
Congenital Heart Disease Adult CHD is not


- Размер: 14.9 Mегабайта
- Количество слайдов: 68
Описание презентации Congenital Heart Disease Adult CHD is not по слайдам
Congenital Heart Disease
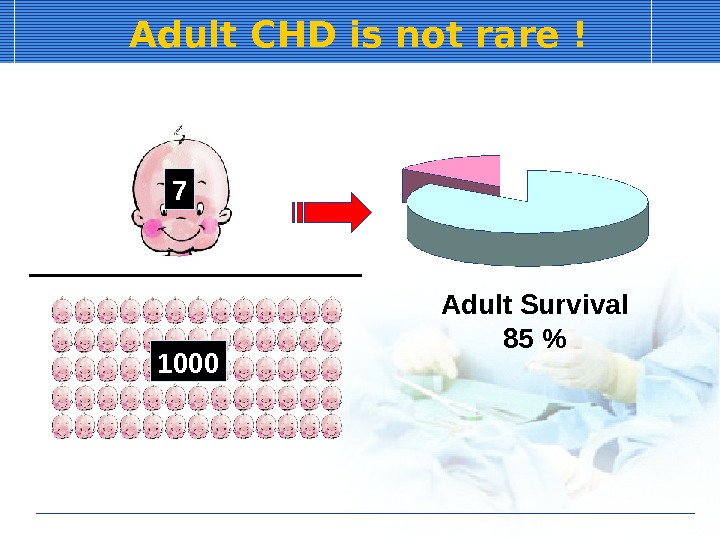
Adult CHD is not rare ! 7 1000 Adult Survival 85 %
Adult Congenital Heart Disease Newly diagnosis Previous diagnosed but not repaired Clinically insignificant lesion Eisenmenger syndrome Performed operation Cure: VSD, PDA New problems: TOF, Fontan….
Congenital Heart Disease (CHD) Simple congenital HD Atrial septal defect: ASD Ventricular septal defect: VSD Patent ductus arteriosus: PDA Pulmonary stenosis: PS) Ebstein’s anomaly Aortic stenosis: AS Complex congenital HD) Tetralogy of Fallot: TOF Transposition of great arteries: TG
Clinical Problems in CHD Heart failure Infective endocarditis Pulmonary hypertension (PHT)
