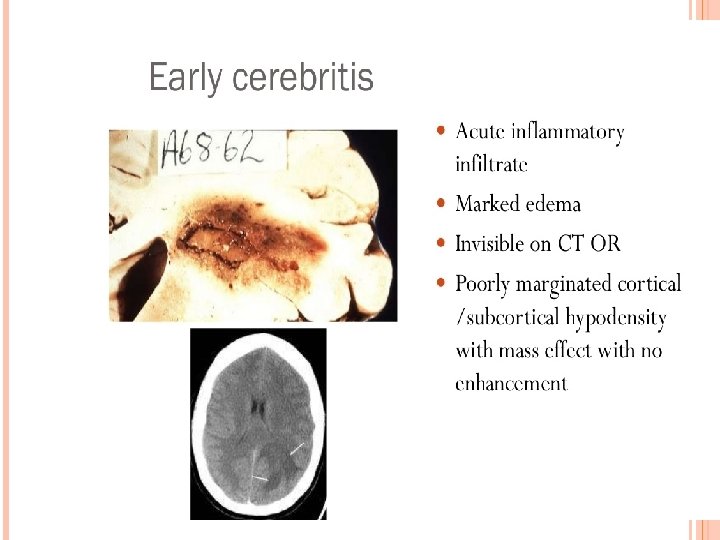
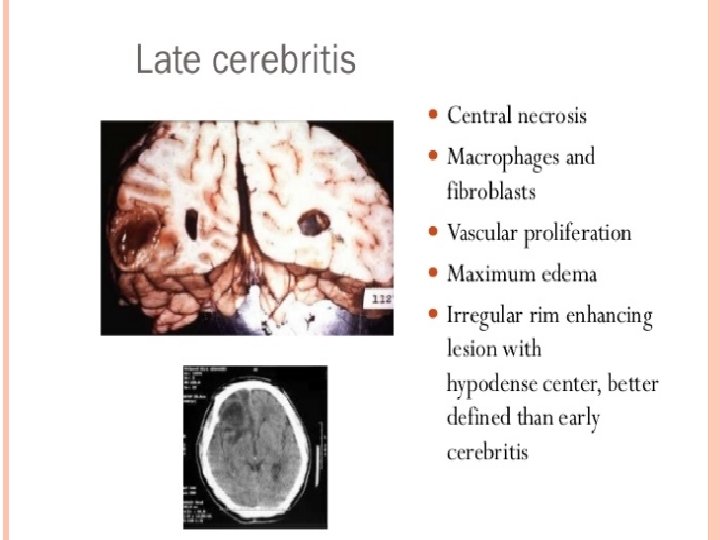
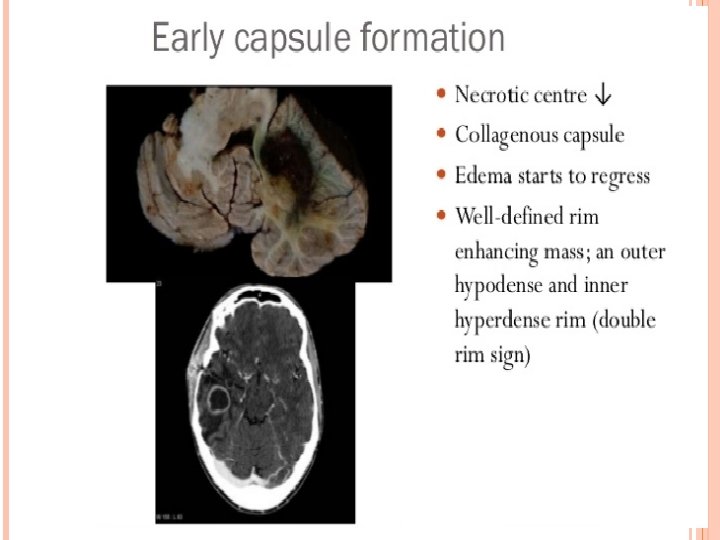
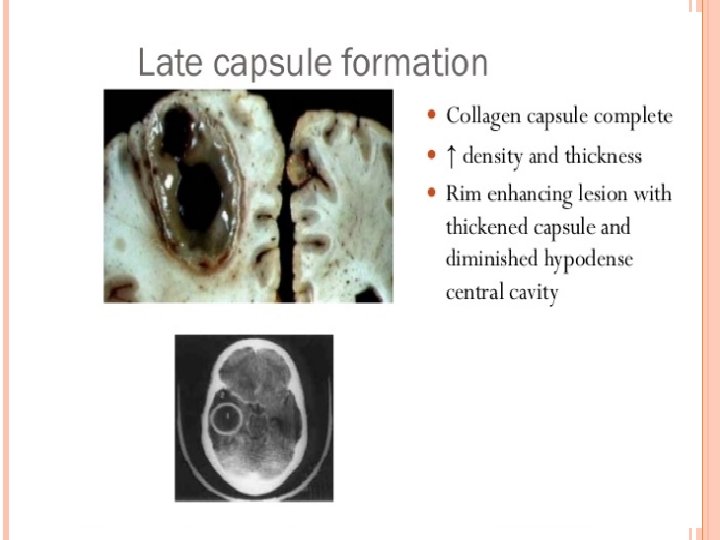
 PATHOGENESIS AND HISTOPATHOLOGY OF BRAIN ABSCESS
PATHOGENESIS AND HISTOPATHOLOGY OF BRAIN ABSCESS
 Clinical presentation : § § § Occur in majorities in the first 2 decades of life Males more affected ( cause is unknown ) Largely dependent on immune status Infants : increase in head circumference , bulging fontanel , separation of cranial sutures , vomiting , irritability , seizures Signs of Raised ICP and Focal Neurological Deficit v Edema v Cerebral tissue destruction
Clinical presentation : § § § Occur in majorities in the first 2 decades of life Males more affected ( cause is unknown ) Largely dependent on immune status Infants : increase in head circumference , bulging fontanel , separation of cranial sutures , vomiting , irritability , seizures Signs of Raised ICP and Focal Neurological Deficit v Edema v Cerebral tissue destruction
 2. Change in conscious level (") Symptoms : 1. Headache ( 90 %) 2. Change in conscious level ( 60 %) 3. FND ( 60 %) § Parietal lobe : hemiparesis § Temporal lobe : dysphasia § Cerebellar : ataxia and nystagmus 4. Fever (more than 50 %) 5. Nausea and vomiting ( 50 %) 6. Seizure ( 50 %) 7. Papilledema and meningismus
Symptoms : 1. Headache ( 90 %) 2. Change in conscious level ( 60 %) 3. FND ( 60 %) § Parietal lobe : hemiparesis § Temporal lobe : dysphasia § Cerebellar : ataxia and nystagmus 4. Fever (more than 50 %) 5. Nausea and vomiting ( 50 %) 6. Seizure ( 50 %) 7. Papilledema and meningismus
 LABORATORY FINDINGS 1. 2. 3. WBC : normal or mild increase ESR : increase in 90% CSF : not specific 1. Opening pressure 2. Protein 3. Glucose 4. Culture
LABORATORY FINDINGS 1. 2. 3. WBC : normal or mild increase ESR : increase in 90% CSF : not specific 1. Opening pressure 2. Protein 3. Glucose 4. Culture
