08d1fdad215d0ed2e0a0f5826d49579d.ppt
- Количество слайдов: 101



Combating Tobacco Smoking Ann Mc. Neill, Ph. D Honorary Senior Lecturer Independent consultant in public health annmcneill@clara. co. uk

Sources: • www. treatobacco. net • www. ash. org. uk

A resource

Global smoking • There an estimated 1. 1 billion smokers worldwide, representing about a third of the adult global population • 800 m in developing countries and most of these are men (700 m) • In China there about 300 m smokers

World cigarette production Source: US Department of Agriculture

Who smokes?

Smoking since 1948

Smoking and deprivation % prevalence UK CIGARETTE SMOKING BY DEPRIVATION 80 70 60 1973 50 40 1996 30 20 10 0 0 1 2 3 4 5 Poorest Most affluent DEPRIVATION SCORE Jarvis (1997)
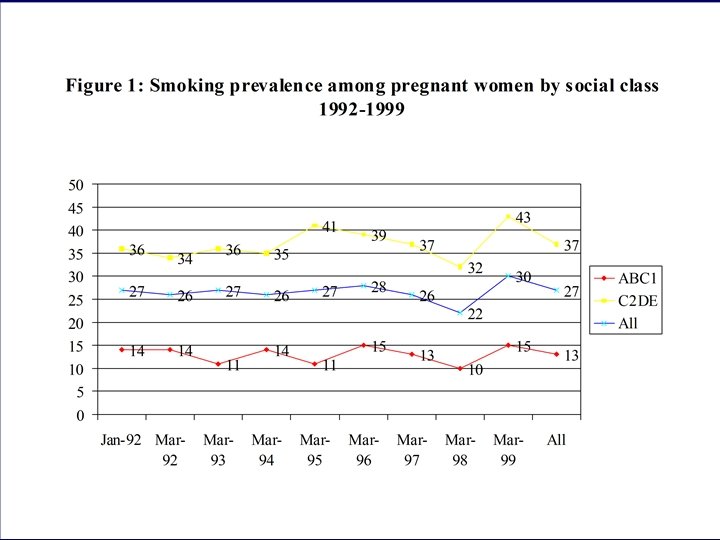

UK Smoking Summary • 28% men, 28% women smoked in 1996, decline in adults plateauing, possibly increasing again • No changes in young peoples’ smoking • No changes in pregnant womens’ smoking • Large socioeconomic differences

Some impacts - Health • Of those who smoke regularly, around one half will die prematurely • Smoking caused 120, 000 deaths in UK in 1995 • Smoking related diseases cost the NHS approx £ 1. 5 billion a year in England

Some impacts - Health • Cancer • Heart & Circulation • Respiratory • 20 fatal illnesses • 50 non-fatal illnesses • Widespread addiction

Health Impacts - Passive Smoking • Harm to others – 600 cases of Lung cancer – 12, 000 cases of heart disease – Trigger to 3. 4 million asthma sufferers – Pregnancy complications and cot death – 17, 000 hospital cases per year in under-5 s – 3 million non smokers work in smokey conditions

Cigarettes are among the leading causes of death in the United States 87% 82% 18% 40% (under 65) 21% (all ages) 33% 10% Source: 1989 Surgeon General's Report. Data from USA.

Annual Deaths from Smoking Compared with Selected Other Causes in the United States Sources: (AIDS) HIV/AIDS Surveillance Report, 1998; (Alcohol) Mc. Ginnis MJ, Foege WH. Review: Actual Causes of Death in the United States. JAMA 1993; 270: 2207 -12; (Motor vehicle) National Highway Transportation Safety Administration, 1998; (Homicide, Suicide) NCHS, vital statistics, 1997; (Drug Induced) NCHS, vital statistics, 1996; (Smoking) SAMMEC, 1995

Why do people smoke? • The tobacco industry • Most smoke because they are addicted to nicotine (affects nearly every organ) • Recent expert reports show that tobacco delivered nicotine is as addictive as heroin, cocaine etc • Most smokers want to quit but cannot