Echo in congenital disease Diagnosis Severity Prognosis Decision of treatment — OP Combined anomaly Evaluaion of cardiac function
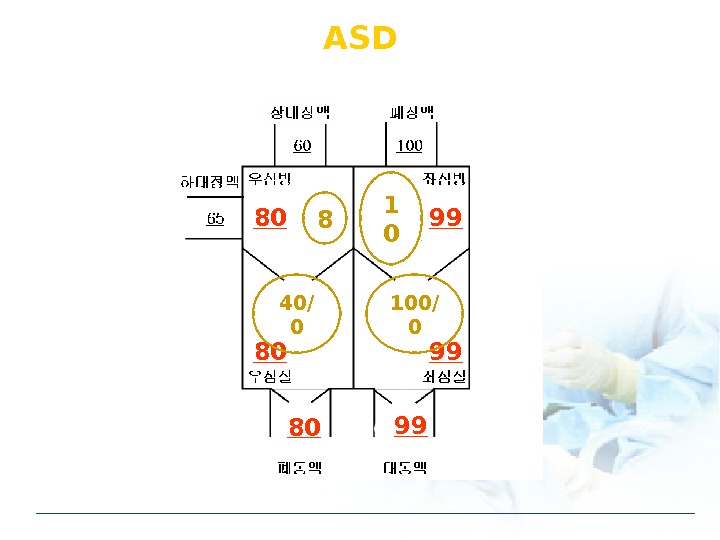
ASD 80 80 80 99 99 998 1 0 40/ 0 100/
Diagnosis of ASD Clinical features Dyspnea, Cardiomegaly, Atrial fibrillation Direct findings Identification of shunt: 2 D echo Confirm of shunt: Doppler Indirect findings Volume overloading of Rt heart — Enlargement of RV, RA, PV Pulmonary hypertension
Echo in ASD When we suspect ASD? How we diagnose ASD? What is type of ASD? How severe ASD? • Enlargement of RV, RA, PV • Pulmonary hypertension: TR jet velocity • Qp/Qs Combined congenital anomaly ASD size
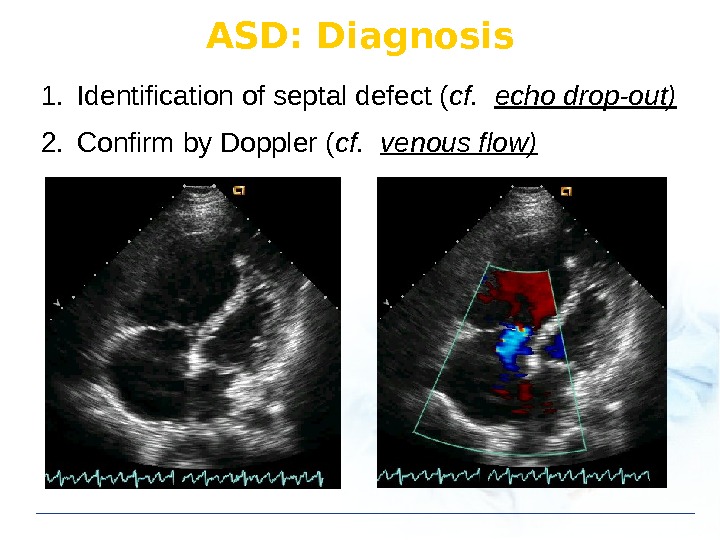
ASD: Diagnosis 1. Identification of septal defect ( cf. echo drop-out) 2. Confirm by Doppler ( cf. venous flow)
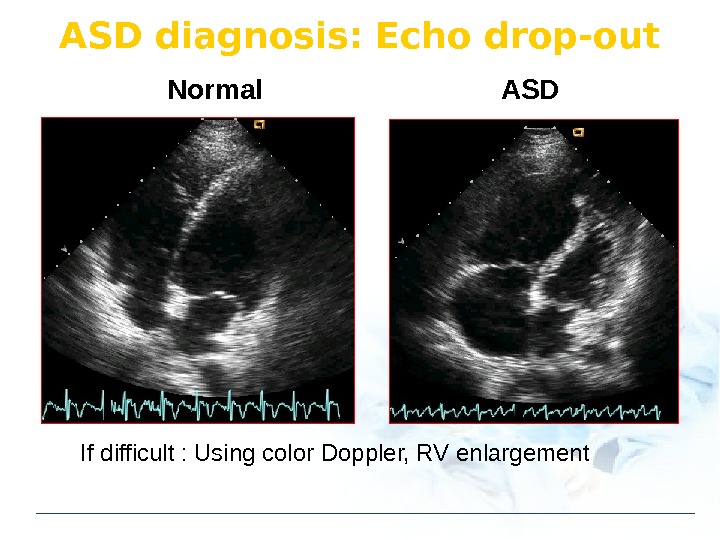
