

c2e96f5a25f7f470cdb29dfd9ce7eac7.ppt
- Количество слайдов: 38
 CHIPRA QUALITY DEMONSTRATION GRANT:
CHIPRA QUALITY DEMONSTRATION GRANT:
 South Carolina chose categories: CHIPRA Measures: Category A – Experiment with, and evaluate the use of, new measures for quality of Medicaid/ CHIP children’s health care EHRs: Category B – Promote the use of Health Information Technology (HIT) for the delivery of care for children covered by Medicaid/CHIP Medical Home/Behavioral Health: Category C – Evaluate provider-based models which improve the delivery of Medicaid/CHIP children’s health care services 2
South Carolina chose categories: CHIPRA Measures: Category A – Experiment with, and evaluate the use of, new measures for quality of Medicaid/ CHIP children’s health care EHRs: Category B – Promote the use of Health Information Technology (HIT) for the delivery of care for children covered by Medicaid/CHIP Medical Home/Behavioral Health: Category C – Evaluate provider-based models which improve the delivery of Medicaid/CHIP children’s health care services 2
 3
3
 The South Carolina grant has four key goals: Quality: demonstrate that newly developed quality measures can be successfully utilized in pediatric practices; Technology: share key clinical data through a statewide electronic quality improvement network; Innovation: develop a physician-led, peer-to-peer quality improvement network; and Pediatrics: expand the use of pediatric medical homes to address mental health challenges of children in our state. 4
The South Carolina grant has four key goals: Quality: demonstrate that newly developed quality measures can be successfully utilized in pediatric practices; Technology: share key clinical data through a statewide electronic quality improvement network; Innovation: develop a physician-led, peer-to-peer quality improvement network; and Pediatrics: expand the use of pediatric medical homes to address mental health challenges of children in our state. 4
 From the Beginning February 2010 – June 2012 5
From the Beginning February 2010 – June 2012 5
 Beginning to Now February 2010 – June 2012 • • • Staff, Contractors and 18 Practices Selected HIT and reporting development Baseline data gathering Blog and tracking mechanisms MOAs/Contracts 3 Learning Collaborative sessions 6
Beginning to Now February 2010 – June 2012 • • • Staff, Contractors and 18 Practices Selected HIT and reporting development Baseline data gathering Blog and tracking mechanisms MOAs/Contracts 3 Learning Collaborative sessions 6
 Quality Measures February 2010 – June 2012 – Introduced 11 of 24 quality core measures – SC received approval American Board of Pediatrics (ABP) to offer MOC credits on 9 of our quality measures: - Access ADHD Access Behavioral Health Services Developmental Screening - Emergency Dept. Use Family Centered Care Oral Health Well Child Visits (all) Goal: to demonstrate that newly developed quality measures can be successfully utilized in pediatric practices
Quality Measures February 2010 – June 2012 – Introduced 11 of 24 quality core measures – SC received approval American Board of Pediatrics (ABP) to offer MOC credits on 9 of our quality measures: - Access ADHD Access Behavioral Health Services Developmental Screening - Emergency Dept. Use Family Centered Care Oral Health Well Child Visits (all) Goal: to demonstrate that newly developed quality measures can be successfully utilized in pediatric practices
 Electronic Health Records/ Quality Reporting • 18 practices use 10 different EMR operating systems • Historical data downloaded from 4 practices • Driver customization completed with 2 operating systems • Aim: to extract data from 9 of QTIP practices by the end of summer 2012 • Working on data quality review and report design • Aim: reports to select practices October 2012 GOAL: share key clinical data through a statewide electronic quality improvement network
Electronic Health Records/ Quality Reporting • 18 practices use 10 different EMR operating systems • Historical data downloaded from 4 practices • Driver customization completed with 2 operating systems • Aim: to extract data from 9 of QTIP practices by the end of summer 2012 • Working on data quality review and report design • Aim: reports to select practices October 2012 GOAL: share key clinical data through a statewide electronic quality improvement network
 Patient Centered Medical Homes • Implementing PCMH concept using NCQA standards • Standards 1, 2, 5, 6 presented • July 2012 Learning Collaborative focusing on NCQA - PCMH – 1 practice received PCMH – level 3 (2008) certification – At least 3 are actively working on applications. • At least 3 practices have “parent partners” Goal: Implement pediatric medical homes to address the mental health needs
Patient Centered Medical Homes • Implementing PCMH concept using NCQA standards • Standards 1, 2, 5, 6 presented • July 2012 Learning Collaborative focusing on NCQA - PCMH – 1 practice received PCMH – level 3 (2008) certification – At least 3 are actively working on applications. • At least 3 practices have “parent partners” Goal: Implement pediatric medical homes to address the mental health needs
 Integrated Mental Health • 3 practices piloting the CHADIS software system • Actively exploring UMASS training • 52 on-site visits and 11 community mixers occurred • April 1 st , behavioral health carved into managed care • AAP Mental Health Practice Readiness Inventory assessment conducted Goal: Implement pediatric medical homes to address the mental health needs
Integrated Mental Health • 3 practices piloting the CHADIS software system • Actively exploring UMASS training • 52 on-site visits and 11 community mixers occurred • April 1 st , behavioral health carved into managed care • AAP Mental Health Practice Readiness Inventory assessment conducted Goal: Implement pediatric medical homes to address the mental health needs
 AAP’s Mental Health Practice Readiness Inventory Results Total Scores ranged from 5079 with an average score of 64 out of 96 possible. Average scores ranged from 80% of the total possible in the health care financing domain to 58% in the clinical information systems/ delivery system redesign.
