
Colonic polyps Made by: Islamova Sh. Group: 646


Colonic polyps Made by: Islamova Sh. Group: 646 P.

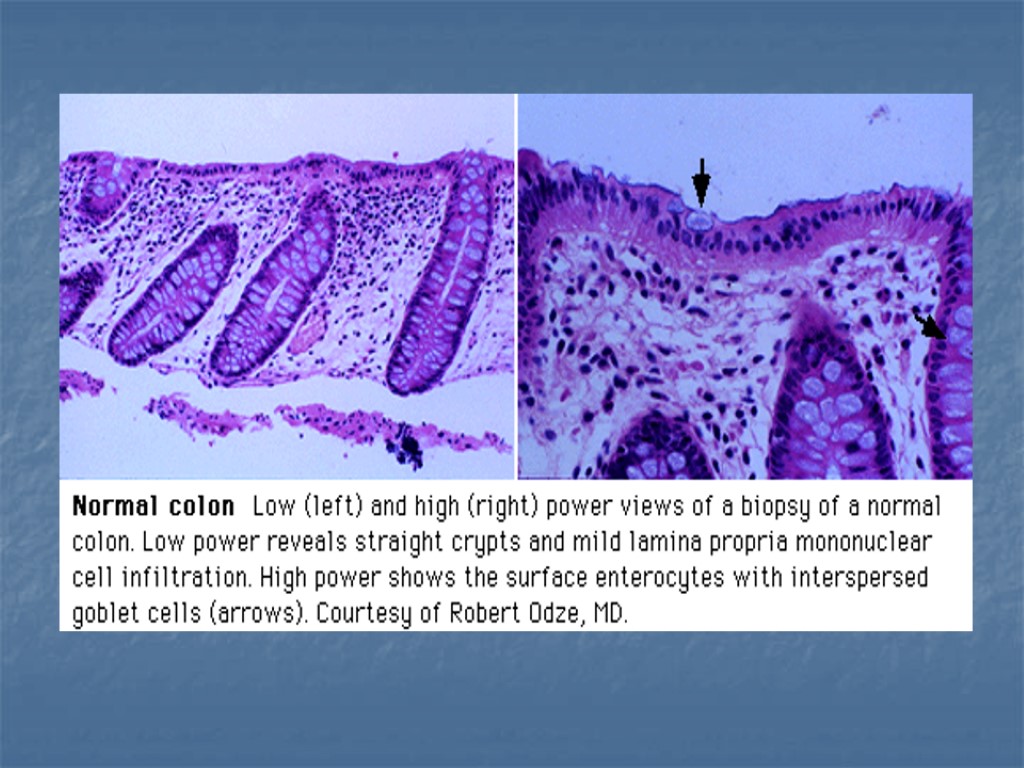
Background Polyps are slow-growing overgrowths of the colonic mucosa that carry a small risk (<1%) of becoming malignant. However, because polyps are highly prevalent in the general population (especially with increasing age), they confer an important predisposition to colon cancer and are therefore removed when detected. Patients with isolated polyps are usually asymptomatic. Polyps can occur as part of inherited polyposis syndromes in which their number is greater and the risk for malignant progression is much greater compared to the risk with isolated polyps.

Pathophysiology Colonic polyps, or adenomas, are benign epithelial neoplasms that arise from the epithelial cells lining the colon. Polyps are traditionally divided into 4 groups. Hyperplastic polyps. Adenomas. Polyposis syndromes. Miscellaneous.