ASD diagnosis: Echo drop-out Normal ASD If difficult : Using color Doppler, RV enlargement
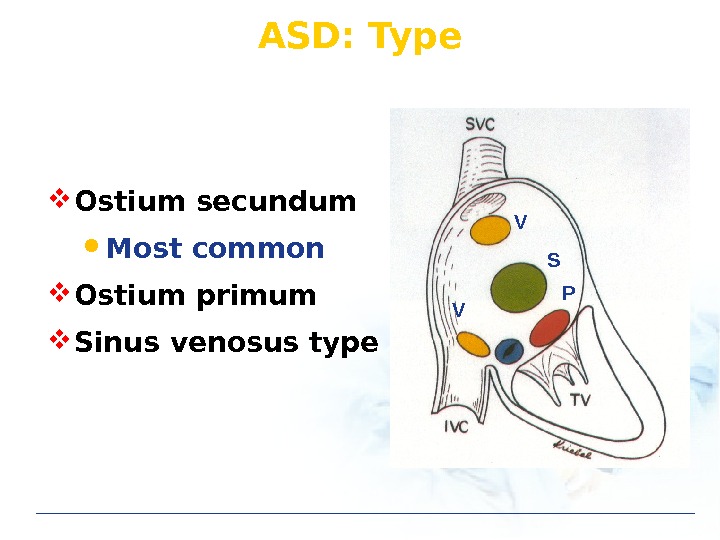
ASD: Type S PV V Ostium secundum Most common Ostium primum Sinus venosus type
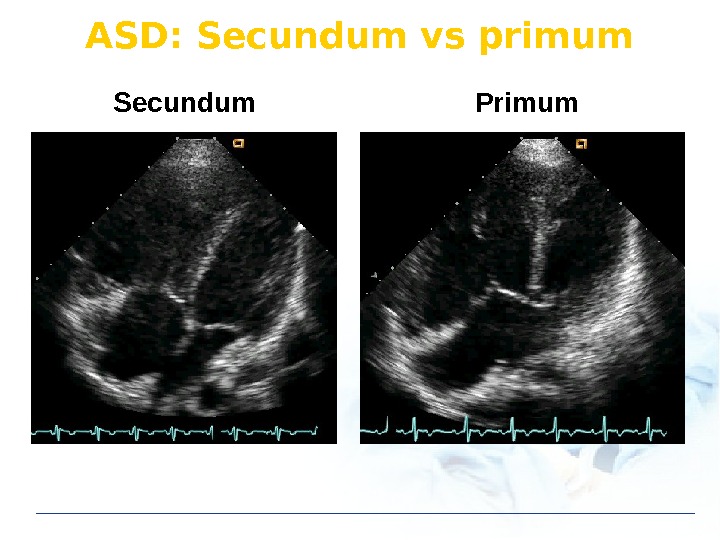
ASD: Secundum vs primum Secundum Primum
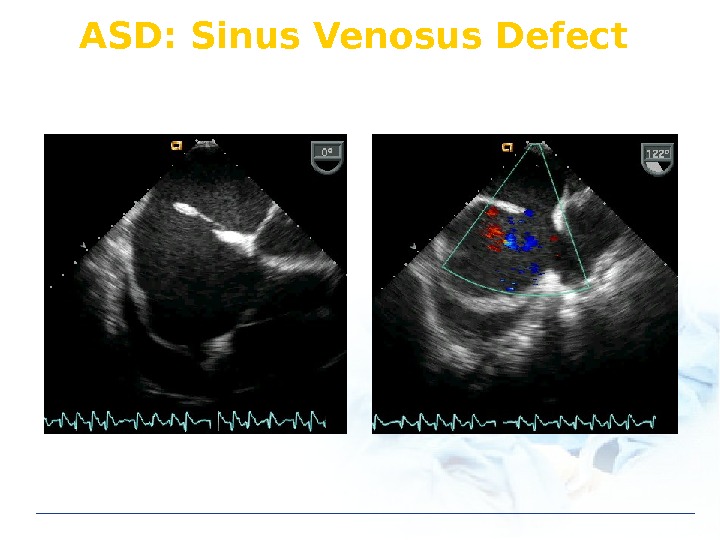
ASD: Sinus Venosus Defect
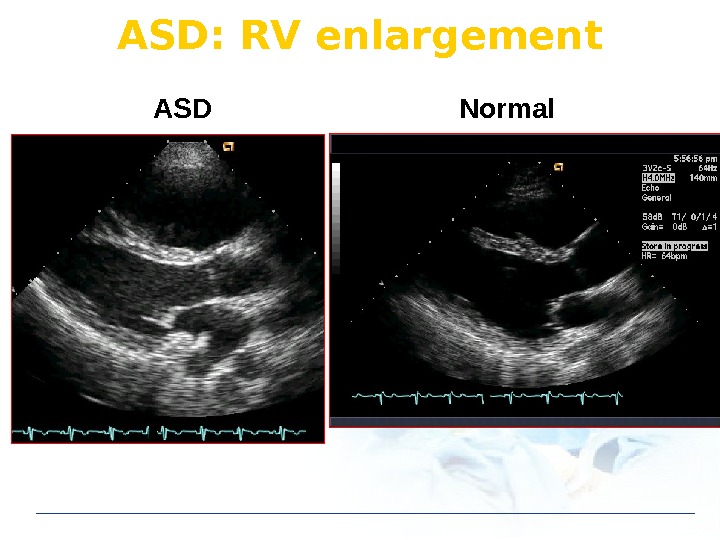
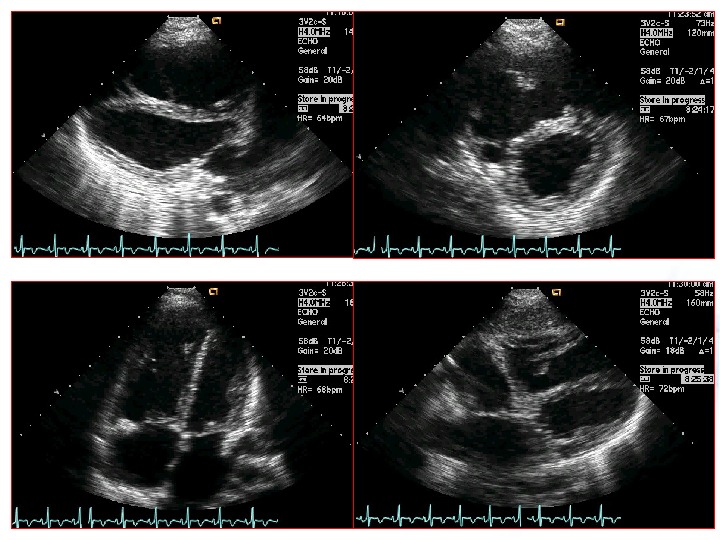
ASD: RV enlargement ASD Normal
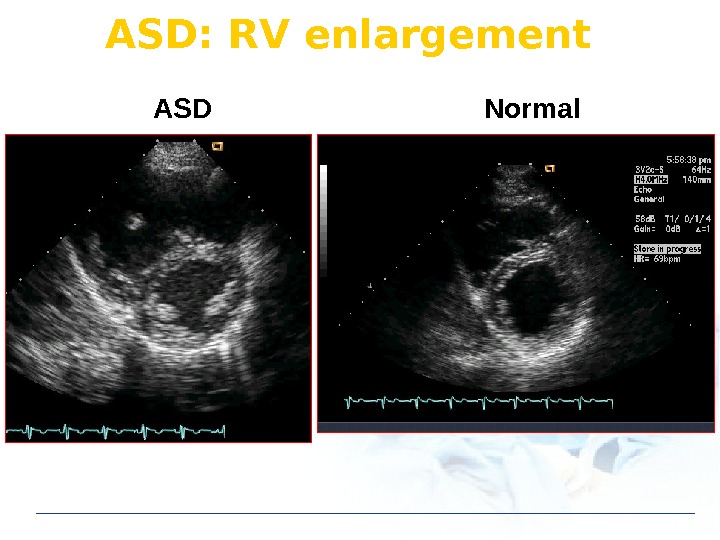
ASD Normal. ASD: RV enlargement
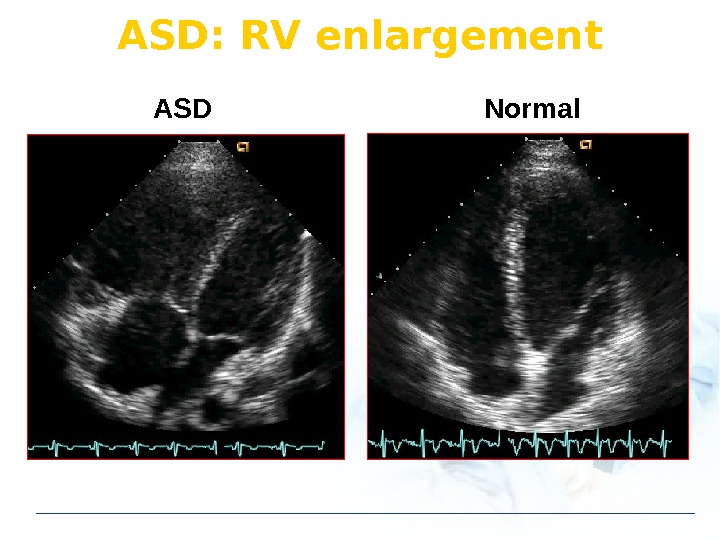
ASD Normal. ASD: RV enlargement
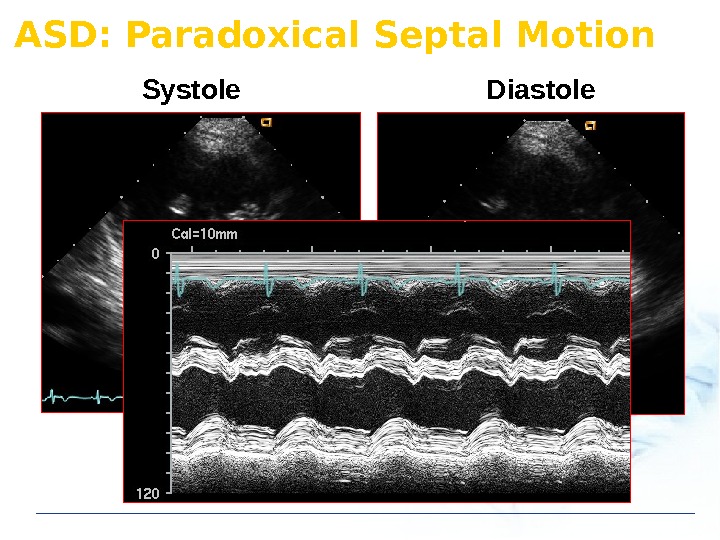
ASD: Paradoxical Septal Motion Systole Diastole
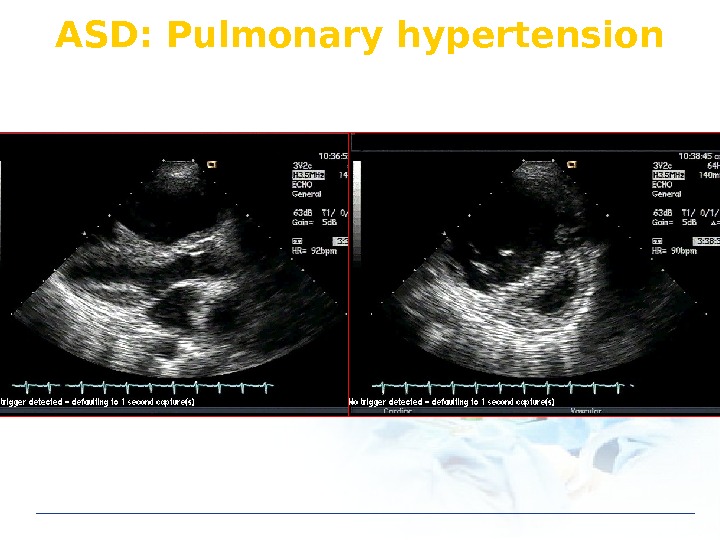
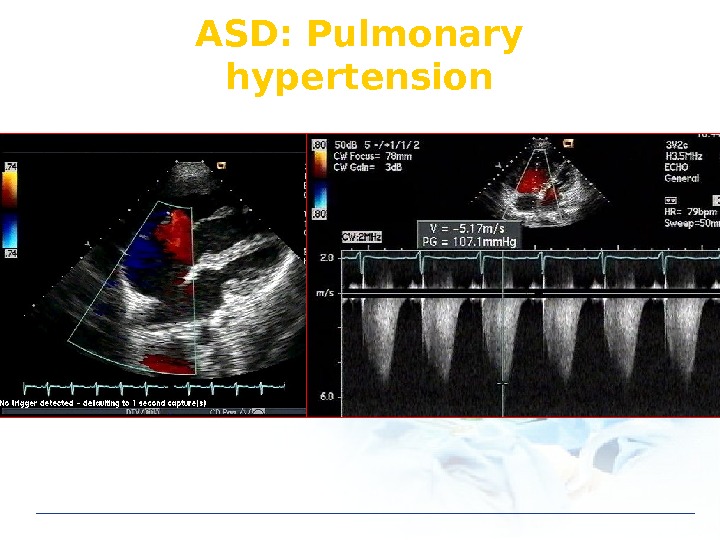
ASD: Pulmonary hypertension
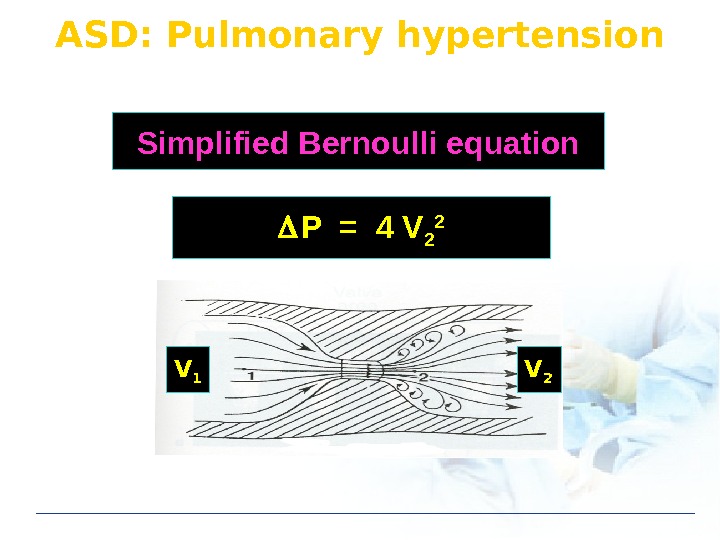
ASD: Pulmonary hypertension P = 4 V 2 2 Simplified Bernoulli equation V 1 V