Key Findings • Tobacco dependence & withdrawal syndromes classified as substance use disorders under WHO ICD 10 • Nicotine dependence & withdrawal classified similarly under APA DSM IV • More common general term is addiction

Why it is so hard to stop smoking Rapid absorption of nicotine reinforces smoking behaviour Plasma nicotine (mg/m. L) 30 25 Cigarette 20 15 10 5 0 0 10 20 30 40 Time after smoking a cigarette (mins) 1. Royal College of Physicians, 2000. 50 60

Why it is so hard to stop smoking The power of addiction All smokers ~70% want to stop 1 ~2– 3% succeed in stopping each year 3 ~30% try each year 2 1. Bridgwood et al. , 2000. 2. West, 1997. 3. Arnsten, 1996.

Addiction “The cigarette should be conceived not as a product but as a package. The product is nicotine. …Think of the cigarette pack as a storage container for a day’s supply of nicotine. …Think of a cigarette as a dispenser for a dose unit of nicotine. Think of a puff of smoke as the vehicle of nicotine. … Smoke is beyond question the most optimised vehicle of nicotine and the cigarette the most optimised dispenser of smoke. ” • Philip Morris 1972
 •")
Reducing this public health burden • Preventing young people taking up smoking (prevention) • Encouraging smokers to stop (cessation) • Harm reduction approaches

Age at which smokers start US data 1991, Institute of Medicine

Unless Current Smokers Quit, Tobacco Deaths will Rise Dramatically in the Next 50 years Estimated cumulative tobacco deaths 1950 -2050 with different intervention strategies 520 Tobacco deaths (millions) 500 400 340 300 — — 220 200 190 — 100 70 0 1950 2000 2025 Baseline If proportion of young adults taking up smoking halves by 2020 If adult consumption halves by 2020 2050 Year World Bank. Curbing the epidemic: Governments and the economics of tobacco control. World Bank Publications, 1999. p 80.

Interventions • School health education • Restricting sales to minors • Advertising bans • Price rises • No smoking policies • Media & community-wide campaigns • Cessation interventions • Product modification

Assessing interventions • Efficacy • Effectiveness • Reach • Cost-effectiveness

Smoking Kills: A White Paper on Tobacco • To reduce smoking among children & young people • To help adults, especially the most disadvantaged, to give up • To offer particular help to pregnant women who smoke • (Lack of harm reduction apps)

Targets • To reduce smoking among children from 13% to 9% by 2010 (2005 -11%) • To reduce adult smoking from 28% to 24% by 2010 (2005 - 26%) • To reduce smoking among pregnant women from 23% to 15% by 2010 (2005 - 18%)

Prevention • Why do young people smoke? – sociodemographic variables – peer & sibling smoking – parental smoking & support – low academic achievement, alienation – rebelliousness – lack skills to resist offers, low self-esteem

Prevention • Why do young people smoke? – Many young smokers are already dependent on nicotine – They want to stop, have tried and failed – They inhale and take in substantial doses of nicotine from their cigs – Experimenters highly likely to become regular daily smokers

Prevention • Unanswered questions… – is there a minimum dosage of nicotine necessary – is daily use a prerequisite to dependence – are there gender/ethnic differences – are there genetic factors involved

Prevention • School programmes – health hazards did not affect smoking – social learning theory based programmes delay onset for 4 -10 years – when programmes implemented in real life they have been shown to be ineffective – comprehensive programmes dealing with range of health issues may be > effective

Prevention • Restricting sales to minors – laws rarely enforced - v expensive – young people still easily buy tobacco – evasion rife - ID card forgery, asking others to buy for them – a few intensive campaigns have worked, but divert attention from tobacco industry to retailers/children & drugs field shows inadequacy of supply issues

Illegal sales recommendations • Unpaid media to encourage retailers to comply with the law • Work with magistrates to encourage higher fines • Restrict retail outlets for tobacco? • Fine the industry rather than retailers for illegal sales