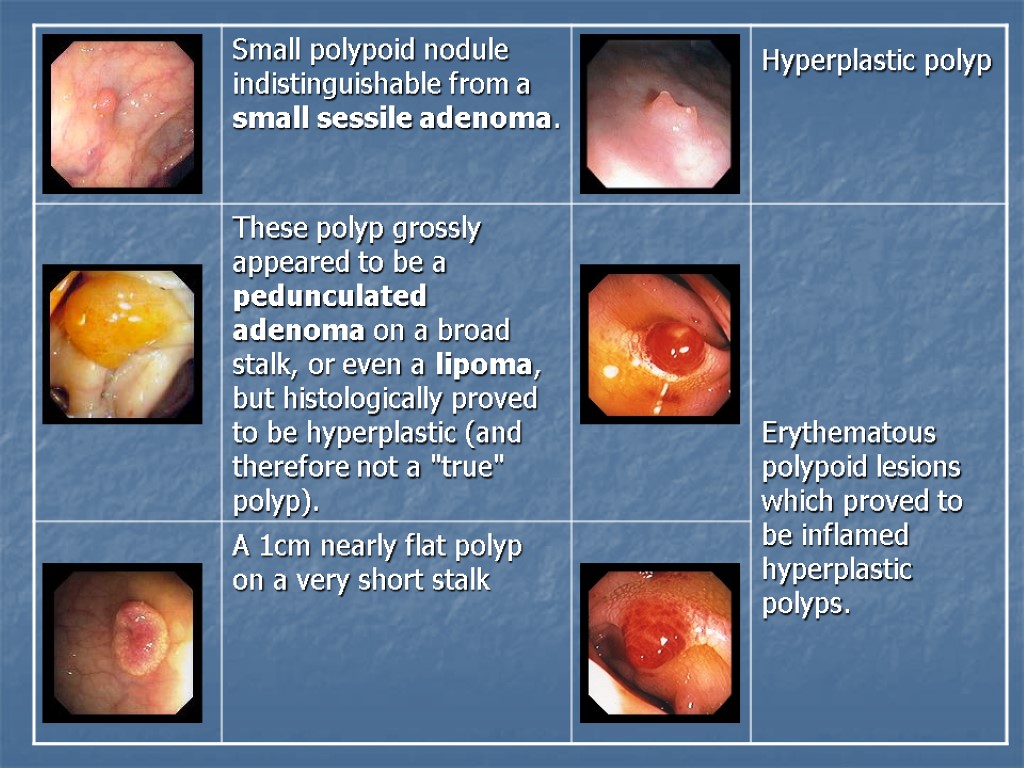
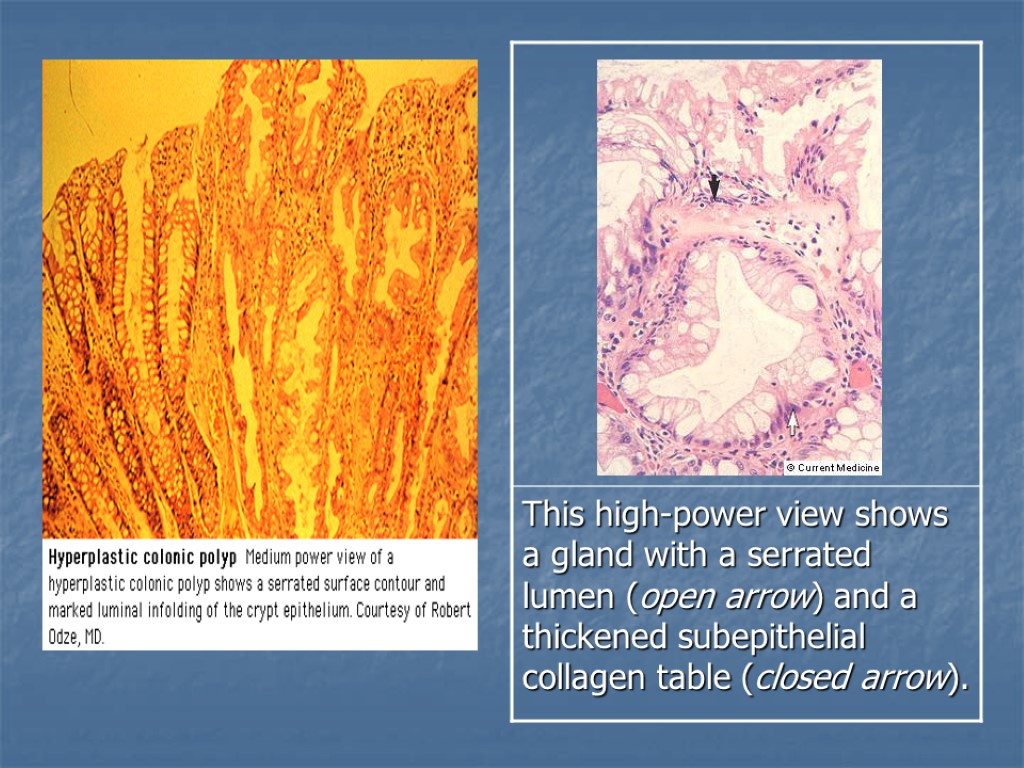
Hyperplastic polyps Hyperplastic polyps comprise about 90% of all polyps and are totally benign protrusions. They are usually less than 0.5 cm in diameter. They most commonly occur in the rectosigmoid region during adulthood. The lesions tend to be smaller than adenomas and do not appear to be related to the adenoma-carcinoma sequence.
 are small, usually less than")
Adenomas Adenomas comprise approximately 10% of polyps. Most (~90%) are small, usually less than 1.5 cm in diameter, and have a very small potential for malignancy. The remaining 10% of adenomas are larger than 1.5 cm and have about a 10% chance of containing invasive cancer. Adenomas are traditionally divided into 3 types: tubular, tubulovillous, and villous. Tubular adenomas are the most common of the 3 types and can be found anywhere in the colon.

