f39fff366e600a28944aaa591e08be9a.ppt
- Количество слайдов: 47



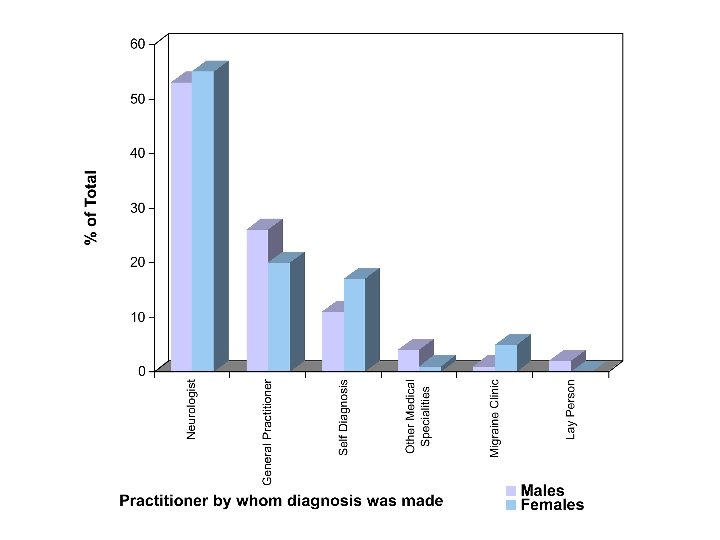
Cluster Headache 3 rd BIENNIAL HULL-BASH NATIONAL MEETING ON HEADACHE Anish Bahra The National Hospital for Neurology and Neurosurgery Whipps Cross University Hospital

Lifetime prevalence Tension-type headache ~ 60 -80% Migraine headache 15% Cluster Headache 0. 1%
 • Severe unilateral orbital, supraorbital and/or temporal pain")
IHS Classification for Cluster Headache (2004) • Severe unilateral orbital, supraorbital and/or temporal pain • Associated symptoms: – Conjunctival injection / Lacrimation – Nasal congestion / Rhinorrhea – Eyelid oedema – Forehead and facial sweating – Ptosis and Miosis – A sense of restlessness / agitation • 15 -180 minutes duration • 1 / alternate days – 8 /day

Cluster Headache – Defining features Strictly unilateral V 1 pain + Autonomic features Restlessness / agitation Short-duration / daily / bouts

% Cluster Headache – Laterality

Cluster Headache – Laterality %

Site of pain →V 1 • • • Retro-orbital Temporal Upper teeth Forehead Jaw Cheek % 92 70 50 46 45 45 Bahra A et al. Neurology 2002; 58: 354 -361 • • Lower teeth Neck Nose Ear Shoulder Vertex Occiput Parietal % 32 31 20 17 13 7 6 1

• • Retro-orbital Temporal Upper teeth Forehead V 1 V 2 V 1 • • • Jaw Cheek Lower teeth Neck Nose Ear Shoulder Vertex Occiput Parietal V 3 V 2 V 3 C 2/3 V 2 C 3/4 C 2 C 2

Autonomic Features %

Autonomic Features % CH – 98%1 Migraine – 25%2 1. Torelli, 2001 n=553 2. Obermann, 2007 n=841

Attack Duration and Frequency N CH Migraine Duration 15 -180 mins 4 -72 hrs Frequency 1 / day 1 -2 / month

Additional Features % CH Migraine

IHS Classification Criteria for Cluster Headache Episodic Cluster Headache → 90% 7 days - One year Pain-free interval ≥ one month Chronic Cluster Headache → 10% ≥ one year without remission ≥ one year with remissions one month
 and")
Cluster Headache Attack Provocation • 1 mg s/l nitroglycerine provocation • During (n=28) and out (n=15) of active bout • Attack precipitated in ALL during active bout • No attack precipitated out of the bout Ekbom, K. Arch Neurol 1968; 19: 487

Cluster Paroxysmal Headache hemicrania 3: 1 1. 5: 1 Episodic: Chronic 90: 10 35: 65 10: 90 Attack Duration 15 -180 mins 2 -30 mins 5 -250 s 1 -8/day > 5 /day 1/day to 30/hr 90% 80% 65% Present Rare Absent ++ + – M: F Attack Frequency Restlessness Periodicity Alcohol Trigger SUNCT

Cluster Headache & Imaging • All patients ?

