2187b2d5460cb6ebabb637630b875616.ppt
- Количество слайдов: 32



Children System of Care Application Process for Behavioral Assistance & Intensive In-Community Providers can download the application and instructions from CSOC website at http: //www. state. nj. us/dcf/provi ders/csc/training/ or call CSOC at 609 -888 -7200. These are the only two ways to access an application at this time. Department of Children and Families, Children’s System of Care, PO Box 717, Trenton NJ 08625 -0717 The Medicaid Office of Provider Enrollment will make a final check of application and then send copy to Molina Office of Provider Enrollment. Molina will notify the Medicaid Office of Provider Enrollment of the Provider’s seven-digit provider number and effective date. Provider completes application. If they have any questions completing the forms provided, they can contact Molina Office of Provider Enrollment at 609 -588 -6036. For general information about the program or the new services, please call the CSOC office at 609 -8887690. Application is returned to CSOC office. It will be reviewed to make sure all necessary signatures, license and certifications are present. CSOC office will then forward the application on to the Medicaid Office of Provider Enrollment certifying that this provider has been approved to be a CSOC provider and meets the necessary CSOC requirements. The Medicaid Office of Provider Enrollment will sent out an enrollment letter to the provider. The letter will notify them of their new seven-digit provider number and the start date. The CSOC will be copied on this letter.
 who will be AUTHORIZED TO SIGN THE")
Signature Authorization Form Full Names of Individual(s) who will be AUTHORIZED TO SIGN THE CLAIM FORMS. ALL CLAIMS MUST HAVE AN ORIGINAL SIGNATURE. NO STAMPED OR COPIED SIGNATURES ARE ACCEPTED. . Date: Enter today’s DATE when you are completing the form. Enter your LEGAL or CORPORATE name that coincides with your Federal Tax ID # or Provider Name: if you are a SOLE PROPRIETOR then you can use a SS #. Provider Address: Enter your OFFICE ADDRESS Provider Number: Enter APPLYING PLEASE PRINT OR TYPE: Full Name Actual Signature(s) PRINT or TYPE your Name. SIGN your Name

Signature Authorization Form Dear Provider: Please furnish below the full names of those individuals you have authorized to sign and certify Medicaid claims and supporting documents. If the authorized individual is the Medicaid Provider, he/she must sign the Authorization Form. In addition to the above, this form should only be completed by an authorized representative(s) who is an employee of your office. Should your office utilize a billing firm or agency, a letter signed by yourself must be submitted indicating the name(s) of those individuals you have authorized to sign. The name(s) should be typed and then the actual signature affixed by that individual. The letter should contain the name of the billing firm or agency which has been approved to provide your billing. Date: _________________ Provider Name ________________________ Provider Address _______________________________________________ Provider Number _____________ PLEASE PRINT OR TYPE: Full Name Actual Signature(s) _____________________________________________________________________ _____________________________________________________________________ ___________________________________

FD-20 Application

FD-20 Application #1. Enter LEGAL NAME or CORPORATE NAME that coincides with your Federal Tax Id # or if you are a SOLE PROPRIETOR use your SS #. #2. Enter Children’s System of Care Services. #3. Enter the NAME OF YOUR BUSINESS, if different then # 1 (legal name). i. e. What is your business called?

FD 20 Application, cont’d #4. Employer Tax Id #: 9 -digits given by the IRS @ start of your business. #5. Telephone # & Extension: A # where you can be outreached. #8 -13. Practice Office: Location of actual business. #14 -18. Pay Address: Where Checks & Remittance Advices (RA’s) are mailed.