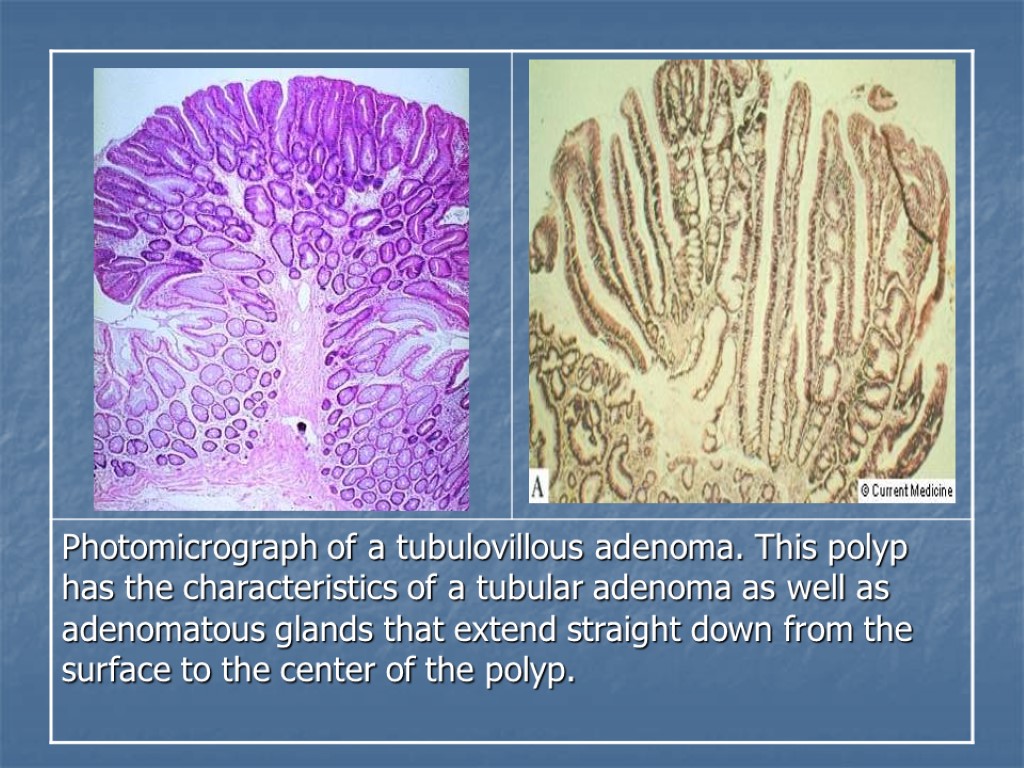
Those with a distinct stalk are termed pedunculated; those without a stalk are termed sessile. The risk of progression to carcinoma is related to the size of the adenoma. Tubulovillous adenomas are most commonly found in the rectal area. The degree of villous component of these adenomas is correlated with the risk of progression to carcinoma.

Villous adenomas most commonly occur in the rectal area. They tend to be larger than the other two types; and tend to be nonpedunculated, velvety, or cauliflower-like in appearance. Villous adenomas are associated with the highest morbidity and mortality rates of all polyps. They can cause hypersecretory syndromes characterized by hypokalemia and profuse mucous discharge and can harbor carcinoma in situ or invasive carcinoma more frequently than other adenomas.

Sessile Tubular Adenoma

Pedunculated Tubular Adenoma

Photomicrograph of tubular adenoma of the colon cut in cross section to demonstrate stalk. Tubular adenomas are characterized by a complex network of branching adenomatous glands.

Sessile Villous Adenoma

Villous adenoma. This lesion has a sessile configuration with a villi-form frond-like surface.

