

73e4e29baccba2fedac1a2077657a1ba.ppt
- Количество слайдов: 64
 Child Onset Depression: Is It a Different Disorder? Neal Ryan
Child Onset Depression: Is It a Different Disorder? Neal Ryan
 Conflict of Interest Statement Ø No industry-funds in prior two years PI on the Pittsburgh site of the Keller et. al study of paroxetine funded by GSK Ø PI on Pittsburgh site of Wyeth study of child depression Ø Paid consultant (lifetime) to: Ø l l l Abbott BMS GSK Johnson and Johnson Pfizer Wyeth
Conflict of Interest Statement Ø No industry-funds in prior two years PI on the Pittsburgh site of the Keller et. al study of paroxetine funded by GSK Ø PI on Pittsburgh site of Wyeth study of child depression Ø Paid consultant (lifetime) to: Ø l l l Abbott BMS GSK Johnson and Johnson Pfizer Wyeth
 Joaquim Puig-Antich, 1944 -1989
Joaquim Puig-Antich, 1944 -1989
 Joaquim Puig-Antich Ø Ø Ø Born: September 22, 1944, Barcelona Spain Died: December 2, 1989 Undergraduate: 1953 -1960, La Salle Bonanova, Barcelona Graduate: 1961 -1967, Facultad de Medicine, Universidad de Barcelona Post Graduate l l 1967: Clinique Rech. , Montpellier, France, Resident in Neurosurgery 1970 -1971: Sinai Hospital, Baltimore, Intern in Medicine 1971 -1973, Beth Israel, New York, Resident in Psychiatry 1973 -1975, Albert Einstein, New York, Child Psychiatry Fellow
Joaquim Puig-Antich Ø Ø Ø Born: September 22, 1944, Barcelona Spain Died: December 2, 1989 Undergraduate: 1953 -1960, La Salle Bonanova, Barcelona Graduate: 1961 -1967, Facultad de Medicine, Universidad de Barcelona Post Graduate l l 1967: Clinique Rech. , Montpellier, France, Resident in Neurosurgery 1970 -1971: Sinai Hospital, Baltimore, Intern in Medicine 1971 -1973, Beth Israel, New York, Resident in Psychiatry 1973 -1975, Albert Einstein, New York, Child Psychiatry Fellow
 Joaquim Puig-Antich Ø Appointments: l 1975 -1977: Albert Einstein, Assistant Professor of Psychiatry l 1977 -1983, Columbia, Assistant Professor of Clinical Psychiatry l 1983 -1984, Columbia, Associate Professor of Clinical Psychiatry l 1984 -1989, Pittsburgh, Professor of Psychiatry l 1988 -1989, Pittsburgh, Professor of Pediatrics
Joaquim Puig-Antich Ø Appointments: l 1975 -1977: Albert Einstein, Assistant Professor of Psychiatry l 1977 -1983, Columbia, Assistant Professor of Clinical Psychiatry l 1983 -1984, Columbia, Associate Professor of Clinical Psychiatry l 1984 -1989, Pittsburgh, Professor of Psychiatry l 1988 -1989, Pittsburgh, Professor of Pediatrics
 Additional Acknowledgements Ron Dahl Ø David Axelson Ø Boris Birmaher Ø David Brent Ø BJ Casey Ø Cam Carter Ø Mike De Bellis Ø Erika Forbes Ø Ø Ø Ø Ø Ahmad Hariri Joan Kaufman Chris Kye Cecile Ladouceur Chris May Jim Perel Scott Waterman Doug Williamson