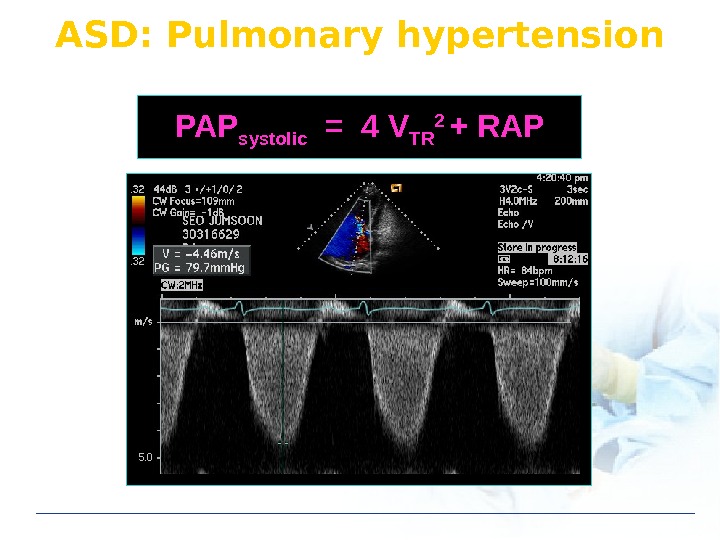
ASD: Pulmonary hypertension PAP systolic = 4 V TR 2 + RAP
ASD: Pulmonary hypertension
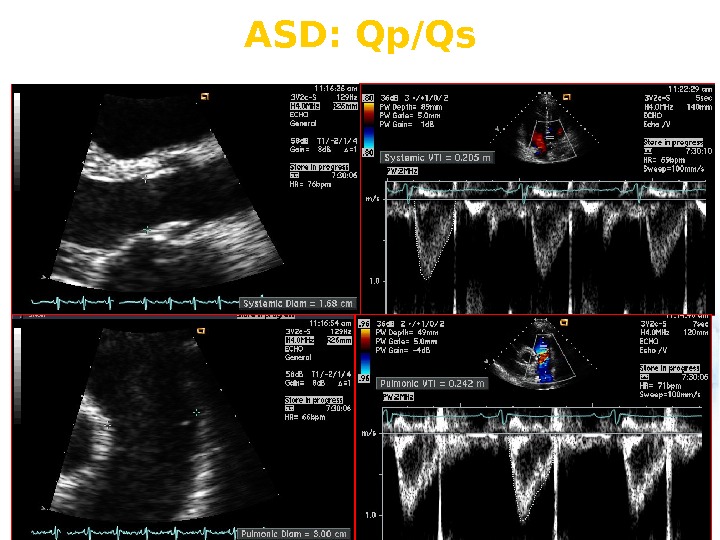
ASD: Qp/Qs
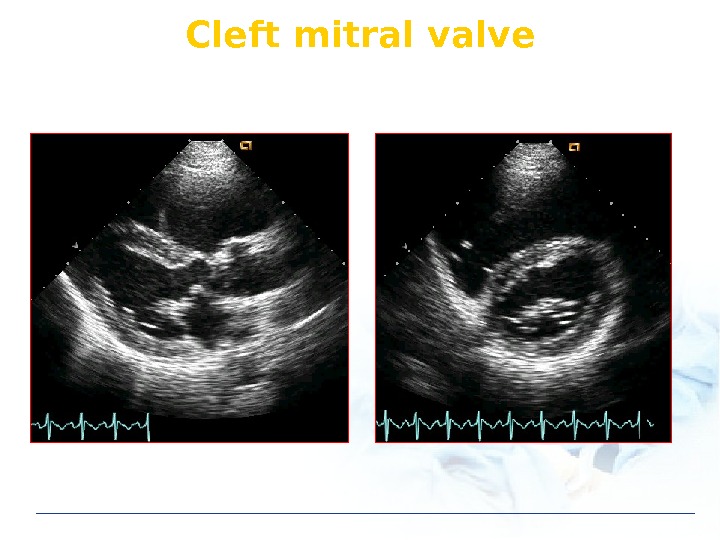
ASD: Combined anomaly Secundum ASD mitral valve prolapse Primum ASD cleft mitral valve Sinus venosus defect anomalous pulmonary venous return
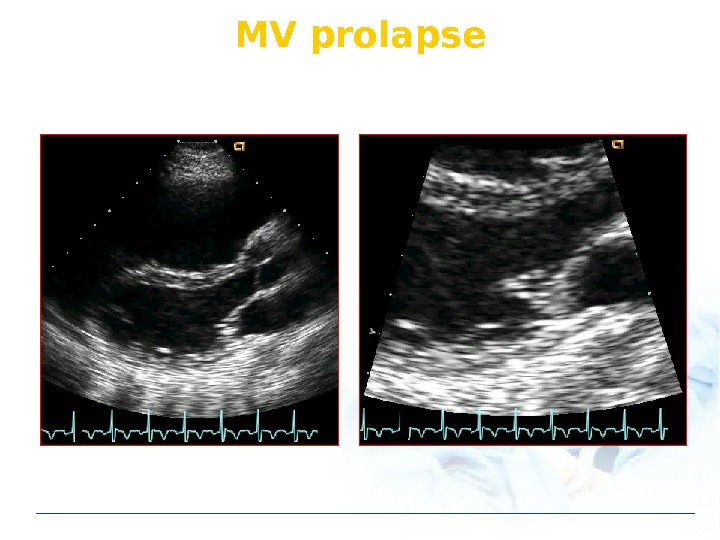
MV prolapse
Cleft mitral valve
ASD: Treatment Medical treatment Endocarditis prophylaxis: not recommended Surgical treatment Indication: Qp/Qs 2. 0 Device closure: secundum ASD Contraindication Severe pulmonary hypertension
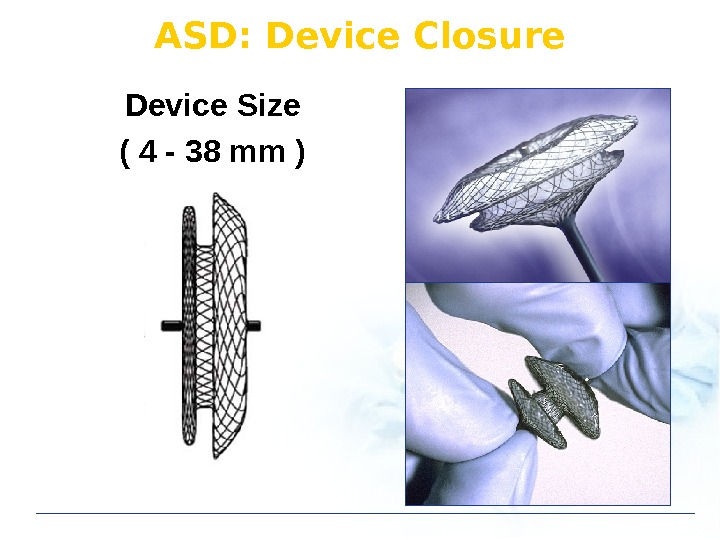
Device Size ( 4 — 38 mm ) ASD: Device Closure
Case: 45/Male, Dyspnea
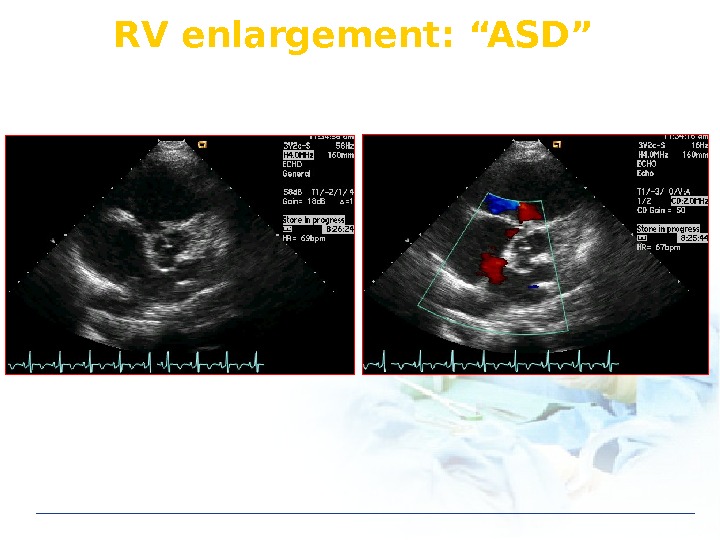
RV enlargement: “ASD”
Echo in ASD Unknown origin RV & RA enlargement TEE in sinus venosus defect