Serrated Adenoma Histologically this lesion was a mixture of hyperplastic and adenomatous elements, hence the designation of serrated adenoma.
. Gardner")
Polyposis syndromes Polyposis syndromes are hereditary conditions that include: Familial adenomatous polyposis (FAP). Gardner syndrome. Turcot syndrome. Peutz-Jeghers syndrome. Cowden disease. Familial juvenile polyposis. Some of the syndromes have extraintestinal features that help differentiate one syndrome from the other.
")
Familial adenomatous polyposis (FAP)
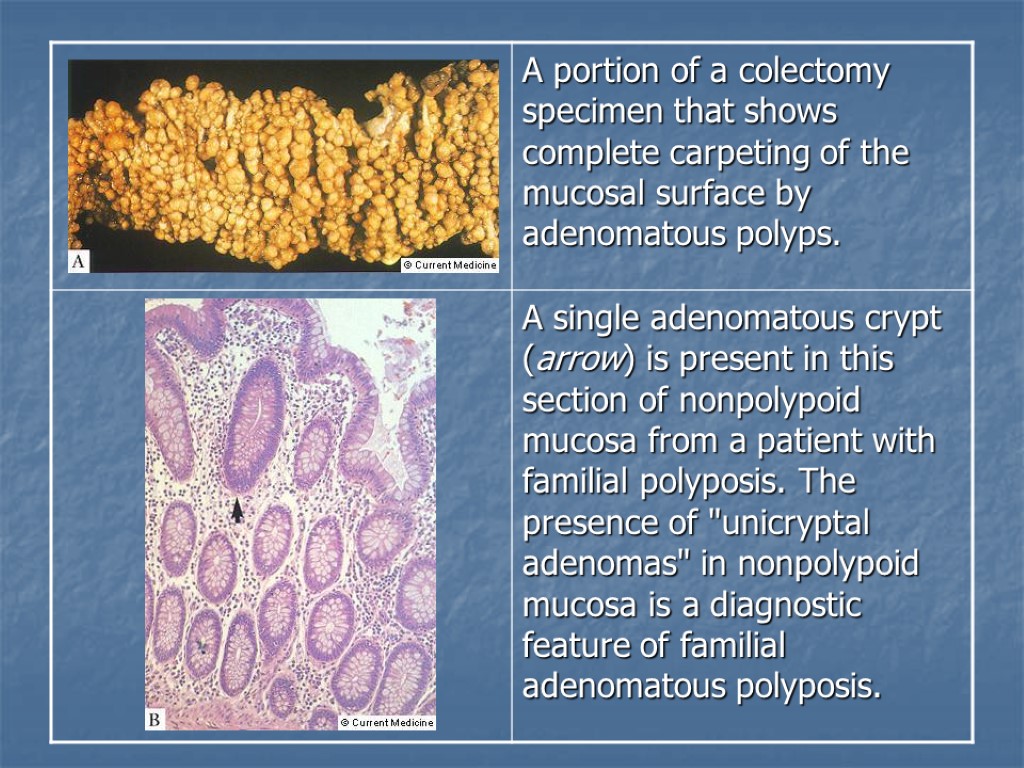
 Is the association of colonic adenomatous polyposis, osteomas, and soft tissue")
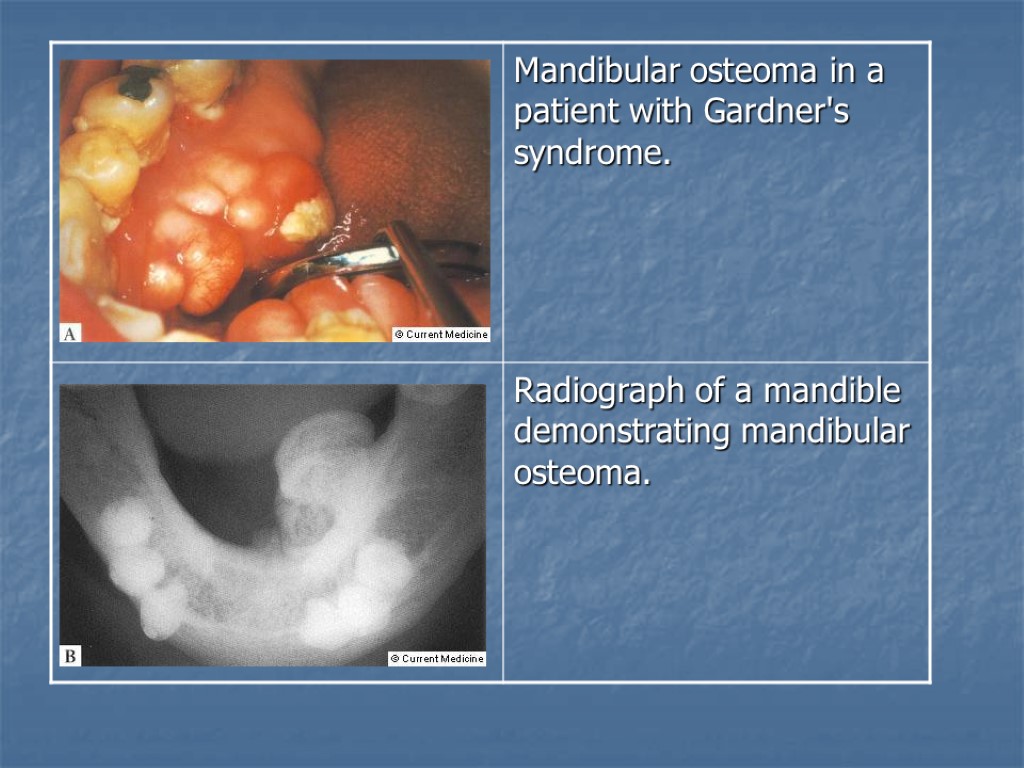
Gardner syndrome (GS) Is the association of colonic adenomatous polyposis, osteomas, and soft tissue tumors (epidermoid cysts, fibromas, desmoid tumors). Turcot syndrome Includes polyps, medulloblastoma, congenital hypertrophy of the retinal pigmented epithelium [CHRPE], and glioblastoma multiforme). Cowden syndrome Includes polyps, fibrocystic disease, breast cancer, and thyroid cancer).