Additional Acknowledgements Ron Dahl Ø David Axelson Ø Boris Birmaher Ø David Brent Ø BJ Casey Ø Cam Carter Ø Mike De Bellis Ø Erika Forbes Ø Ø Ø Ø Ø Ahmad Hariri Joan Kaufman Chris Kye Cecile Ladouceur Chris May Jim Perel Scott Waterman Doug Williamson
 Department of Psychiatry University of Pittsburgh Medical Center Western Psychiatric Institute and Clinic
Department of Psychiatry University of Pittsburgh Medical Center Western Psychiatric Institute and Clinic
 Child Depression Ø Duration and Course l l Duration 3 -9 months 6 -10% last more than 2 years 70% recurrence in 5 years 20 -40% become bipolar • But 25% total adolescent prevalence of unipolar in epidemiologic studies versus 1 -2% for bipolar disorders so numbers don’t “add up”
Child Depression Ø Duration and Course l l Duration 3 -9 months 6 -10% last more than 2 years 70% recurrence in 5 years 20 -40% become bipolar • But 25% total adolescent prevalence of unipolar in epidemiologic studies versus 1 -2% for bipolar disorders so numbers don’t “add up”
 Clinical Picture Clinical picture in child, adolescent and adult depression very similar Ø Endogenicity/melancholic, suicide attempts, lethality of suicide attempts, and impairment of functioning increase with age Ø Separation anxiety, phobias, somatic complains and comorbid behavioral problems decrease with age Ø
Clinical Picture Clinical picture in child, adolescent and adult depression very similar Ø Endogenicity/melancholic, suicide attempts, lethality of suicide attempts, and impairment of functioning increase with age Ø Separation anxiety, phobias, somatic complains and comorbid behavioral problems decrease with age Ø
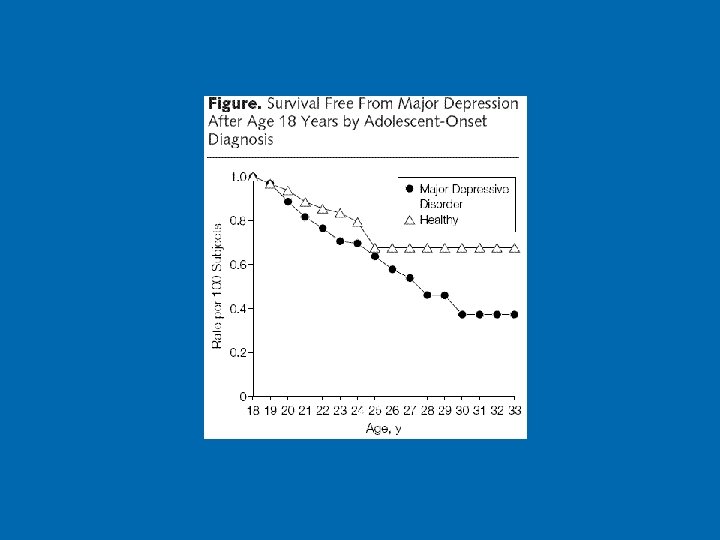
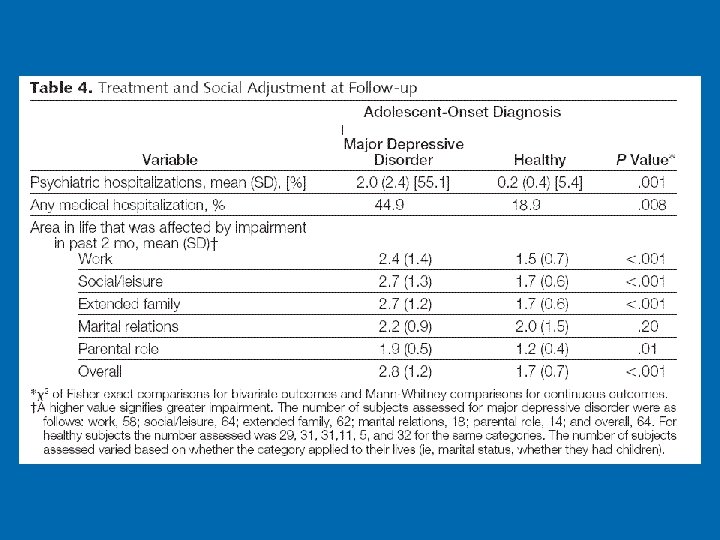
 Psychosocial Outcomes Ø During depression and after recovery: l l l Worse functioning with friends and family Impaired performance in school Higher rate of pregnancy More smoking – “gateway” Clear long-term persistence after “successful” treatment of depression
Psychosocial Outcomes Ø During depression and after recovery: l l l Worse functioning with friends and family Impaired performance in school Higher rate of pregnancy More smoking – “gateway” Clear long-term persistence after “successful” treatment of depression
 Increase in rate of depression, particularly great in girls, correlated with puberty and not age per se Ø Point Prevalence l l 0. 4 to 2. 5% in children 1: 1 sex ratio 0. 4 to 8. 3% in adolescents 2: 1 female excess Ø Lifetime prevalence in adolescence l 15% - 25%