FD 20 Application, cont’d #19 -23. Mail Address: Where Newsletters/Correspondence are mailed. #24. E-mail Address. #25. Fax #. #28. Indicate Type of Service: Behavior Assistance, Intensive In -Community or Both.
")
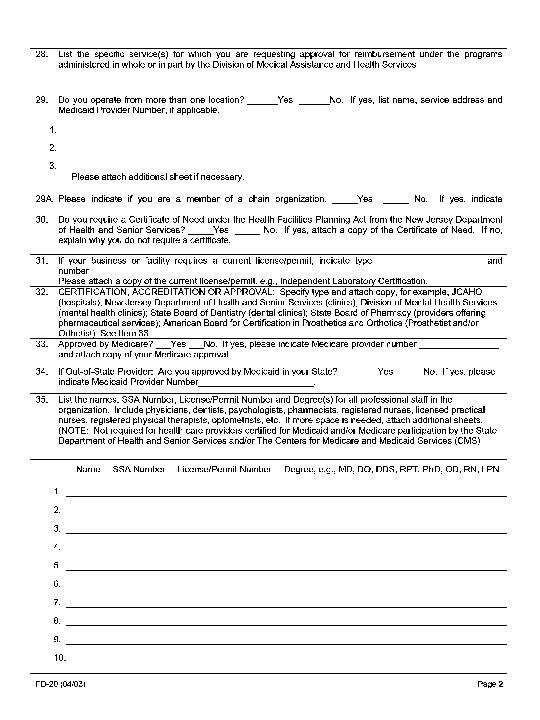
FD 20 Application, cont’d #29. List All Offices within that county. #35. List Name(s) & Degree(s) as appropriate & submit Copy of Current License(s). 37. Check “All” & List usual & customary Fees.

For Unisys Internal Use Only Provider Name: __________________________ Doc Type: _________ Provider Type: ______ Provider Specialty: _____ Tax ID: ____________ Social Security: ________________ Provider Number: _______________ #1 Enter LEGAL NAME or CORPORATE NAME that coincides with your Federal Tax Id # or if you State of New Jersey are a SOLE PROPRIETOR use your SS #. DEPARTMENT OF HUMAN SERVICES Division of Medical Assistance and Health Services # 2 Enter Children’s System of Care Services PROVIDER APPLICATION 1. Legal Name of Provider 2 A. Type of Business or Facility 2. Provider Type Sole Proprietor Corporation Partnership Other (Specify) 3. Business Name, if Different from Above 4. Employer/Tax ID Number/Social Security Number 5. Telephone Number/Extension 6. Length of time at Practice address in New Jersey 7. Name of Administrator, Chief Executive Officer, Other Responsible Official 8. Practice Address (Do not use P. O. Box) 9. Street 10. City 11. State 12. County 13. Zip 14. Pay To Address (for Checks/Remittance Advice) 15. Street 16. City 17. State 18. Zip 19. Mail To Address (for Newsletters/Correspondence) 20. Street 21. City 22. State 23. Zip 24. E-mail Address 25. Fax # 26. Indicate NJ Charity Care Provider ______Yes ______No (Questions 26 -26 H are for NJ acute care hospitals only) 26 A. Charity Care Pay To Address (Remittance Advice) 26 B. Street 26 C. City 26 D. State 26 E. Zip 26 F. Charity Care Telephone Number/Extension 26 G. Charity Care Fax # 26 H. Charity Care E-mail Address 27. Indicate legal status of your organization: Profit ______ Non-Profit______ Private______ Public______ If other, please specify____________________________________________ FD-20 (04/03) Page 1

Provider Agreement FD-62

FD-62 Agreeing to: • All Terms & Conditions • Comply w/ all State & Federal Laws • Maintain Medical Record • Furnish Info. re: Payments Claimed for Services • Comply w/ all Amendments which makes it a Crime for persons making any False Statements or Representations • Accept Payment as Payment in Full & not to Institute Collection Activities against Beneficiaries

This document outlines what you are agreeing to as a NJ CSOC Medicaid Provider Must Sign & Date Print Name & Title

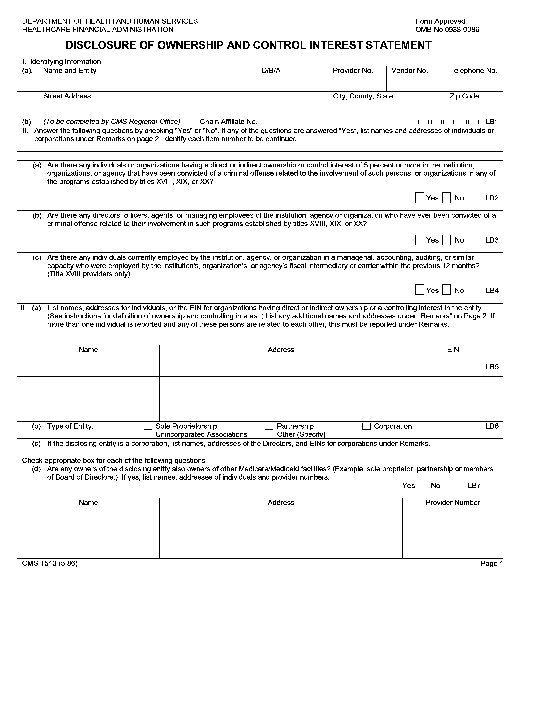
Ownership & Control Interest Statement • Any entity, corporation or facility – this form is utilized to indicate any type of controlling ownership that exists w/in your facility. • Any change of ownership – a NEW form must be completed & submitted.