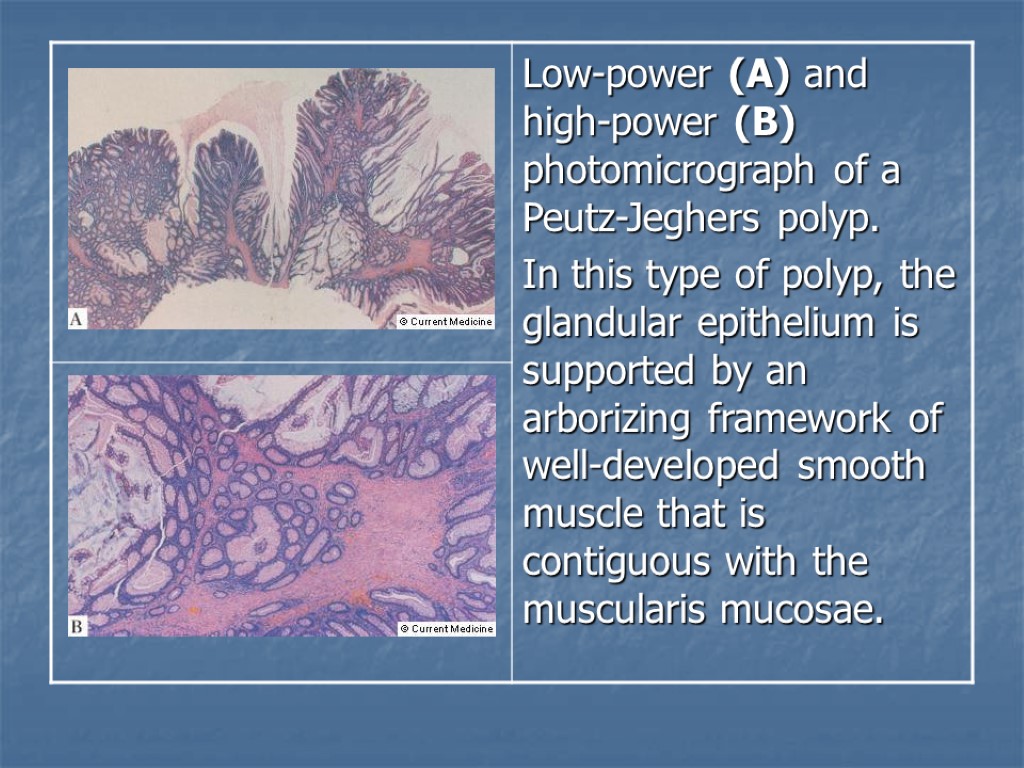
Peutz-Jeghers syndrome. Inherited in an autosomal dominant manner, PJS is characterized by the association of gastrointestinal polyposis and mucocutaneous pigmentation. Peutz-Jeghers type hamartomatous polyps are most prevalent in the small intestine (jejenum, ileum, and duodenum, respectively), but can occur elsewhere in the GI tract. Mucocutaneous hyperpigmentation presents in children under the age of five years as dark blue to dark brown mucocutaneous macules around the mouth, eyes, and nostrils, in the perianal area, on the buccal mucosa, and on the fingers.
, a benign")
Females are at risk for sex cord tumors with annular tubules (SCTAT), a benign neoplasm of the ovaries. Males occasionally develop calcifying Sertoli cell tumors of the testes, which secrete estrogen and can lead to gynecomastia. Individuals with Peutz-Jeghers syndrome are at increased risk for intestinal and extraintestinal malignancies, including colorectal, esophageal, gastric, breast, ovarian, and pancreatic cancers.

Mucocutaneous pigmentation in a patient with Peutz-Jeghers syndrome.
 Juvenile polyposis syndrome (JPS) is characterized by predisposition for hamartomatous")
Juvenile polyposis syndrome (JPS) Juvenile polyposis syndrome (JPS) is characterized by predisposition for hamartomatous polyps in the gastrointestinal (GI) tract, specifically in the stomach, small intestine, colon, and rectum. JPS is diagnosed if any one of the following is present: More than five juvenile polyps of the colorectum. OR Multiple juvenile polyps throughout the GI tract. OR Any number of juvenile polyps. and a Family history of juvenile polyps.

The term "juvenile" refers to the type of polyp, not the age of onset of polyps. Most individuals with JPS have some polyps by 20 years of age. Some individuals may only have four or five polyps over their lifetimes, whereas others in the same family may have over a hundred. Most juvenile polyps are benign; however, malignant transformation can occur. Estimates of developing GI cancers in families with JPS range from 9-50%.

Juvenile Polyp

Other hereditary syndromes Hereditary mixed polyposis syndrome Mode of inheritance is unknown. The syndrome is characterized by atypical juvenile polyps, polyps containing mixed histology, or multiple polyps of more than one histologic type in an individual. Neurofibromatosis type 1 (NF1) Individuals with NF1 may exhibit multiple intestinal polypoid neurofibromas or ganglioneuromas in the small bowel, stomach, and colon.