Increase in rate of depression, particularly great in girls, correlated with puberty and not age per se Ø Point Prevalence l l 0. 4 to 2. 5% in children 1: 1 sex ratio 0. 4 to 8. 3% in adolescents 2: 1 female excess Ø Lifetime prevalence in adolescence l 15% - 25%
 What other disorders are like Major Depressive Disorder Ø Similar l Complex genetic disorders, large environmental contribution, exacerbated by stress, treatment but no “cure”, the group that is responsible for most medical morbidity • • • Ø Hypertension Obesity, adult onset diabetes Alcohol Abuse Not similar • • • Communicable diseases (avian flu) Single-gene disorders (ALS, sickle cell disease) Being struck by lightning
What other disorders are like Major Depressive Disorder Ø Similar l Complex genetic disorders, large environmental contribution, exacerbated by stress, treatment but no “cure”, the group that is responsible for most medical morbidity • • • Ø Hypertension Obesity, adult onset diabetes Alcohol Abuse Not similar • • • Communicable diseases (avian flu) Single-gene disorders (ALS, sickle cell disease) Being struck by lightning
 A Model for Genesis and Maintenance of Child Depression
A Model for Genesis and Maintenance of Child Depression
 Child to Adult Depression Ø Continuities l l Clinical picture Clinical course Responds to CBT and IPT in adolescents Responds to (at least some) SSRIs Ø Discontinuities l l Probably unresponsive or minimally responsive to TCAs Some biological correlates of depression show maturational effects
Child to Adult Depression Ø Continuities l l Clinical picture Clinical course Responds to CBT and IPT in adolescents Responds to (at least some) SSRIs Ø Discontinuities l l Probably unresponsive or minimally responsive to TCAs Some biological correlates of depression show maturational effects
 Child Depression vs. Adolescent Depression vs. Adult Depression Ø Adolescent Depression is continuous with adult depression; child depression shows less continuity but studies are very limited Ø Perinatal insults, motor skill deficits, care taking instability and family-of-origin psychopathology increases hazard for child depression but not adult depression (Jaffee 2002)
Child Depression vs. Adolescent Depression vs. Adult Depression Ø Adolescent Depression is continuous with adult depression; child depression shows less continuity but studies are very limited Ø Perinatal insults, motor skill deficits, care taking instability and family-of-origin psychopathology increases hazard for child depression but not adult depression (Jaffee 2002)