Symptomatic Cluster Headache • Aneurysm of the ACA • Pituitary tumour • AVM of the occipital lobe • Vertebral artery aneurysm • Meningioma of the cervical canal (C 2)

Symptomatic Cluster Headache • Aneurysm of the ACA • Pituitary tumour • AVM of the occipital lobe • Vertebral artery aneurysm • Meningioma of the cervical canal (C 2)

Symptomatic Cluster Headache • Typical or atypical • Response to treatment ≡ Primary CH • ± Resolution with Rx of precipitating pathology

Symptomatic Cluster Headache • Phenotype • Rx Response Cannot differentiate b/u Primary & Secondary CH

Any one → Sensitivity 98. 6% Likelihood Ratio Age > 50 years* 2. 34 Sudden Onset* 1. 74 Predictors of Secondary Headache Abnormal neurological examination* 3. 56 Additional Features 2. 27 Locker at al. Headache. 2006 ( n = 558) / Ramirez-Lassepas. Arch Neurol. 1997

Cluster Headache & Imaging • All patients ? → Need Data • New onset • Primary CCH • Atypical history • + Systemic / neurological features

Therapeutics

ABORTIVE THERAPY : SUMATRIPTAN S/C Ø The Sumatriptan Cluster Headache Study Group -1991 Success: 74% Sumatriptan 26% Placebo Ø Modest further benefit from 12 mg Ø 2 & 3 mg are effective Ø No prophylactic benefit Ø Long term - Well tolerated. Ø No tachyphylaxis / MOH

ABORTIVE THERAPY : OXYGEN Double-blind cross-over comparison of oxygen 100% inhalation with air 12 l / min for 15 minutes ( n=76) * Success: 78% Oxygen 20% Placebo Ø Recommendation : 7 – 12 l/min for 15 minutes CONCLUSION : Safest treatment but impractical Fogan, 1985. / Cohen, 2007*

ABORTIVE THERAPY Sumatriptan 20 mg IN Zolmitriptan 5 and 10 mg po Lidocaine IN

ABORTIVE THERAPY Sumatriptan 20 mg IN Zolmitriptan 5 and 10 mg IN Response at 30 minutes Zolmitriptan 5 and 10 mg po Lidocaine IN

ABORTIVE THERAPY : LIGNOCAINE IN Double-blind placebo controlled cross-over study Lignocaine 10% Intranasal ( n = 9) 37 ± 7. 8 mins Lignocaine } p < 0. 01 59. 3 ± 12. 3 mins Placebo } A/Es – Unpleasant taste. Adequate self- administration 4% Lignocaine solution 3 -4 drops intranasally Costa et. Al (2000) Cephalalgia ; 20 : 85

PREVENTATIVE THERAPY Multiple daily attacks → Prophylaxis

PREVENTATIVE THERAPY : VERAPAMIL • 240 -480 mg daily – Lethargy • Up to 1200 mg daily • Start at 80 mg tds • 40 -80 mg increments every 10 -14 days – Constipation – Pedal oedema – Bradycardia • ECG monitoring every two weeks Leone et al. (2000) Neurology ; 54 : 1382
 Dose ±SD Patients on VPM")
Verapamil in Cluster Headache Arrhythmias No Patients Mean VPM(mg) Dose ±SD Patients on VPM 217 512 ± 279 ECGs 108 587 ± 264 1° Heart Block 13 578 ± 264 Other HB 9 604 ± 260 Total arrhythmias 21 567 ± 290 PR ≤ 0. 2 s 9 653 ± 275 Cohen, 2007
 Dose ±SD Total 108 591 ± 264 Heart Rate")
Bradycardia No Patients Mean VPM(mg) Dose ±SD Total 108 591 ± 264 Heart Rate (mean) 66 Bradycardia 39 659 ± 253 53 Bradycardia → Stop VPM 4 495 ± 172 49
 Rhythm Junctional (after Lithium")
Arrhythmias in patients on VPM + Other Drug Lithium 5(1) Rhythm Junctional (after Lithium stopped) Methysergide 1(1) 1° Heart Block (after Methysergide stopped) Triptans 49(8) 1° HB (6), 2° HB (1), Junctional (1)

PREVENTATIVE THERAPY : METHYSERGIDE • 3 -6 mg : Increase in one week • Then 1 mg / week – Nausea and vomiting – Abdominal discomfort – Vasoconstrictive effects – Fibrosis • Up to 12 mg daily • BNF – 6 months then drug holiday Weight gain Muscle cramps Mood changes