Ganglioneuromatosis. A proliferation of neural tissue within the mucosa. A ganglion cell is also present (arrow). This finding may be seen as an isolated polyp (eg, ganglioneuroma) or as a diffuse process throughout the gastrointestinal tract (eg, ganglioneuromatosis).
 It is an autosomal dominant colon cancer syndrome with")
Hereditary non-polyposis colon cancer (HNPCC) It is an autosomal dominant colon cancer syndrome with proximal colonic predominance. Few colonic adenomas are present. Other malignancies include cancer of the endometrium, ovary, stomach, small intestine, and urinary tract. It may be difficult to distinguish between HNPCC and attenuated FAP in individuals and families who have few adenomatous colonic polyps.

Acquired syndrome Cronkite-Canada syndrome Generalized gastrointestinal hamartomatous polyposis, cutaneous hyperpigmentation, hair loss, and nail atrophy.

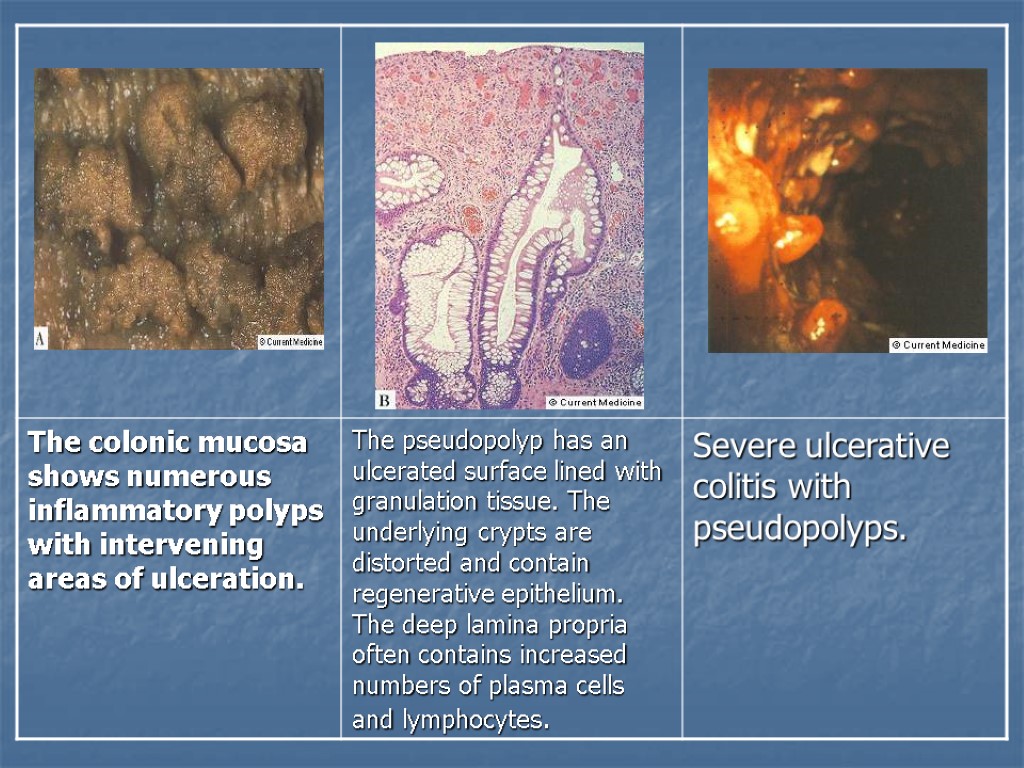
Miscellaneous Inflammatory polyps/ pseudopolyps These lesions develop as by-products of the ulcers that penetrate into the submucosa, leaving islands of adjacent regenerative mucosa. Although most common in ulcerative colitis, inflammatory polyps may also be seen in Crohn's disease, ischemia, and other ulcerative conditions of the colon.
")
Colonic Leiomyoma (Stromal Tumor)

A large area of pink whirling spindle cells is observed directly beneath the mucosa. The lesion has the typical appearance of a leiomyoma, complete with a well-circumscribed smooth border.