 Outcome of Child/Adolescent Depression Ø More depression and anxiety l Ø probably a direct result of prior depression episode More nicotine dependence, alcohol abuse, suicide attempts, educational underachievement, unemployment and early parenthood l possibly as a result of shared risk factors for depression and other adverse outcomes (Fergusson et al, 2002) though not all data supports this conclusion
Outcome of Child/Adolescent Depression Ø More depression and anxiety l Ø probably a direct result of prior depression episode More nicotine dependence, alcohol abuse, suicide attempts, educational underachievement, unemployment and early parenthood l possibly as a result of shared risk factors for depression and other adverse outcomes (Fergusson et al, 2002) though not all data supports this conclusion
 Initiation of smoking
Initiation of smoking
 Substance abuse / dependence
Substance abuse / dependence
 Puberty
Puberty
 Puberty is starting earlier
Puberty is starting earlier
 Puberty and Brain Development Some brain changes precede pubertal increase in hormones and body changes Ø Some brain changes appear to be the consequence of some pubertal processes Ø Some adolescent brain maturation appears to be independent of pubertal processes Ø Potential for creating internal dis-synchrony Ø Slide courtesy R. Dahl
Puberty and Brain Development Some brain changes precede pubertal increase in hormones and body changes Ø Some brain changes appear to be the consequence of some pubertal processes Ø Some adolescent brain maturation appears to be independent of pubertal processes Ø Potential for creating internal dis-synchrony Ø Slide courtesy R. Dahl
 Puberty and Motivation/Emotion Strongest links to pubertal changes per-se are in the domains of romantic motivation, sexual interest, emotional intensity, sleep/arousal regulation, appetite, and affective disorders Ø A general increase in risk-taking, noveltyseeking, sensation-seeking (reward-seeking). Ø Animal studies also show increase in noveltytaking (risk-taking? ) in the peri-adolescent period (Spear 2000) Ø Slide courtesy R. Dahl
Puberty and Motivation/Emotion Strongest links to pubertal changes per-se are in the domains of romantic motivation, sexual interest, emotional intensity, sleep/arousal regulation, appetite, and affective disorders Ø A general increase in risk-taking, noveltyseeking, sensation-seeking (reward-seeking). Ø Animal studies also show increase in noveltytaking (risk-taking? ) in the peri-adolescent period (Spear 2000) Ø Slide courtesy R. Dahl