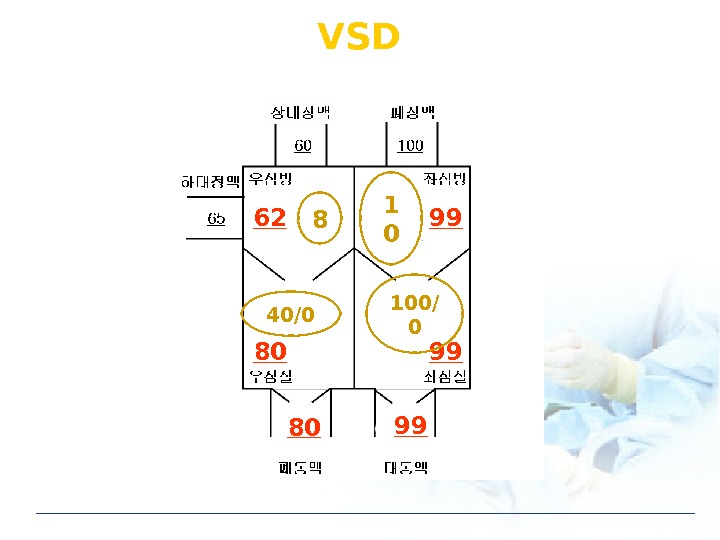
VSD 62 80 80 99 99 998 1 0 40/0 100/
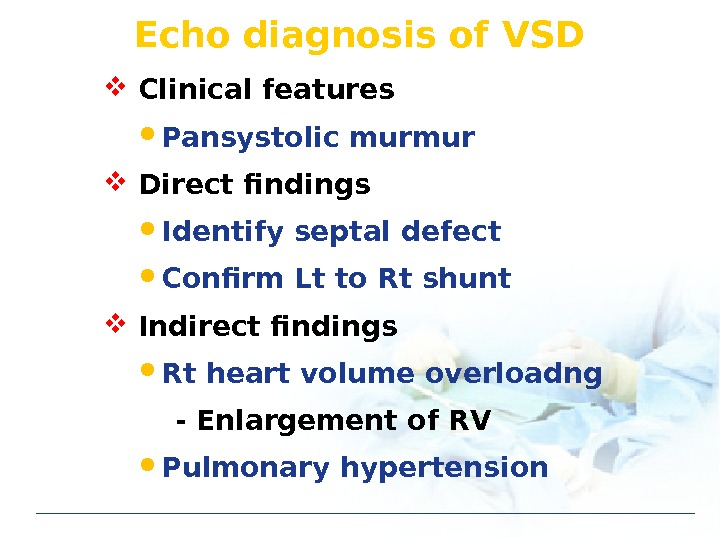
Echo diagnosis of VSD Clinical features Pansystolic murmur Direct findings Identify septal defect Confirm Lt to Rt shunt Indirect findings Rt heart volume overloadng — Enlargement of RV Pulmonary hypertension
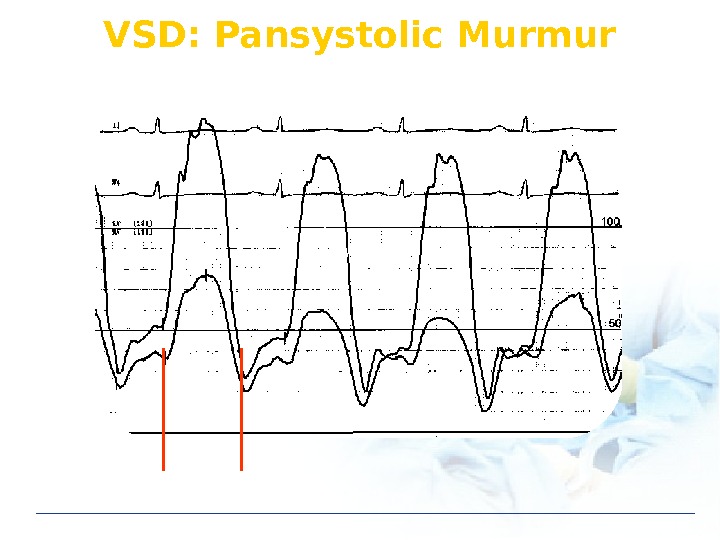
VSD: Pansystolic Murmur
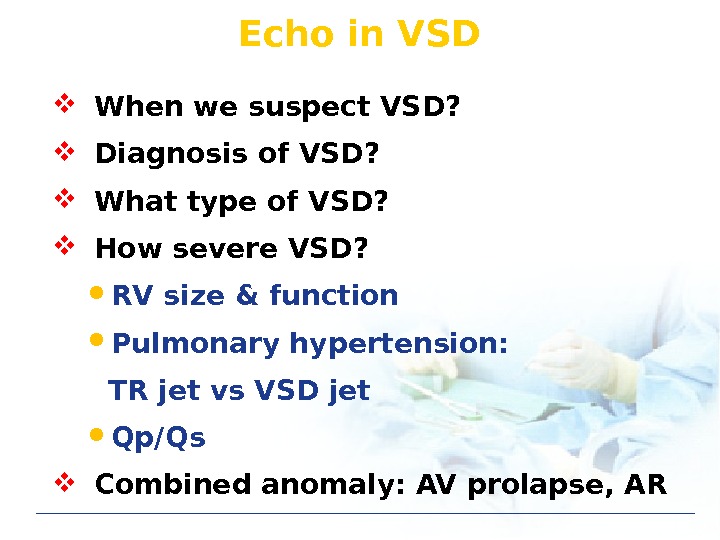
Echo in VSD When we suspect VSD? Diagnosis of VSD? What type of VSD? How severe VSD? RV size & function Pulmonary hypertension: TR jet vs VSD jet Qp/Qs Combined anomaly: AV prolapse, AR
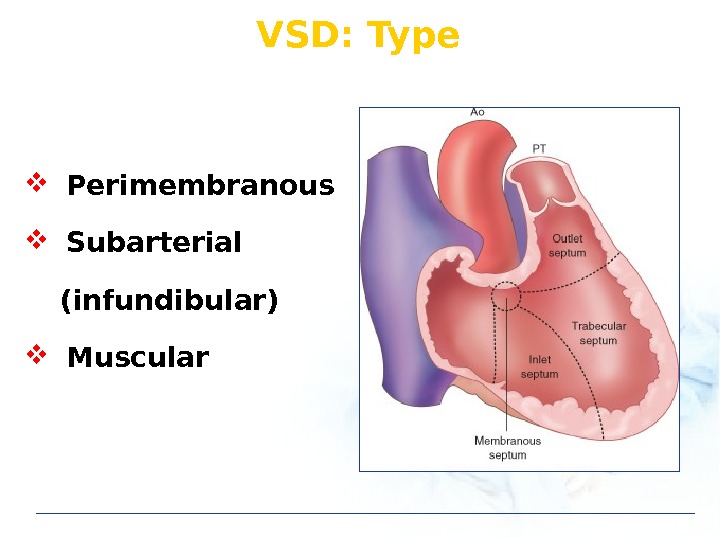
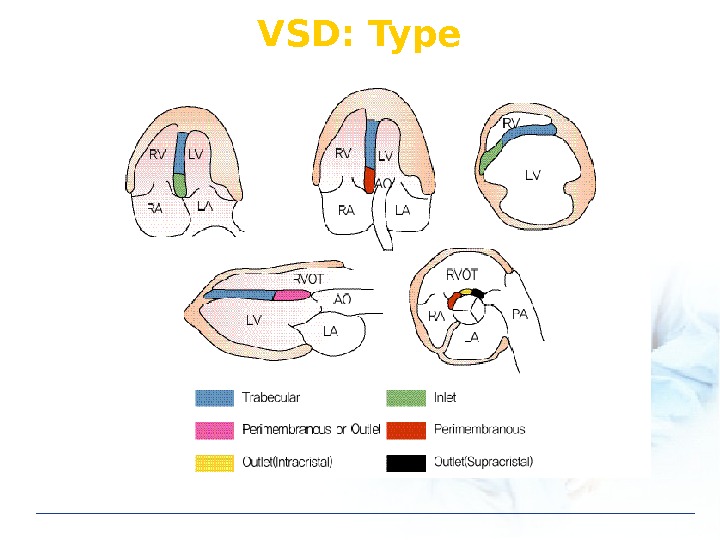
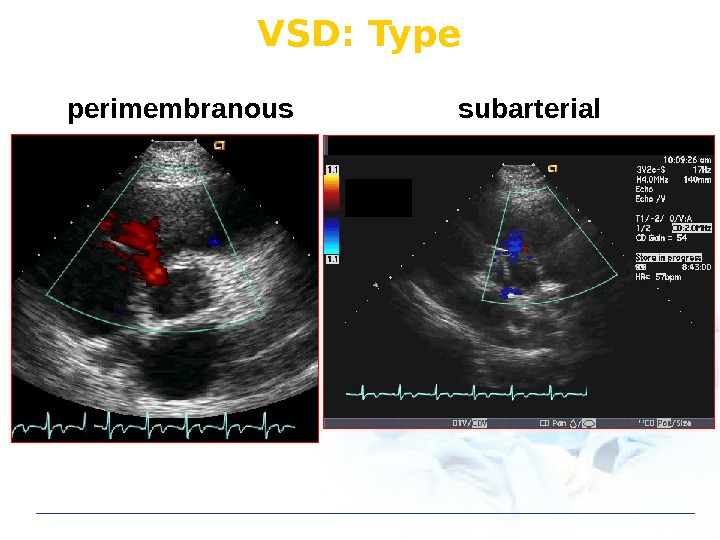
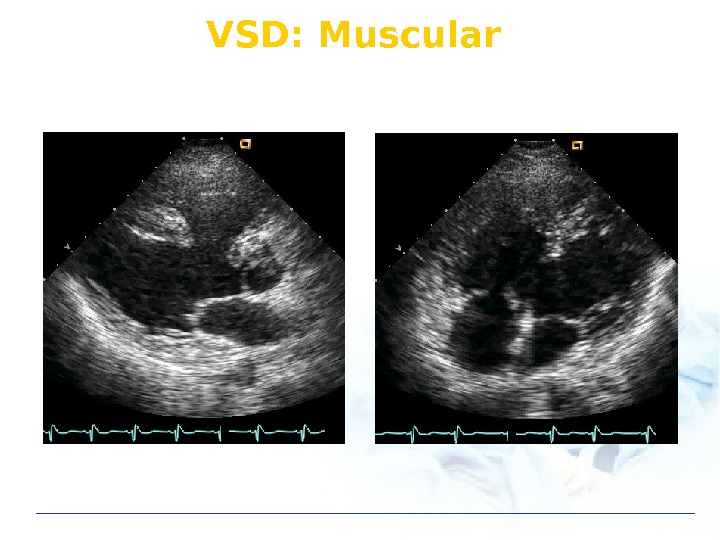
VSD: Type Perimembranous Subarterial (infundibular) Muscular