 INVESTIGATIONS Radiological characteristic of brain abscess 1. Brain CT with contrast Ring enhancement Sigle Locus/Multi loculation Multiplicity Finding of gas
INVESTIGATIONS Radiological characteristic of brain abscess 1. Brain CT with contrast Ring enhancement Sigle Locus/Multi loculation Multiplicity Finding of gas

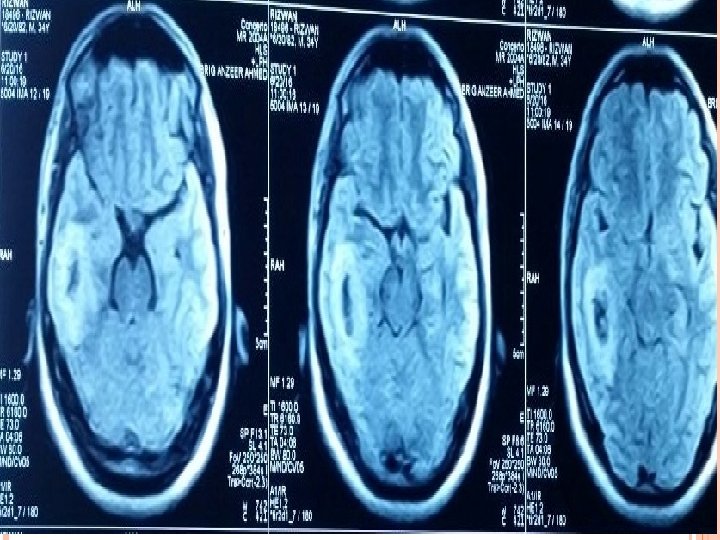
 Capsule ( hyperintense) Edema ( hypointense)") MRI T 1 : necrotic center ( hypointense) Capsule ( hyperintense) Edema ( hypointense) T 2 : necrotic center ( hyperintense) Capsule ( hypointense) Edema ( hyperintense)
MRI T 1 : necrotic center ( hypointense) Capsule ( hyperintense) Edema ( hypointense) T 2 : necrotic center ( hyperintense) Capsule ( hypointense) Edema ( hyperintense)
 MANAGEMENT 1. Antibiotic therapy : Antibiotic is mandatory and should given Antibiotics depends on C/S Treatment depend on the etiology ◦ ◦ Sinusitis : ( penicillin + metronidazole ) Otitis : ( penicillin + metronidazole + 3 rd generation cephalosporin) Metastatic abscess : (metronidazole + 3 rd generation cephalosporin) Post traumatic abscess ( vancomycin) Advantage of antibiotic therapy Small size Deep seated Multiple
MANAGEMENT 1. Antibiotic therapy : Antibiotic is mandatory and should given Antibiotics depends on C/S Treatment depend on the etiology ◦ ◦ Sinusitis : ( penicillin + metronidazole ) Otitis : ( penicillin + metronidazole + 3 rd generation cephalosporin) Metastatic abscess : (metronidazole + 3 rd generation cephalosporin) Post traumatic abscess ( vancomycin) Advantage of antibiotic therapy Small size Deep seated Multiple
 TREATMENT OPTIONS 2. Aspiration : Advantages : 1. Confirm diagnosis 2. Remove of purulent material 3. Provide environment for antibiotics to work 4. Provide immediate relief of IICP Stereotactic guided aspiration