AAP’s Mental Health Practice Readiness Inventory Results Total Scores ranged from 5079 with an average score of 64 out of 96 possible. Average scores ranged from 80% of the total possible in the health care financing domain to 58% in the clinical information systems/ delivery system redesign.
 Academic Detailing: 2011 - ADHD – 129 practitioners participated in the initial visit; 82 practitioners, in the follow-up visit. – 28 practitioners received CEU certificates 2012 – ASTHMA - As of June 30 th 133 practitioners from 16 practices have participated in the initial on-site visit. 12
Academic Detailing: 2011 - ADHD – 129 practitioners participated in the initial visit; 82 practitioners, in the follow-up visit. – 28 practitioners received CEU certificates 2012 – ASTHMA - As of June 30 th 133 practitioners from 16 practices have participated in the initial on-site visit. 12
 Evaluation: Measuring Quality Improvement • Process • Analysis of successes/challenges, PDSA and QI • Partner interviews – Lessons Learned • Outcomes • CHIPRA quality measures (baseline, CY 2011, annually) • Individual practice quality measure reports based on administrative claims data until EMR data exchange • CAHPS: results provided (baseline CY 2010, CY 2011) • Practice characteristics and movement toward PCMH and Integrated behavioral health • National Evaluation – MHI, claims analysis 13
Evaluation: Measuring Quality Improvement • Process • Analysis of successes/challenges, PDSA and QI • Partner interviews – Lessons Learned • Outcomes • CHIPRA quality measures (baseline, CY 2011, annually) • Individual practice quality measure reports based on administrative claims data until EMR data exchange • CAHPS: results provided (baseline CY 2010, CY 2011) • Practice characteristics and movement toward PCMH and Integrated behavioral health • National Evaluation – MHI, claims analysis 13
 February 2011 – June 2012 54 Technical Assistance visits by Dr. Rushton Spring 2012 • 17 on-site visits • 178 pediatric staff participated • 7 peer reviewers Previous visits: • 180 staff - Fall 2011 • 228 staff - Spring 2011 14
February 2011 – June 2012 54 Technical Assistance visits by Dr. Rushton Spring 2012 • 17 on-site visits • 178 pediatric staff participated • 7 peer reviewers Previous visits: • 180 staff - Fall 2011 • 228 staff - Spring 2011 14
 Let’s not forget …… • National Evaluators - March 2012 • Quality Improvement Specialist hired • MOC Part IV – Credits earned by 10 doctors in 4 QTIP practices for their work on ADHD (2011) – 3 doctors have earned credits in 2012 • 121 Postings and 70 comments on the blog between January and June 2012 15
Let’s not forget …… • National Evaluators - March 2012 • Quality Improvement Specialist hired • MOC Part IV – Credits earned by 10 doctors in 4 QTIP practices for their work on ADHD (2011) – 3 doctors have earned credits in 2012 • 121 Postings and 70 comments on the blog between January and June 2012 15
 Progress… What Did You Do? 16
Progress… What Did You Do? 16
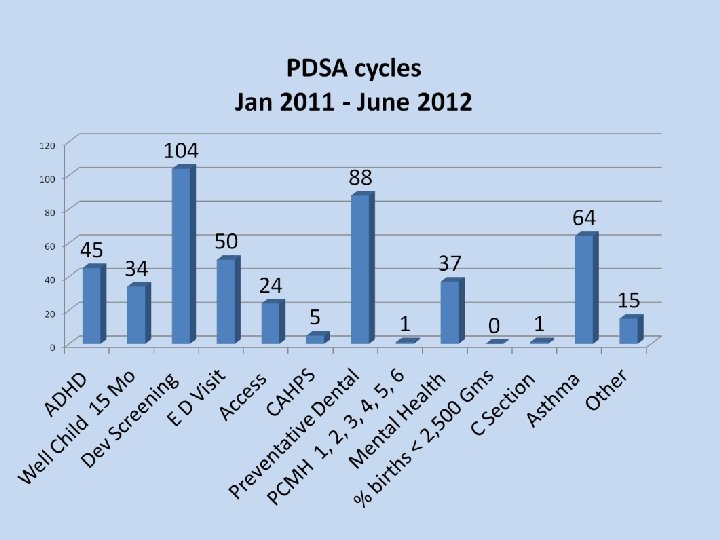
 What did you do? Quality - To Date: Collection of CHIPRA Quality Measures – As of June 30, 2012, 468 PDSA cycles have been documented from January 2011 to June 2012. – 188 of these were documented for work completed between January - June 2012. • Most frequent PDSA topic: Asthma 17
What did you do? Quality - To Date: Collection of CHIPRA Quality Measures – As of June 30, 2012, 468 PDSA cycles have been documented from January 2011 to June 2012. – 188 of these were documented for work completed between January - June 2012. • Most frequent PDSA topic: Asthma 17
 Quality WHAT DID YOU DO? UPDATE Quality improvement team within the pediatric setting – Over 350 quality meetings documented from January 2011 to July 2012. – 144 meetings were documented between January to June 30, 2012. 19