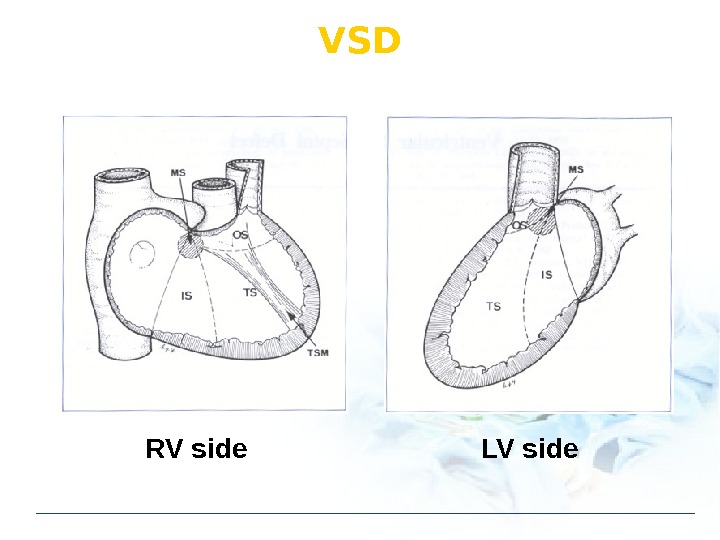
VSD RV side LV side
VSD: Type
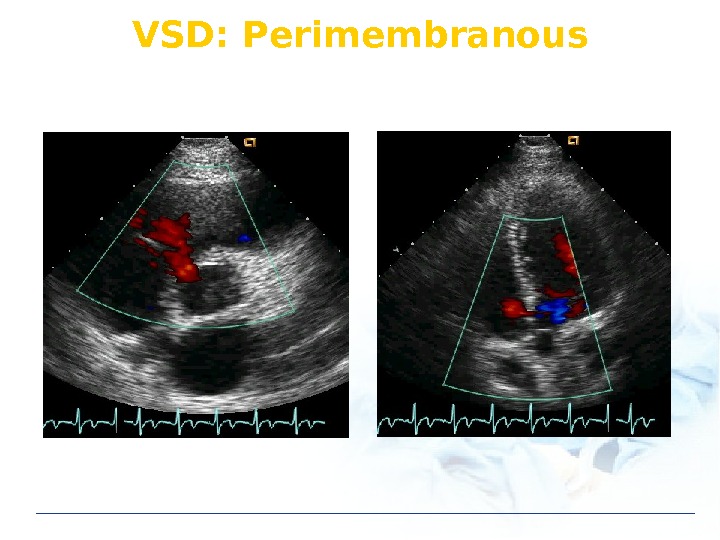
VSD: Perimembranous
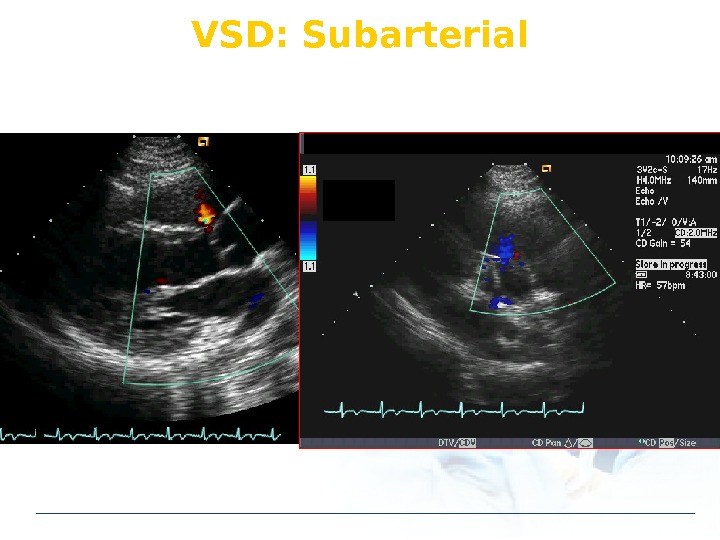
VSD: Subarterial
VSD: Type perimembranous subarterial
VSD: Muscular
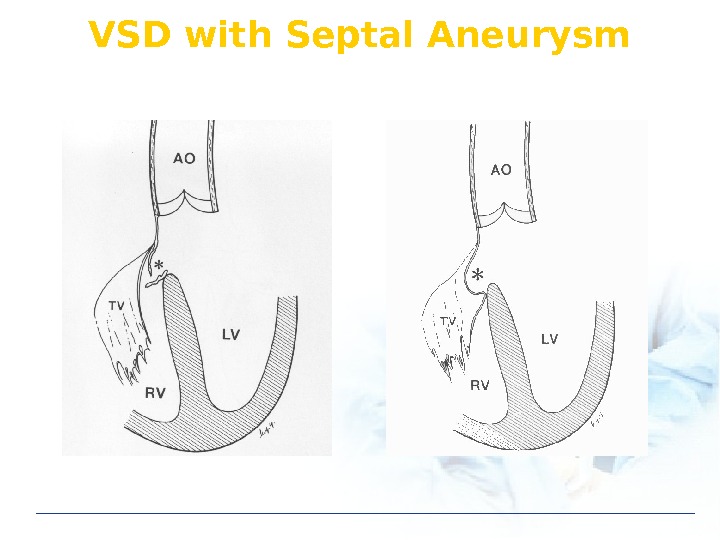
VSD with Septal Aneurysm
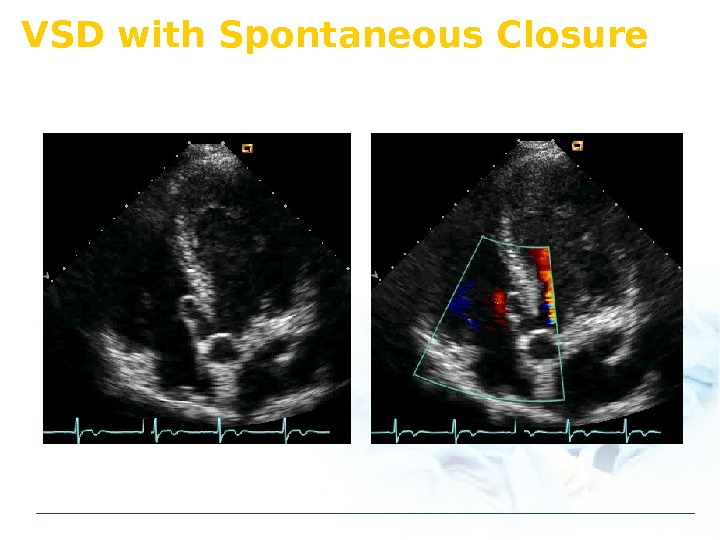
VSD with Spontaneous Closure
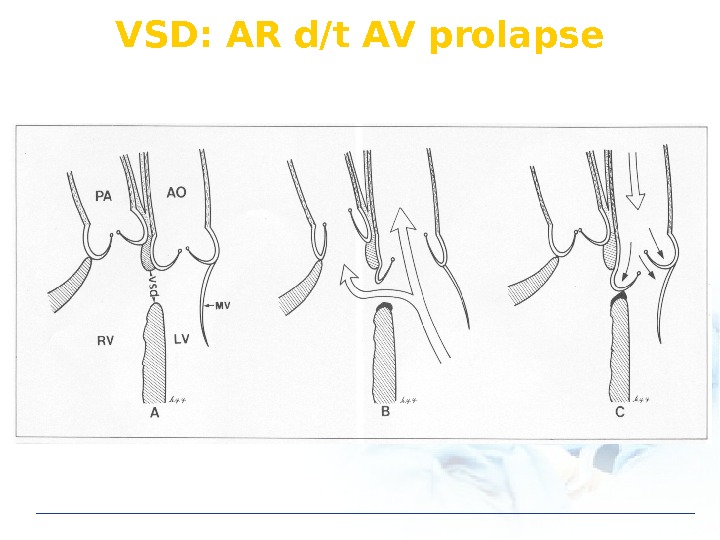
VSD: AR d/t AV prolapse
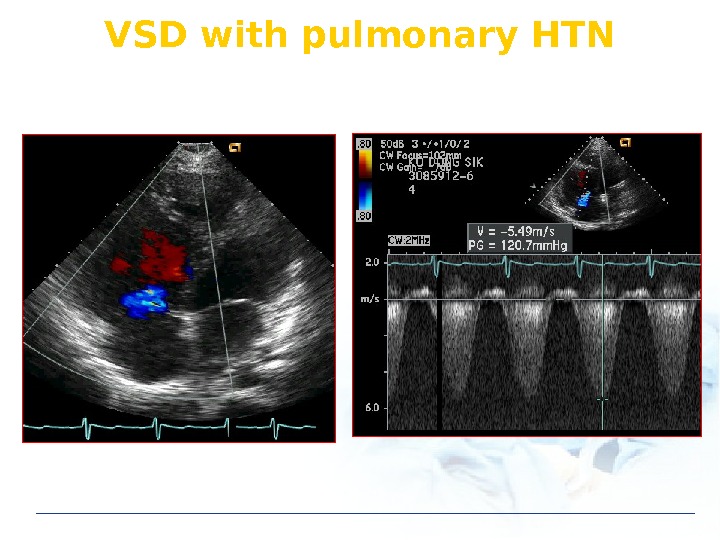
VSD with pulmonary HTN
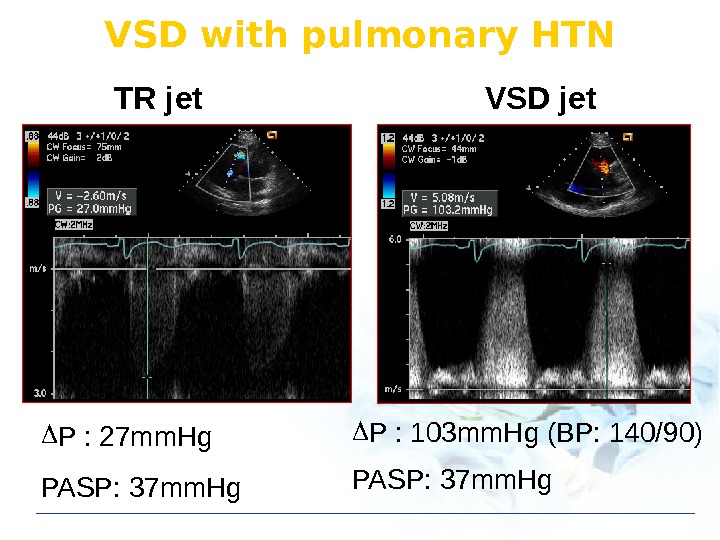
P : 27 mm. Hg PASP: 37 mm. Hg P : 103 mm. Hg (BP: 140/90) PASP: 37 mm. Hg. TR jet VSD jet. VSD with pulmonary HTN
VSD: Treatment Medical treatment Endocarditis prophylaxis: not recommended Surgical treatment Indication: Qp/Qs 1. 5 ~ 2. 0 Device closure Contraindication Severe pulmonary hypertension
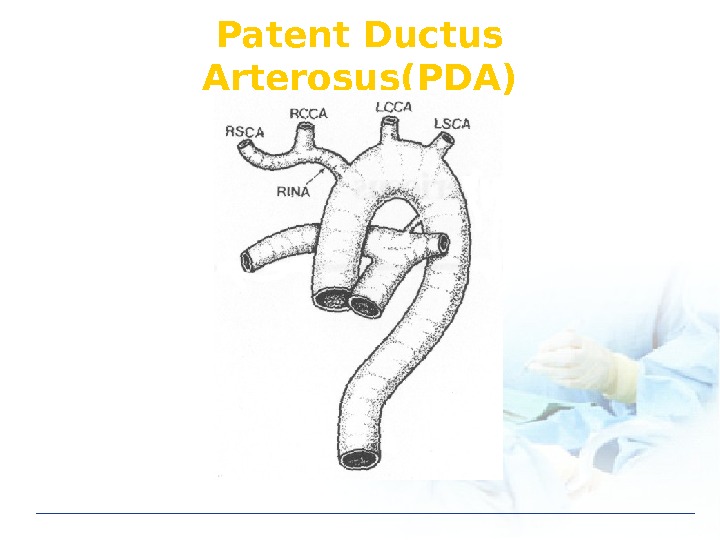