 Puberty Ø Ø Ø A number of developmental hormonal changes occur during the pubertal transition (reproductive hormones, adrenal androgens, growth hormones). Hormone levels fluctuate across hours and days. Increased stress exposure during adolescence also leads to hormonal (cortisol) and brain changes. There are complex interactions between reproductive hormones, stress-related hormones, and neural systems that regulate behavioral affect. There are profound individual differences in developmental trajectories in each of these systems. Slide courtesy R. Dahl
Puberty Ø Ø Ø A number of developmental hormonal changes occur during the pubertal transition (reproductive hormones, adrenal androgens, growth hormones). Hormone levels fluctuate across hours and days. Increased stress exposure during adolescence also leads to hormonal (cortisol) and brain changes. There are complex interactions between reproductive hormones, stress-related hormones, and neural systems that regulate behavioral affect. There are profound individual differences in developmental trajectories in each of these systems. Slide courtesy R. Dahl
 Brain Development
Brain Development
 Brain Development by Anatomic Region (145 Children & Adolescents age 4 -22 years of age who underwent 243 MRI Scans) [Giedd et al] Peak Cerebellum vs. Other Peaks: * <. 002, ** <. 0001
Brain Development by Anatomic Region (145 Children & Adolescents age 4 -22 years of age who underwent 243 MRI Scans) [Giedd et al] Peak Cerebellum vs. Other Peaks: * <. 002, ** <. 0001
 Overview of Psychotherapy Studies in Child and Adolescent Depression
Overview of Psychotherapy Studies in Child and Adolescent Depression
 Psychotherapy Ø CBT l Ø CBT works better than wait-list and better than some other psychotherapies in child and adolescent major depression (Reinecke 1998, Harrington 1998; Brent 1997; Clarke 1999) IPT l Works in depressed adolescents (Mufson, 1999)
Psychotherapy Ø CBT l Ø CBT works better than wait-list and better than some other psychotherapies in child and adolescent major depression (Reinecke 1998, Harrington 1998; Brent 1997; Clarke 1999) IPT l Works in depressed adolescents (Mufson, 1999)
 TADS Results Ø SSRI+CBT and SSRI better then placebo and better than CBT alone aggregating across measures Ø CBT seemed to protect against suicidality while SSRI may increase it Ø Combination better than SSRI alone but by small margin
TADS Results Ø SSRI+CBT and SSRI better then placebo and better than CBT alone aggregating across measures Ø CBT seemed to protect against suicidality while SSRI may increase it Ø Combination better than SSRI alone but by small margin