Quality WHAT DID YOU DO? UPDATE Quality improvement team within the pediatric setting – Over 350 quality meetings documented from January 2011 to July 2012. – 144 meetings were documented between January to June 30, 2012. 19
 What We Noticed 20
What We Noticed 20
 Successes Increased responsiveness, communication and sharing among QTIP practices MOC has added value Fully engaged contractors and Planning and Steering members, and QTIP practices. Early results from both practices and outcomes are showing improvement. Learning Collaborative appears to be a good method to disseminate information and share ideas. 21
Successes Increased responsiveness, communication and sharing among QTIP practices MOC has added value Fully engaged contractors and Planning and Steering members, and QTIP practices. Early results from both practices and outcomes are showing improvement. Learning Collaborative appears to be a good method to disseminate information and share ideas. 21
 Observations: • PDSA documentation often corresponds with site visits. • Mid-summer/mid-grant fatigue • Work occurs that’s not documented. • Evidence of QTIP in offices: bulletin boards, posters, newsletters, awards …. • Correlation between QI activities and reimbursement. • Increased communication and sharing among QTIP practices. 22
Observations: • PDSA documentation often corresponds with site visits. • Mid-summer/mid-grant fatigue • Work occurs that’s not documented. • Evidence of QTIP in offices: bulletin boards, posters, newsletters, awards …. • Correlation between QI activities and reimbursement. • Increased communication and sharing among QTIP practices. 22
 Decreasing Emergency Department Utilization: • 12 practices developed fliers outlining ER criteria • 1 practice reported a decrease of 395 ED visits over a 3 month period in 2011 & 2012 – Strategies included: open access including lunch & late clinic appointments; new patient information sheets; and targeted anticipatory guidance. • 12 Practices have documented at least 1 PDSA cycle on ED
Decreasing Emergency Department Utilization: • 12 practices developed fliers outlining ER criteria • 1 practice reported a decrease of 395 ED visits over a 3 month period in 2011 & 2012 – Strategies included: open access including lunch & late clinic appointments; new patient information sheets; and targeted anticipatory guidance. • 12 Practices have documented at least 1 PDSA cycle on ED
 Decreasing Emergency Department Utilization: Challenges: • Difficulty retrieving ED utilization data from hospitals • Found one-time information to families on emergency vs non-emergency treatment inadequate; must keep reinforcing • At times, face resistance
Decreasing Emergency Department Utilization: Challenges: • Difficulty retrieving ED utilization data from hospitals • Found one-time information to families on emergency vs non-emergency treatment inadequate; must keep reinforcing • At times, face resistance
 Oral Health 88 PDSA cycles QTIP Focus: 1. 2. 3. 4. Perform an oral health risk assessment between 12 - 36 months Referral to a dental home Apply fluoride varnish to high risk patients between 12 - 36 months Discuss fluoride in the family’s drinking water source Other Corresponding PDSA cycles 13 28 27 16 4
Oral Health 88 PDSA cycles QTIP Focus: 1. 2. 3. 4. Perform an oral health risk assessment between 12 - 36 months Referral to a dental home Apply fluoride varnish to high risk patients between 12 - 36 months Discuss fluoride in the family’s drinking water source Other Corresponding PDSA cycles 13 28 27 16 4
 Oral Health Results: • 184 QTIP practice staff trained to administer fluoride varnish; 14/18 QTIP practices are now eligible to provide fluoride varnish. • An 80% increase in fluoride varnish application (D 1206) (as of April 2012 and compared with 2011) • One practice reported an 54% increase in oral health screenings at the 6 mo. visit and an 22% increase with 2 yr. olds referrals to a dentist. • Increased collaborative with DHEC on oral heath toolkits and water testing.