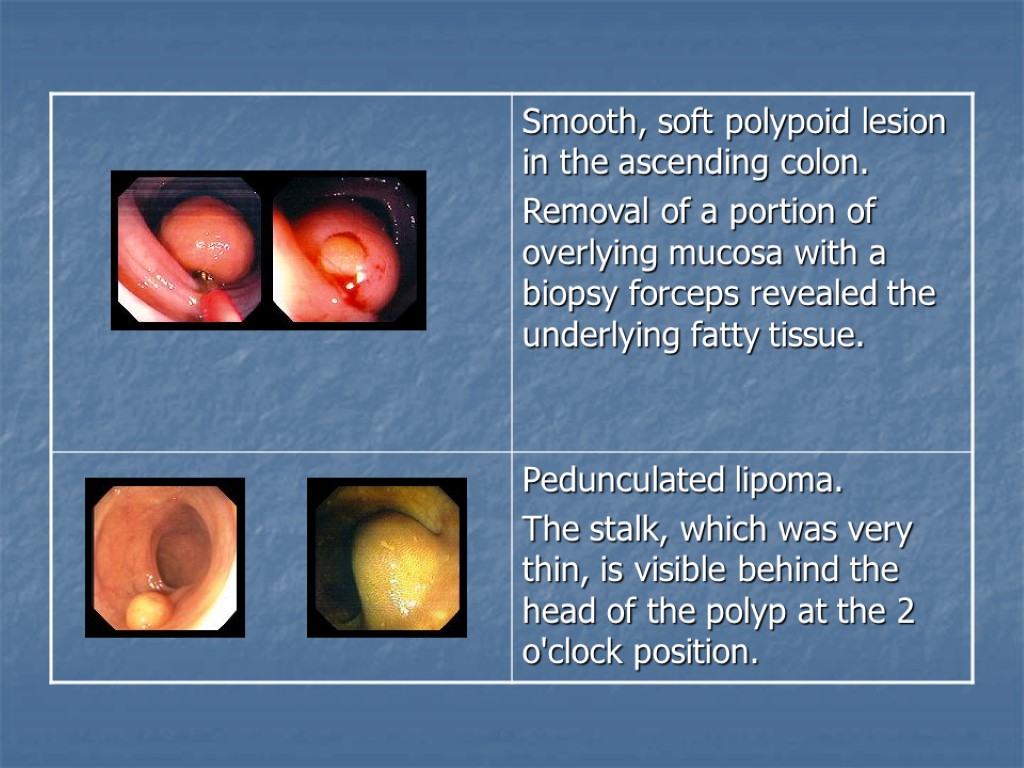
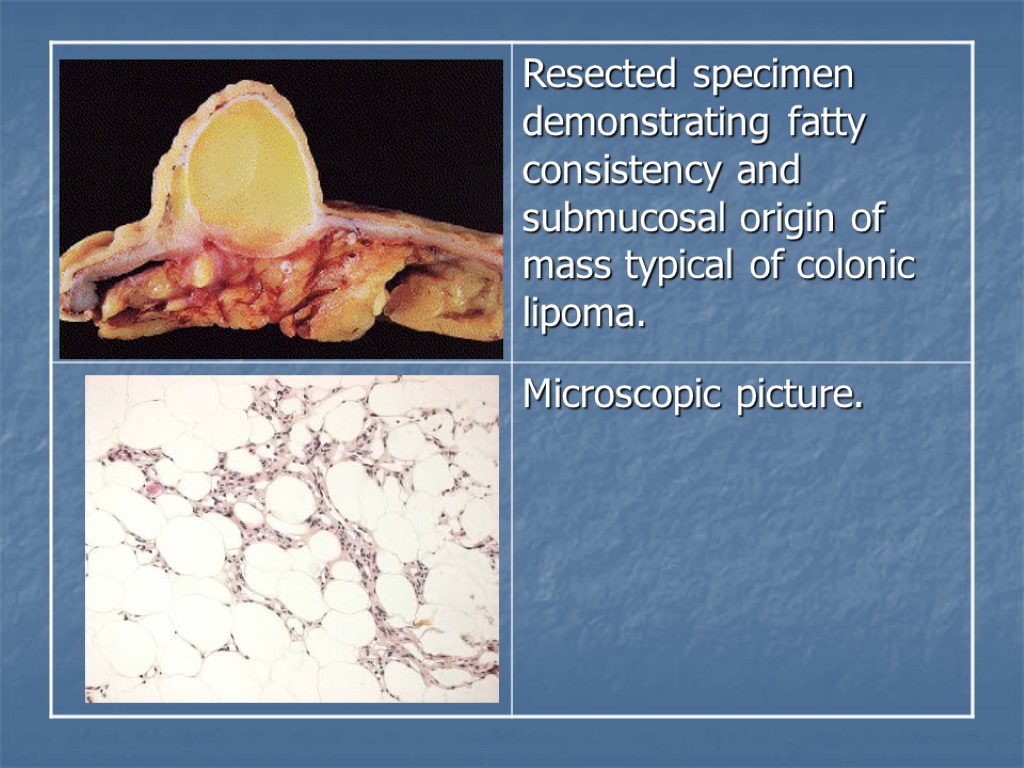
Colonic Lipoma Colon is the most common gastrointestinal site for lipomas: about 60-70% of all lipomas of the gastrointestinal tract originate in the colon. Ninety percent of colonic lipomas arise in the submucosa and 10% in the subserosa (appendices epiploicae). The size of colonic lipomas ranges between 1 and 10 cm in diameter, but most are smaller than 3 cm. They are usually solitary but can be multiple. The right side of the colon is involved more frequently than the left. The majority of noncomplicated colonic lipomas will not cause clinical complaints. However, recurrent intussusception of the tumour may cause intermittent abdominal pain whereas ulceration of the mucosa overlying the tumour may lead to intestinal blood loss.