Advertising bans • Total ban on advertising, sponsorship, promotion is necessary • Tobacco industry circumvent partial bans • Some evidence that advertising bans reduce young people’s smoking • Govt reported showed advertising bans reduce cigarette consumption

How it works - part 1 Younger adult smokers are the only source of replacement smokers. . . If younger adults turn away from smoking, the industry must decline, just as a population which does not give birth will eventually dwindle. (RJ Reynolds, 1984)

How it works - part 2 A cigarette for the beginner is a symbolic act. I am no longer my mother's child, I'm tough, I am an adventurer, I'm not square … As the force from the psychological symbolism subsides, the pharmacological effect takes over to sustain the habit. (Philip Morris, 1969)

Examples of Marketing

Examples of Marketing

Appeal to kids

Tobacco sponsorship

Advertising bans • EU Directive adopted on 22 June 1998 struck down by European Court of Justice • UK enacting own ban following a private members bill which is currently going through the Houses of Parliament

Taxation • Price inversely related to consumption • May have an influence on young people’s smoking • UK has high tax policy • Goal - balance this with real support for those wanting to quit - hypothecation?

Price of 20 cigarettes in 2000 Price = £ 4. 14 Taxes = £ 3. 34

Affordability of cigarettes

EU tobacco taxation

Smuggling • Increased from 3% 96/97 to 22% 2000 • 80% containers, 20% white van • Loss to revenue £ 3. 8 bn • £ 35 m over three years to combat tobacco smuggling • Extra customs officers • Tougher penalites

Responses - Smuggling • Treat Smuggling as a criminal activity • Big Tobacco benefits from smuggling • Canadian Government is suing RJ Reynolds • The DTI is investigating BAT

No smoking policies • Growing evidence of effectiveness of workplace bans • Reduces passive smoking exposure • Associated with increases in productivity

UK approach • Voluntary action preferred over legislation • Public places charter developed with the hospitality industry, problem pubs • Approved Code of Practice (legal guidance for workplaces) stalled • Opposition DTI & DCMS

Public places charter The signatories to this Charter recognise that non-smoking is the general norm and that there should be increasing provision of facilities for non- smokers and the availability of clean air.
 80% target Source: NOP (1996) Smoking in public places:")
Workplaces with Smoking Policies (1995) 80% target Source: NOP (1996) Smoking in public places: 2 nd survey report

Approved Code of Practice • ACo. P is ‘quasi-legal’ like Highway Code • Gives meaning to Health & Safety at Work Act • Employers must take all reasonable and practicable steps to reduce or eliminate passive smoking exposure • Presumption in favour of banning smoking

Mass media & community campaigns • Effective in reducing adult smoking • Model = combination of both • Little effect with teenage smoking behaviour • Expensive • Unpaid publicity & media advocacy > cost-effective

Mass media & community campaigns • £ 50 m over 3 years for public education • Priority groups - young people, adults who want to quit, pregnant women • National media activity • Local involvement

Health Benefits of Smoking Cessation • Major & immediate health benefits for men and women of all ages whether or not they have smoking-related diseases • Former smokers live longer than continuing smokers • Decreases risk of lung & other cancers, heart attack, stroke, & COPD & can affect reproductive outcomes

Cessation interventions • Not routine - in spite of supporting evidence • Advice on smoking given to: – only 29% of smokers by GP (HEA, 1995) – only 39% of pregnant smokers (HEA, 1996)

Smoking cessation guidelines • Based on evidence from: – AHCPR Guidelines – Cochrane Centre Reviews • Evidence based evidence • Peer-reviewed and professionally endorsed

Smoking cessation guidelines • Raw M, Mc. Neill A, West R. Smoking Cessation Guidelines for Health Professionals. Thorax, 1998; 53 (Suppl 5, Part 1): S 1 -S 19 • West R, Mc. Neill A, Raw M. Smoking cessation guidelines for health professionals: an update. Thorax, 2000; 55: 987 -999.