TREATMENT OPTIONS 2. Aspiration : Advantages : 1. Confirm diagnosis 2. Remove of purulent material 3. Provide environment for antibiotics to work 4. Provide immediate relief of IICP Stereotactic guided aspiration
 TREATMENT OPTIONS 3. Excision of brain abscess Advantages 1. 2. 3. Traumatic abscess ( contain foreign body and bone fragment ) Fungal abscess Gas containing abscess Disadvantages
TREATMENT OPTIONS 3. Excision of brain abscess Advantages 1. 2. 3. Traumatic abscess ( contain foreign body and bone fragment ) Fungal abscess Gas containing abscess Disadvantages
 Follow up CT weekly during antibiotic therapy And then monthly CT 2 -3 week decrease size of abscess 3 -4 months complete resolution of abscess 6 -9 months no residual contrast enhancement
Follow up CT weekly during antibiotic therapy And then monthly CT 2 -3 week decrease size of abscess 3 -4 months complete resolution of abscess 6 -9 months no residual contrast enhancement
 OUTCOME OF ABSCESS : Mortality influenced by : ØHerniation ØRupture ØClinical ØType of abscess to the ventricle course of the patient of abscess ØNeurological diagnosis state of patient at time of
OUTCOME OF ABSCESS : Mortality influenced by : ØHerniation ØRupture ØClinical ØType of abscess to the ventricle course of the patient of abscess ØNeurological diagnosis state of patient at time of
 v Recurrence: (") v Long term morbidity : ( seizure , FND, Cognitive dysfunction) v Recurrence: ( 5 -10%) causes (inadequate antibiotic therapy, incorrect choice of AB, presence of foreign body , failure to eradicate source of the abscess)
v Long term morbidity : ( seizure , FND, Cognitive dysfunction) v Recurrence: ( 5 -10%) causes (inadequate antibiotic therapy, incorrect choice of AB, presence of foreign body , failure to eradicate source of the abscess)
 Thank You
Thank You