Colonic Hamartoma

This low-power photomicrograph demonstrates a hamartomatous polyp with dilated mucus-filled glands and extensive edema and inflammation in the lamina propria. Hamartomas of the colon, small intestine, and stomach characterize familial juvenile polyposis. The risk of colon cancer is increased in this syndrome because of the presence of synchronous adenomatous polyps.

Lymphoid Hyperplasia

Fibroepithelial Polyp

Filiform polyps

Granular Cell Tumor

Diminutive Polyp

Rectal Condyloma

Lymphomatous polyposis Occurrence of primary extranodal lymphomas in the gastrointestinal tract. Two types include: Multiple lymphomatous polyposis. Mediterranean-type lymphoma.
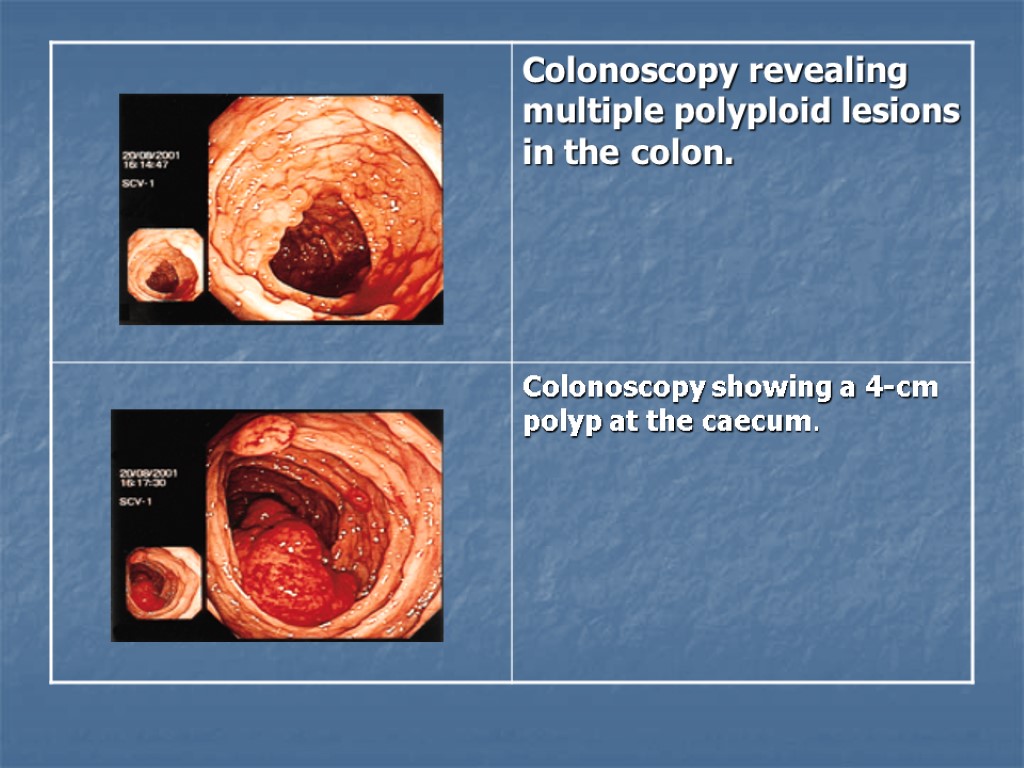

Figure 2. Colonoscopy with multiple polypoid lesions ranging from 0.2 to 0.5 mm in diameter. Mucosa between polyps appears to be normal. Figure 3. Colonoscopy with a sprayed dye technique (indigo carmine) showing multiple polypoid lesions of various sizes. Figure 4. Colonic biopsy specimen showing a dense lymphoid infiltrate with well-defined borders (hematoxylin-eosin, original magnification ×100).

Diagrammatic representation of carcinoma within a polyp. Black wedges represent foci of carcinoma. A wedges indicate carcinoma in situ; malignant cells do not traverse the muscularis mucosae. B wedges indicate invasive carcinoma; malignant cells have breached the muscularis mucosae.

Metastasis cascade. Metastasis of colorectal cancer cells from the primary site in the colon to the liver involves a complex series of events, all of which are necessary to result in distant metastatic disease. Tumors must become vascularized to grow at the primary site. Cells must then be able to invade basement membranes, avoid immune surveillance, adhere to vascular endothelia, and interact with the microenvironment to set up metastatic foci.

Thank you
colonic_polyps_-_waleed_fouad.ppt
- Количество слайдов: 54