Brief opportunistic advice Brief advice from a primary care physician during a routine consultation is effective in increasing the number of smokers stopping for at least 6 months West R, Mc. Neill A and Raw M. Thorax 2000; 55: 987 -999. Silagy C. Physician advice for smoking cessation. Cochrane Database Syst Rev 2002; 1.

Brief opportunistic advice • May trigger quit attempt in 40% of cases • Reduced effect with repeated exposure • Minimal effect on heavy smokers in absence of NRT/bupropion or beh suppt • GPs prefer to give to patients with smoking-related diseases but no greater in effect in this group West R, Mc. Neill A and Raw M. Thorax 2000; 55: 987 -999.

Face-to-face behavioural support • Behavioural support with multiple sessions of individual or group counselling aids smoking cessation, • Dose-response relationship between the amount of therapist-client contact and successful cessation West R, Mc. Neill A and Raw M. Thorax 2000; 55: 987 -999. USDHHS. Treating Tobacco use and dependence. A clinical practice guideline. Rockville, MD AHQR 2000. Lancaster T, Stead LF. Individual behavioural counselling for smoking cessation. Cochrane Database Syst Rev 2002; 1. Stead LF, Lancaster T. Group therapy for smoking cessation. Cochrane Database Syst Rev 2002; 1.

Face-to-face behavioural support West R, Mc. Neill A and Raw M. Thorax 2000; 55: 987 -999. USDHHS. Treating Tobacco use and dependence. A clinical practice guideline. Rockville, MD AHQR 2000.

Effect of smokers clinic Expected effect combining effect of medication with effect of behavioural support West R, Mc. Neill A and Raw M. Thorax 2000; 55: 987 -999.

Face-to-face behavioural support • Nurses can be effective where trained and employed for the purpose 1 • Specialist counselling for pregnant smokers is effective but brief midwife delivered advice probably is not 2 • There has been limited research on support for adolescent smokers, and no clear evidence 2 1. Rice VH, Stead LF. Cochrane Database Syst Rev 2002; 1. 2. West R, Mc. Neill A and Raw M. Thorax 2000; 55: 987 -999.

Self-help interventions Generic self-help interventions provided without personal support have a small effect on quit rates. Their impact is smaller and less certain than face-to-face interventions Lancaster T, Stead LF. Self-help interventions for smoking cessation. Cochrane Database Syst Rev 2002; 1. West R, Mc. Neill A and Raw M. Thorax 2000; 55: 987 -999.

Tailored vs. generic behavioural support material % Abstinent at 4 months There is some evidence that self-help materials tailored for the needs of individual smokers are more effective than standard materials Strecher VJ. Patient Educ Couns 1999; 36: 107 -117. Strecher VJ, et al. Journal of Family Practice 1994; 39(3): 262– 270.

Other support Telephone calls from a counsellor may be more effective than self-help materials alone West R, Mc. Neill A and Raw M. Thorax 2000; 55: 987 -999. USDHHS. Treating Tobacco use and dependence. A clinical practice guideline. Rockville, MD AHQR 2000.
 can be used instead of tobacco")
Nicotine replacement therapy • Nicotine replacement therapy (NRT) can be used instead of tobacco to aid quitting • NRT delivers nicotine without toxins from tobacco • NRT helps combat symptoms of withdrawal • Nicotine dose from NRT is lower & administered more gradually than with smoking and this reduces the addictive potential

Nicotine Replacement Therapy • Effectiveness of NRT does not depend on the amount of face-to-face behavioural support • All forms NRT appear to be similarly effective • Choice may be based on susceptibility to side effects, patient preference and availability • There is evidence that heavy smokers are more successful on 4 mg than 2 mg nicotine gum West R, Mc. Neill A and Raw M. Thorax 2000; 55: 987 -999. Silagy C, et al. Cochrane Database Syst Rev 2002; 1. USDHHS. Treating Tobacco use and dependence. A clinical practice guideline. Rockville, MD AHQR 2000.