Oral Health Results: • 184 QTIP practice staff trained to administer fluoride varnish; 14/18 QTIP practices are now eligible to provide fluoride varnish. • An 80% increase in fluoride varnish application (D 1206) (as of April 2012 and compared with 2011) • One practice reported an 54% increase in oral health screenings at the 6 mo. visit and an 22% increase with 2 yr. olds referrals to a dentist. • Increased collaborative with DHEC on oral heath toolkits and water testing.
 Oral Health Innovations: • Using Reach Out and Read book “Brush, Brush” • A Dental Summit was hosted by one practice to educate the community on early childhood dental disease. • Goodie bags with toothbrushes • Giving patients stickers instead of candy • Providing families a list of local dentists • Templates in EMR
Oral Health Innovations: • Using Reach Out and Read book “Brush, Brush” • A Dental Summit was hosted by one practice to educate the community on early childhood dental disease. • Goodie bags with toothbrushes • Giving patients stickers instead of candy • Providing families a list of local dentists • Templates in EMR
 Mental Health Innovations: • Community mixers to increase awareness of local resources • Increased awareness and use of Teen Screen • PDSA cycles include: – assessment of post partum depression – piloting CHADIS – exploring integrating mental health worker and/or screening tools into adolescent well child visits – exploring decreasing length of time between physician referral and MH visit Challenges • Knowledge of and/or availability of resources • Cumbersome authorization process for services • DHHS carved in mental/behavioral health into Managed Care (April 2012)
Mental Health Innovations: • Community mixers to increase awareness of local resources • Increased awareness and use of Teen Screen • PDSA cycles include: – assessment of post partum depression – piloting CHADIS – exploring integrating mental health worker and/or screening tools into adolescent well child visits – exploring decreasing length of time between physician referral and MH visit Challenges • Knowledge of and/or availability of resources • Cumbersome authorization process for services • DHHS carved in mental/behavioral health into Managed Care (April 2012)
, Stono, and Barnwell’s willingness to pilot CHADIS") Above and Beyond: • Carolina Pediatrics (Columbia), Stono, and Barnwell’s willingness to pilot CHADIS • Stono explored pre-existing asthma and ADHD protocols • Expansion of Project Breathe Easy: – Rock Hill – Beaufort collaborative effort • Caroline Currin’s willingness to pilot IFS’s PCMH assessment, and assist with share info • … and many, many more……. 29
Above and Beyond: • Carolina Pediatrics (Columbia), Stono, and Barnwell’s willingness to pilot CHADIS • Stono explored pre-existing asthma and ADHD protocols • Expansion of Project Breathe Easy: – Rock Hill – Beaufort collaborative effort • Caroline Currin’s willingness to pilot IFS’s PCMH assessment, and assist with share info • … and many, many more……. 29
 Challenges Ø NCQA PCMH level 3 certification for small practices may be unrealistic Ø Discipline in documenting work done by the practices Ø Internal practice barriers: including practice “buy-in” and turnover in lead QTIP staff… Ø EMRs: frustration with systems; competing priorities; constant changes… Ø Practices have multiple priorities: QTIP, MCO, Meaningful Use… Ø Receptive of information/resources – but often are slow incorporating new information into office processes 30
Challenges Ø NCQA PCMH level 3 certification for small practices may be unrealistic Ø Discipline in documenting work done by the practices Ø Internal practice barriers: including practice “buy-in” and turnover in lead QTIP staff… Ø EMRs: frustration with systems; competing priorities; constant changes… Ø Practices have multiple priorities: QTIP, MCO, Meaningful Use… Ø Receptive of information/resources – but often are slow incorporating new information into office processes 30
 Where we are going 31
Where we are going 31