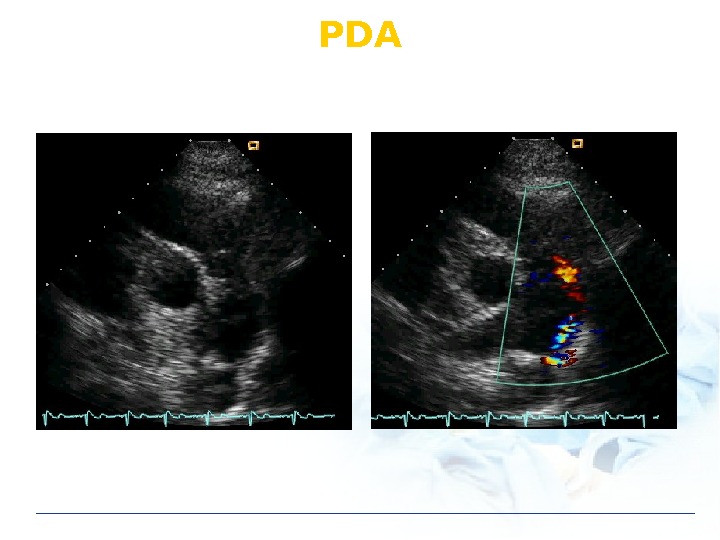
Patent Ductus Arterosus(PDA)
P
PDA: Physical Findings Continuous M Wide pulse pressure Differential cyanosis Rt to Lt shunt
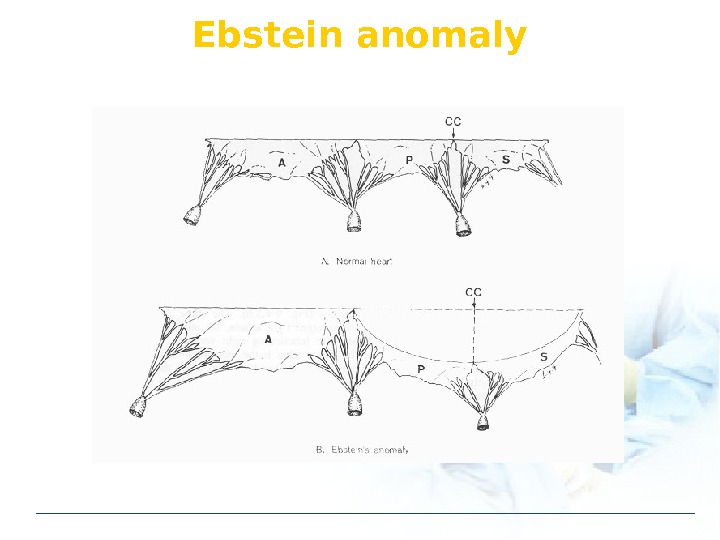
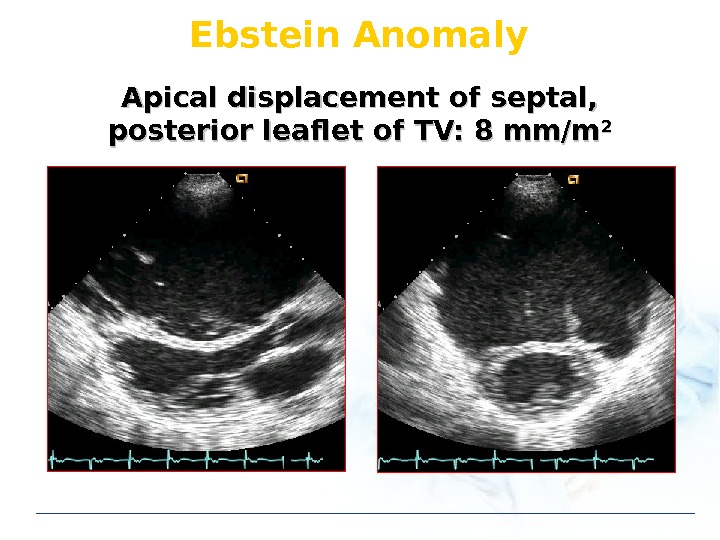
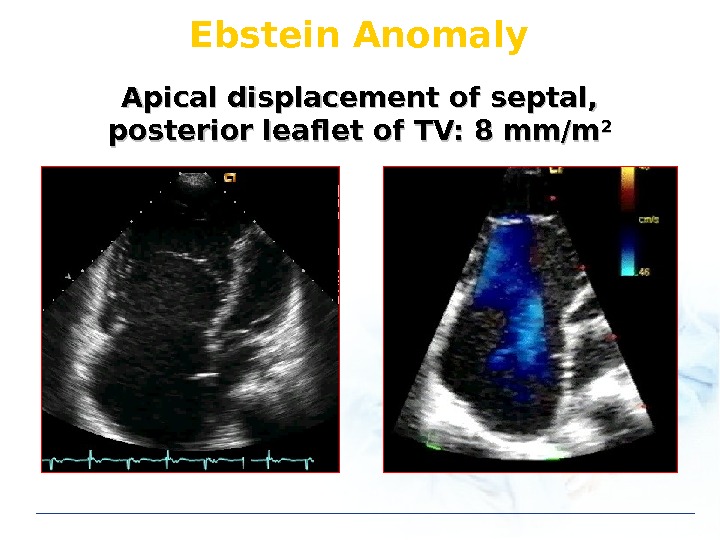
Ebstein anomaly
Ebstein Anomaly Apical displacement of septal, posterior leaflet of TV: 8 mm/m
Ebstein Anomaly Apical displacement of septal, posterior leaflet of TV: 8 mm/m
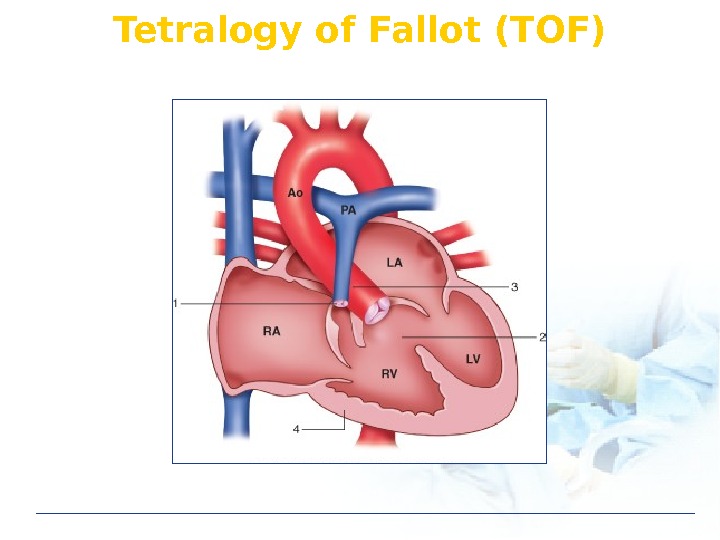
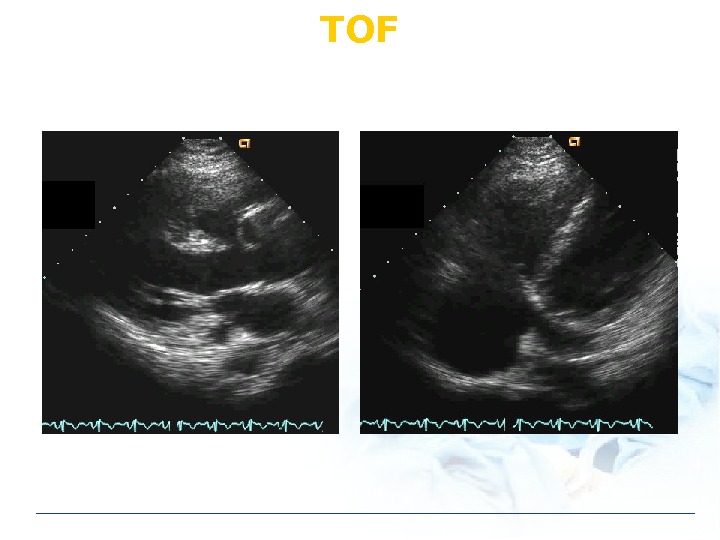
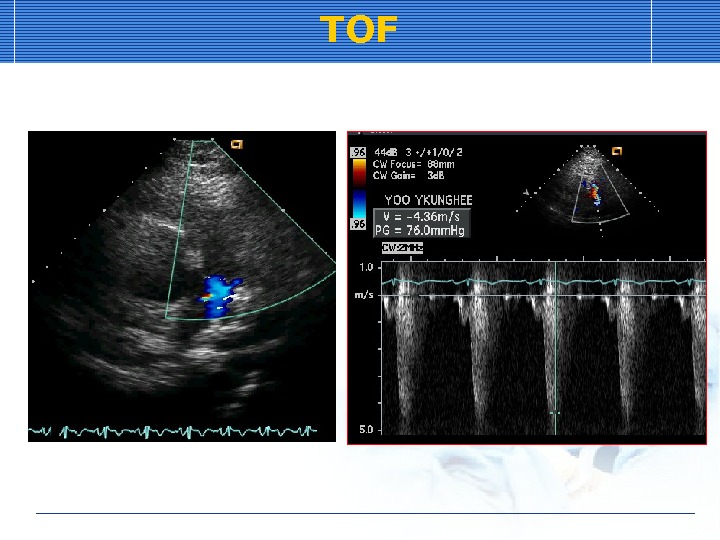
Tetralogy of Fallot (TOF)
TOF Ventricular septal defect Pulmonic stenosis Rt ventricular hypertrophy Overriding of aorta
TO
TO
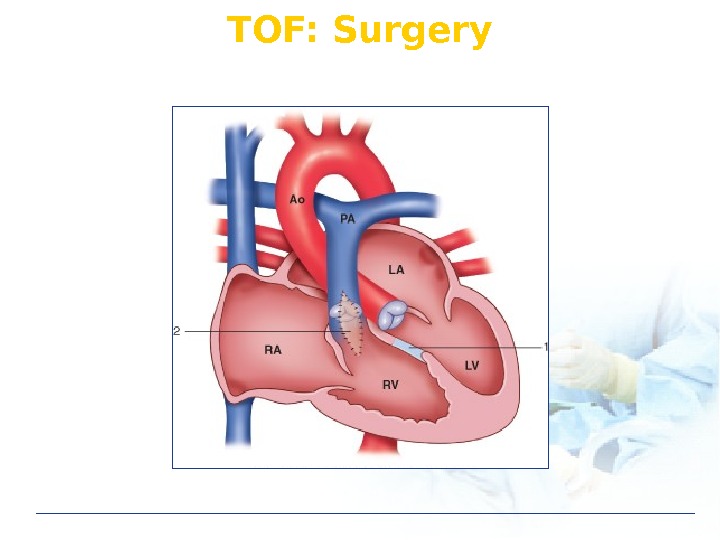
TOF: Surgery
Clinical Problems in CHD Heart failure Infective endocarditis Pulmonary hypertension (PHT) Eisenmenger syndrome