Nicotine Replacement Therapy • There has been little research on combinations of different types of NRT • There is limited evidence that adding another form of NRT to the nicotine patch increases success rates West R, Mc. Neill A and Raw M. Thorax 2000; 55: 987 -999. Silagy C, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev 2002; 1. USDHHS. Treating Tobacco use and dependence. A clinical practice guideline. Rockville, MD AHQR 2000.
")
Plasma nicotine concentrations for smoking and NRT Increase in nicotine concentration ( ng/ml ) 14 12 10 8 Cigarette Gum 4 mg 6 Gum 2 mg 4 Inhaler Nasal spray Patch 2 0 5 10 15 Minutes 20 Source: Balfour DJ & Fagerström KO. Pharmacol Ther 1996 72: 51 -81. 25 30

NRT with limited behavioural support West R, Mc. Neill A and Raw M. Thorax 2000; 55: 987 -999. Silagy C, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev 2002; 1.

NRT with intensive support West R, Mc. Neill A and Raw M. Thorax 2000; 55: 987 -999. Silagy C, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev 2002; 1.

Importance of primary care The effectiveness of smoking cessation in primary care Intensive service with NRT Cessation rates (%) 20 15 Brief advice with NRT 10 5 No action Brief advice 0 Conservative figures; absolute cessation rates, CO validated; not one puff; throughout one year Reproduced and adapted with kind permission of Gay Sutherland John Stapleton of the Maudsley Hospital Smoking Cessation Clinic and the Institute of Psychiatry.

Pharmacotherapy Bupropion HCl SR acts on the neurotransmitters involved in nicotine addiction Modifies dopamine release in ‘reward’ pathway (mesolimbic system) Alters noradrenergic activity in ‘withdrawal’ pathway (locus coeruleus)

Bupropion is an effective aid to smoking cessation West R, Mc. Neill A and Raw M. Thorax 2000; 55: 987 -999. Hughes JR, et al. Antidepressants for smoking cessation. Cochrane Database Syst Rev 2000; 4.

Bupropion • Limited evidence from a single trial that bupropion is more effective than nicotine patch alone, and that a combination of bupropion and the patch is more effective than nicotine patch alone.

Pharmacotherapy Contraindications to bupropion HCl SR • Hypersensitivity to bupropion / excipients • Current/previous seizure or eating disorder • Known CNS tumour • Abrupt withdrawal from alcohol or benzodiazepines • Severe hepatic cirrhosis • Concomitant use with MAOIs • History of bipolar disorder

Acupuncture and Hypnotherapy • Acupuncture and hypnotherapy have not been shown to aid smoking cessation over and above any placebo effect White AR, et al. Acupuncture for smoking cessation. Cochrane Database Syst Rev 2002; 1. Abbot NC, et al. Hypnotherapy for smoking cessation. Cochrane Database Syst Rev 2002; 1. USDHHS. Treating Tobacco use and dependence. A clinical practice guideline. Rockville, MD: AHQR 2000.
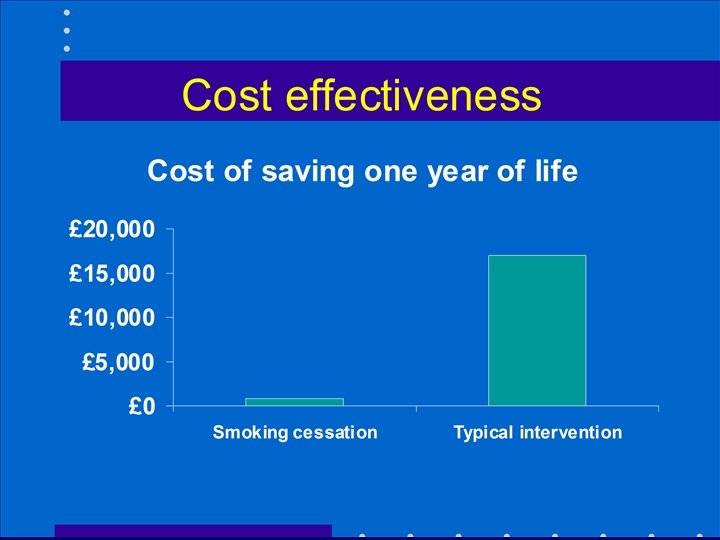