PREVENTATIVE THERAPY : LITHIUM • 300 -1500 mg Tremor – Level at 4/7 after dose change GI side effects – Weekly until dose constant for 4 weeks ↓ thyroid, euthyroid goitre – Then 3 monthly Ataxia, nystagmus, dysarthria • 0. 7 -1. 2 mmol/l Diabetes Insipidus • Normal renal function and Na+ (Li toxicity) Drowsiness, confusion, seizures

ABORTIVE THERAPY : CORTICOSTEROIDS Short-term use for multiple daily attacks Attacks recur once the dose is decreased • 40 -80 mg for 5 – 7 days • Taper thereafter over 2 weeks • Simultaneously introduce a suitable prophylactic Jammes (1975) Dis. Nerv. Syst. ; 36 : 375

Preventative Therapy • Verapamil – 1200 mg daily. ECG monitoring • Methysergide – 12 mg daily. Avoid > 6/12 use • Lithium – 300 -1500 mg ( Level 0. 7 -1. 2 mmol/l) • Steroids – 40 -80 mg. Max. 2 /52. Interim measure ð Other considerations → Topiramate / Melatonin / Sodium Valproate / Gabapentin / Ergotamine

SURGICAL THERAPY • Trigeminal ganglion and nerve • Sphenopalatine ganglion • Greater superficial petrosal nerve • Nervus intermedius • Greater Occipital Nerve • Hypothalamus

Greater Occipital Nerve Block

Greater Occipital Nerve Block Patients N=23 Treatment Group Placebo Complete response at 1/52 11 None Complete response at 4/52 8 None Ambrosini et al. Pain (2005) Patients (N) No. Injections Complete response (N) Partial Response (N) 19 22 10 3 AUDIT. Afridi et al. Pain 2006
 Mo since Subjective Estimated Patient ONS outcome Change %")
Occipital Nerve Stimulation Duration (yrs) Mo since Subjective Estimated Patient ONS outcome Change % Recommend Triptan Use 1 7 23 Same - No Same 2 6 27 Same - Yes Same 3 6 11 Improved 95 Yes Less 4 17 17 Improved 60 Yes Less 5 13 27 Improved 20 -80 Yes Same 6 24 8 Improved 90 Yes Less 7 13 11 Improved 25 Yes Same Burns, The Lancet (2007)
 Lancet ; 352 : 275 VBM May")
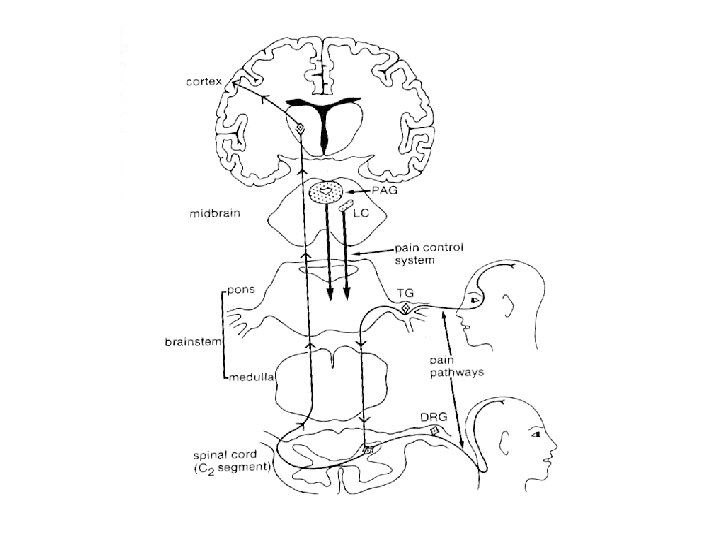
CLUSTER HEADACHE PET May et al. (1998) Lancet ; 352 : 275 VBM May et al. (1999) Nat. Med; 5: 836

Cluster Headache - Stereotactic Stimulation of the Posterior Hypothalamic Gray Matter May et al. (1998) Lancet ; 352 : 275 Leone et al. (2001) NEJM ; 345 : 1428

Cluster Headache Sumatriptan 6 mg sc High flow oxygen IN Sumatriptan / IN or Po Zolmitriptan IN Lidocaine Verapamil Methysergide Lithium Topiramate Corticosteroids Local V / Upper Cervical nerve block Local V / Upper Cervical neurostimulation Central neurostimulation
f39fff366e600a28944aaa591e08be9a.ppt