Eisenmenger Syndrome 1897: Vicktor Eisenmenger 32 yo woman with dyspnea, cyanosis Hemoptysis Autopsy: Large VSD 1958: Paul Wood “ Eisenmenger Syndrome”
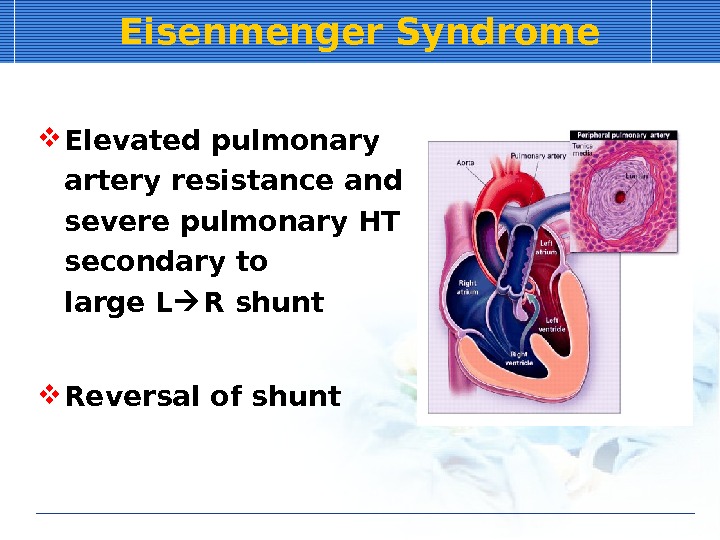
Eisenmenger Syndrome Elevated pulmonary artery resistance and severe pulmonary HT secondary to large L R shunt Reversal of shunt
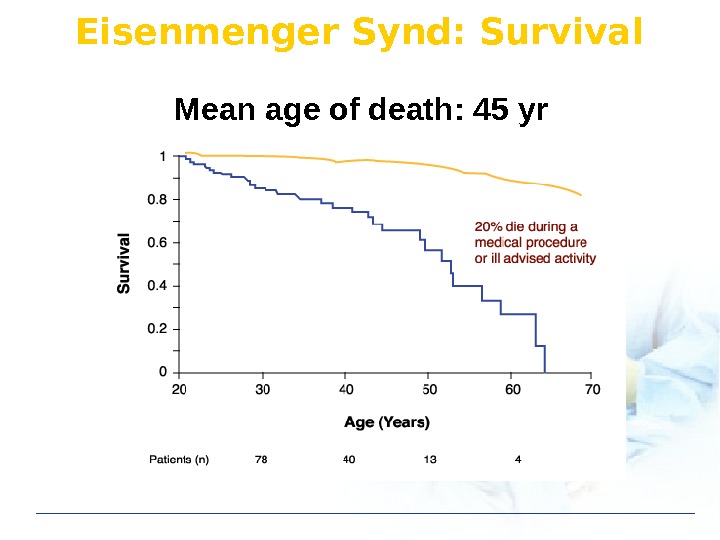
Eisenmenger Synd: Survival Mean age of death: 45 yr
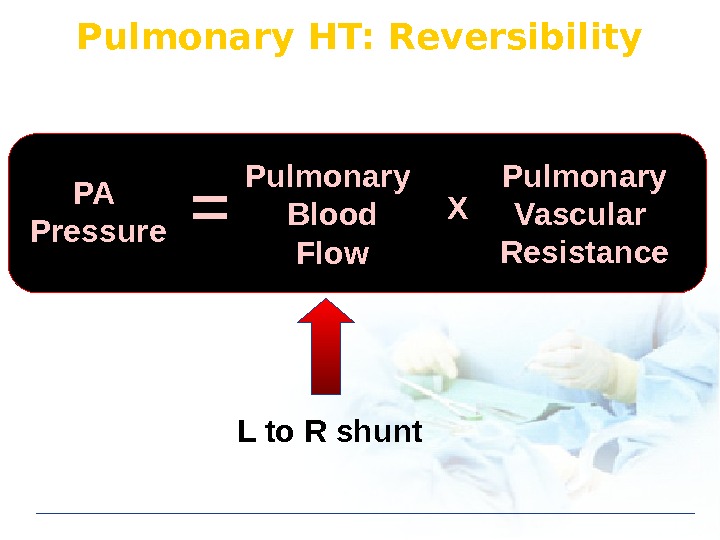
Pulmonary HT: Reversibility PA Pressure Pulmonary Blood Flow Pulmonary Vascular Resistance. X L to R shunt
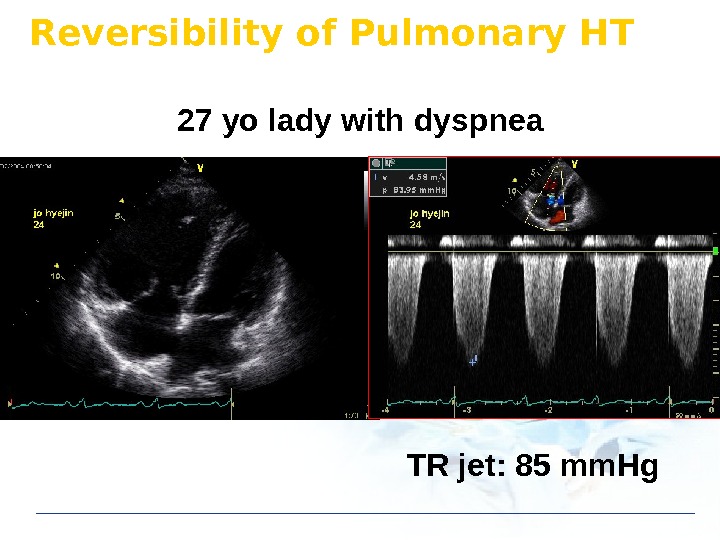
Reversibility of Pulmonary HT 27 yo lady with dyspnea TR jet: 85 mm. Hg
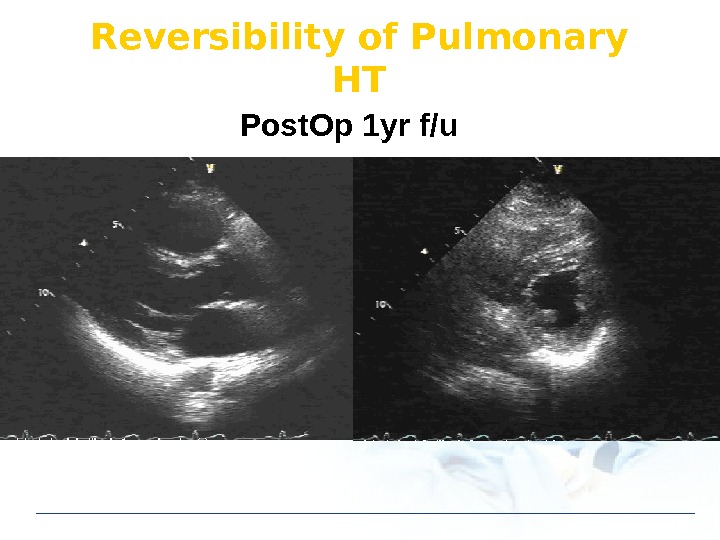
Reversibility of Pulmonary HT Post. Op 1 yr f/u
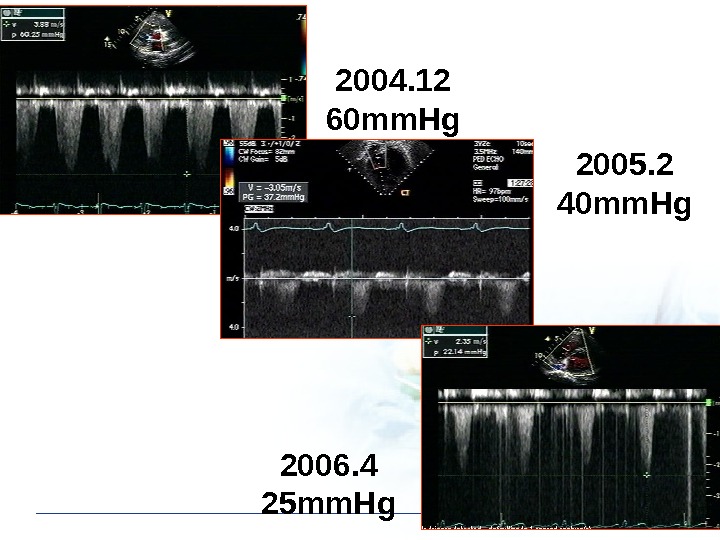
2004. 12 60 mm. Hg 2005. 2 40 mm. Hg 2006. 4 25 mm. Hg