 Year 3 Remaining Tasks July 2012 – January 2013 • Learning Collaboratives – Introducing additional quality measures – NCQA – PCMH standards • Technical assistance site visits conducted between September – December 2012 – Dr. Rushton and QTIP team – SCORx. E: second round visits on Asthma (demonstration of devices) 32
Year 3 Remaining Tasks July 2012 – January 2013 • Learning Collaboratives – Introducing additional quality measures – NCQA – PCMH standards • Technical assistance site visits conducted between September – December 2012 – Dr. Rushton and QTIP team – SCORx. E: second round visits on Asthma (demonstration of devices) 32
 Year 3 Tasks July 2012 – January 2013 • Behavioral Health – Training/certification program available – UMASS – Incorporation of prevention strategies and treatment strategies – Assessment tools - CHADIS – Brokering with community resources – January 2013 Learning Collaborative session will focus on mental health integration – Explore secure messaging for prior authorizations 33
Year 3 Tasks July 2012 – January 2013 • Behavioral Health – Training/certification program available – UMASS – Incorporation of prevention strategies and treatment strategies – Assessment tools - CHADIS – Brokering with community resources – January 2013 Learning Collaborative session will focus on mental health integration – Explore secure messaging for prior authorizations 33
 Year 3 • HIT assistance • Connectivity and data gathering from EMR • Installing CHIPRA Data Registry in practices without and EMR • Continue to work on SCHIEx connection • Quality Reports • October 2012 • Evaluation Activities • • • CHIPRA Intervention Survey Quality Measure Analysis – CHIPRA and Comparison CAHPS results Provider Integration/PCMH results Feedback 34
Year 3 • HIT assistance • Connectivity and data gathering from EMR • Installing CHIPRA Data Registry in practices without and EMR • Continue to work on SCHIEx connection • Quality Reports • October 2012 • Evaluation Activities • • • CHIPRA Intervention Survey Quality Measure Analysis – CHIPRA and Comparison CAHPS results Provider Integration/PCMH results Feedback 34
") Now For Today… • Introducing 2 additional quality measures – BMI (motivational interviewing ) – Hemoglobin Testing and Control • Presenting PCMH toolkit • Practice spread
Now For Today… • Introducing 2 additional quality measures – BMI (motivational interviewing ) – Hemoglobin Testing and Control • Presenting PCMH toolkit • Practice spread
 And Within the Next 6 Months… • Work on the new quality measures, NCQA-PCMH and Behavioral Health • Send and receive data through your EMR • Connect to SCHIEx • Participate in on-site visits; be a peer reviewer • PDSA/QI: minimum 4 PDSAs/quarter • Document what you do! • Sustainability • Develop series of PDSA cycles that provide MOC credit opportunities for the doctors in your practice • Work on spreading the QI concepts practice-wide
And Within the Next 6 Months… • Work on the new quality measures, NCQA-PCMH and Behavioral Health • Send and receive data through your EMR • Connect to SCHIEx • Participate in on-site visits; be a peer reviewer • PDSA/QI: minimum 4 PDSAs/quarter • Document what you do! • Sustainability • Develop series of PDSA cycles that provide MOC credit opportunities for the doctors in your practice • Work on spreading the QI concepts practice-wide
 If it’s not documented…it’s not done… DOCUMENT 37
If it’s not documented…it’s not done… DOCUMENT 37
 Thank you for your continued work and devotion to this project. Focus of SC Grant South Carolina believes that children will achieve the best health outcomes when they receive care through an integrated medical home that addresses all their health needs—both physical and mental—and participates in continuous quality improvement efforts. 38
Thank you for your continued work and devotion to this project. Focus of SC Grant South Carolina believes that children will achieve the best health outcomes when they receive care through an integrated medical home that addresses all their health needs—both physical and mental—and participates in continuous quality improvement efforts. 38