Cost-effectiveness of smoking cessation • Effect on other expenditures arising from the consequences of smoking • 87% with heart attack risk over 3% (the risk threshold used in Sheffield tables) are smokers • Stopping smoking would reduce the risk to below the threshold for statins prescribing for most patients

Cost effectiveness comparisons • Smoking cessation < £ 1, 000 • Statins £ 6, 000 -£ 13, 000 • Benchmark £ 30, 000?

NICE • Acknowledged the cost-effectiveness of smoking cessation • NRT and bupropion should be recommended for smokers who have expressed a desire to quit smoking

Assuming we meet our targets: • Reduce smoking rates among manual groups from 32% (1998) to 26% (2010) • This would still leave millions of smokers • Highly likely that prevalence would not decrease uniformly and that smoking prevalence would remain very high in most deprived groups

Assuming we meet our targets: • High prevalence among specific groups such as psychiatric populations, prison populations • Health effects of active smoking, passive smoking effects, role models. . • Still not offering a less harmful alternative for those that cannot or will not stop

What would a harm reduction policy look like? • Cigarette= dirty syringe • Focus on less harmful ways of using nicotine – make cigarettes less harmful – broaden access to NRT products – encouraging other forms of tobacco use which may be less harmful – encouraging other less harmful forms of nicotine delivery
 harm? – If it dissuaded some smokers")
Controversies? • Could it increase overall (population) harm? – If it dissuaded some smokers from quitting – If it attracted non-smokers? – If it encouraged ex-smokers to relapse • But can we deny individuals the right to use a less harmful product?

Harm reduction approaches • Low priority • Main changes last century were introduction of filters & low tar cigarettes • Danger - some have argued that consumption would be lower today if these products had not been introduced

Harm reduction approaches • Smokers compensate to maintain their nicotine levels • Tobacco industry exploited low tar by marketing as ‘light’, ‘mild’ etc

Harm reduction approaches • Could cigarettes be made less harmful? • Knowledge largely rests with tobacco industry • Cigarette is highly technical engineered product • But if effective, product modification would be beneficial to those who cannot stop (& improve inequalities) & could have beneficial internationally

Harm reduction approaches • Happening anyway - tobacco industry introducing new nicotine delivery devices • Smokeless tobacco - less harmful, but banned throughout EU except Sweden

Harm reduction approaches • Least harmful, most beneficial products most stringently regulated • Most toxic, lethal products (cigarettes) are hardly regulated at all • Regulation is upside down
 Regulation of")
NRT Regulation Critiques • Mc. Neill A, Foulds J, Bates C (2001) Regulation of nicotine replacement therapies (NRT): a critique of current practice. Addiction, 96: 1757 -68. • Mc. Neill A, Hendrie A (2001) Regulation of nicotine therapies: an expert consensus. WHO European Partnership Project, WHO Europe.

NRT Regulation Critiques • Pregnancy advice • Age restrictions • Smokers with cardiovascular disease • Use of NRT to reduce and control cigarette consumption – Use of NRT to support temporary abstinence – Reducing smoke intake from tobacco by allowing concomitant NRT use and smoking

NRT Regulation Critiques • Use for long-term maintenance • NRT combinations • Wider availability of NRT products • Possibility of tobacco competitive nicotine delivery devices for recreational use

NRT Regulation Critiques • Framework in which NRT is regulated: – does not properly weigh the risks and benefits of NRT use in situations in which its use is qualified, restricted or contraindicated – considers the risk of the medication but not the risks of failure to stop smoking
08d1fdad215d0ed2e0a0f5826d49579d.ppt