Ownership & Control Interest Statement Required Fields Section 1 #1. Name of Entity #2. Telephone # #3. Street Address, City, County, State & Zip Code Section 2 All Question. Yes, No or N/A. Section 3 Only required if you are an individual w/ a direct or indirect ownership. Section 4 thru Section 8 All Questions. Yes, No or N/A. Last Section Print Name of Authorized Representative & Title w/ Signature & Date.

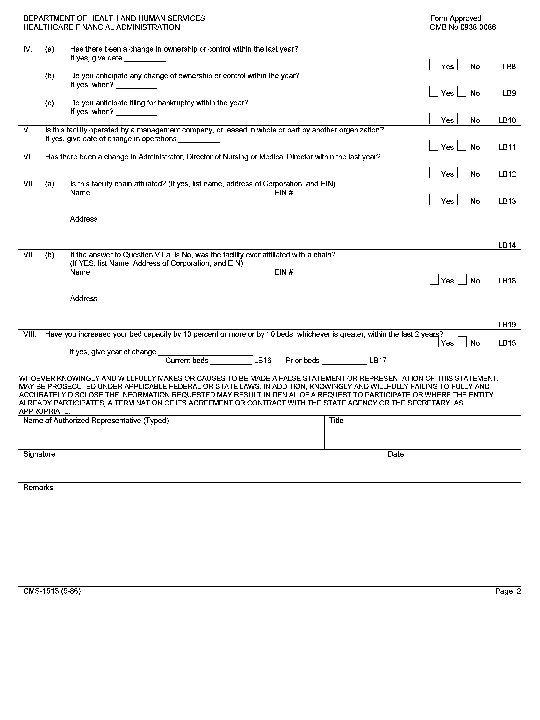
SPECIAL INSTRUCTIONS FOR TITLE XX PROVIDERS All title XX providers must complete part II (a) and (b) of this form. Only those title XX providers rendering medical, remedial, or health related home-maker services must complete Parts II and III. Title V providers must complete parts II and III.
 EASY WAYS to Access the Application. 1. 2.")
Recap of Application Process Two (2) EASY WAYS to Access the Application. 1. 2. Provider completes application. Any questions, call Download from CSOC website @ http: //www. state. nj. us/dcf/pr oviders/csc/training Molina Provider Enrollment @ 609588 -6036 For general information about the program or services, call the CSOC office @ 609 -8887200. Call CSOC @ 609 -888 -7200. Department of Children and Families Children’s System of Care P. O. Box 717 Trenton. NJ 08625 -0717 1. 2. The State Medicaid PE Office conducts a final application check & sends copy to the Molina PE. Molina finalizes the application & assigns a seven (7)-digit Medicaid Provider Id # which is added into a Master file. Application is returned to CSOC office. CSOC reviews application for all necessary signature(s), license(s) & certification(s). 3. CSOC forwards application to the State Medicaid Provider Enrollment (PE) Office certifying provider is approved & meets Medicaid requirements to be a CSOC provider. Molina will notify the State Medicaid PE Office of the Provider’s seven (7) digit Id # & Effective Date. The State Medicaid PE Office will mail an enrollment letter to the provider, CSOC Office & Molina of this Provider Id # & State Date.

Web Site Information • Download Application visit CSOC @ http: //www. state. nj. us/dcf/provider s/csc/training • General Information about Medicaid Provider Inquiries & Questions visit www. njmmis. com
 (general information or new services")
Who to call for Help? (when completing the application) (general information or new services ) • General Information about the Program or New Services, call CSOC @ 609 -8887200. • Molina Provide Enrollment Office @ 609 -588 -6036.

• Open for Questions
2187b2d5460cb6ebabb637630b875616.ppt