 A RCT of CBT to Prevent Adolescent Depression 13 -18 yo adolescents who were at high risk for MDD because of family history (parental) for treated MDD current or in past year and who currently had subsyndromal depressive symptoms Ø Randomized to usual care (N=49) or 15 one-hour sessions of group CBT (N=45) Ø 26 month f/u Ø l l 9. 3% MDD in CBT group versus 28. 8 in usual care by 14 months Preventive effect persisted but somewhat diminished at 18 and 24 months
A RCT of CBT to Prevent Adolescent Depression 13 -18 yo adolescents who were at high risk for MDD because of family history (parental) for treated MDD current or in past year and who currently had subsyndromal depressive symptoms Ø Randomized to usual care (N=49) or 15 one-hour sessions of group CBT (N=45) Ø 26 month f/u Ø l l 9. 3% MDD in CBT group versus 28. 8 in usual care by 14 months Preventive effect persisted but somewhat diminished at 18 and 24 months
 Long Term Course and Maintenance Ø Little evidence for long-term effect of shortterm treatment l Ø Modest evidence for long-term maintenance l Ø CBT better than otherapy acutely but no difference in longitudinal course (Birmaher 2000) Fluoxetine better than placebo in preventing relapse over 1 year in fluoxetine responders, 34 vs 60% relapse (Emslie 2001) However, overall there is little data
Long Term Course and Maintenance Ø Little evidence for long-term effect of shortterm treatment l Ø Modest evidence for long-term maintenance l Ø CBT better than otherapy acutely but no difference in longitudinal course (Birmaher 2000) Fluoxetine better than placebo in preventing relapse over 1 year in fluoxetine responders, 34 vs 60% relapse (Emslie 2001) However, overall there is little data
 Pharmacotherapy of Child and Adolescent Depression
Pharmacotherapy of Child and Adolescent Depression
 Pharmacotherapy Ø In adults SSRIs = SNRIs = TCAs Ø In children SSRIs > TCAs
Pharmacotherapy Ø In adults SSRIs = SNRIs = TCAs Ø In children SSRIs > TCAs
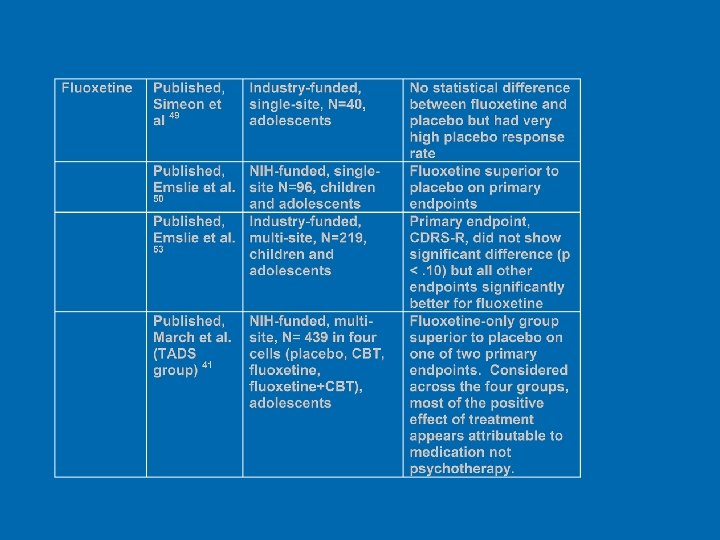
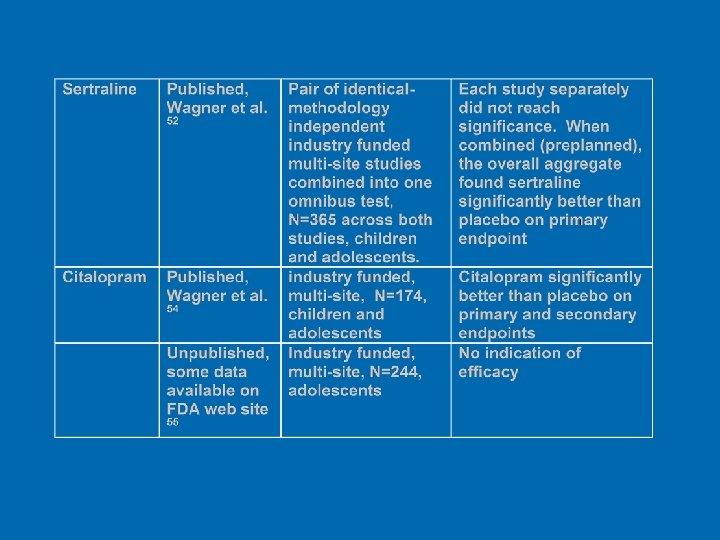
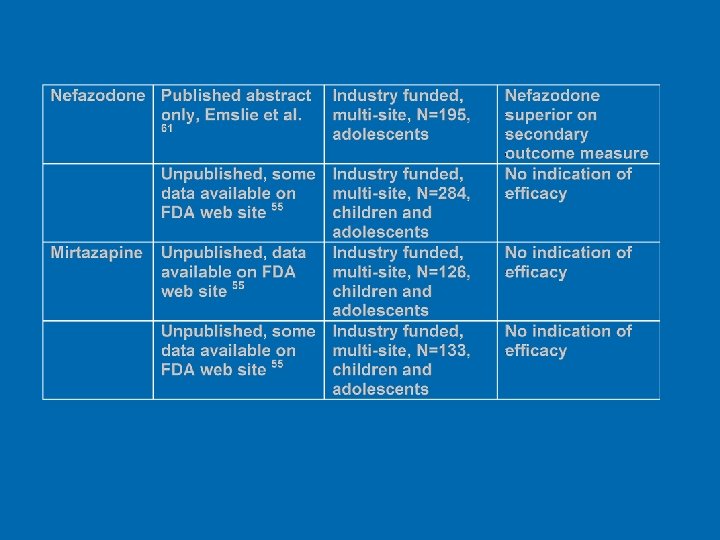
 Summary Ø Signal that SSRIs work l l But less than half of studies are “positive” This is like adult industry studies The more sites in the study, the smaller the effect size found (Brent et al. , in press) Ø Rushed studies probably decrease measured effect size Ø However, even if this is true, you don’t have any way to say how much this decrease is! Ø
Summary Ø Signal that SSRIs work l l But less than half of studies are “positive” This is like adult industry studies The more sites in the study, the smaller the effect size found (Brent et al. , in press) Ø Rushed studies probably decrease measured effect size Ø However, even if this is true, you don’t have any way to say how much this decrease is! Ø
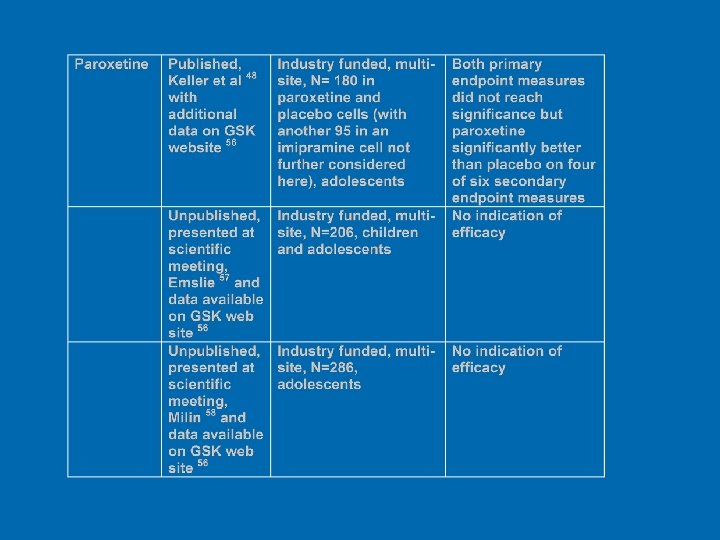
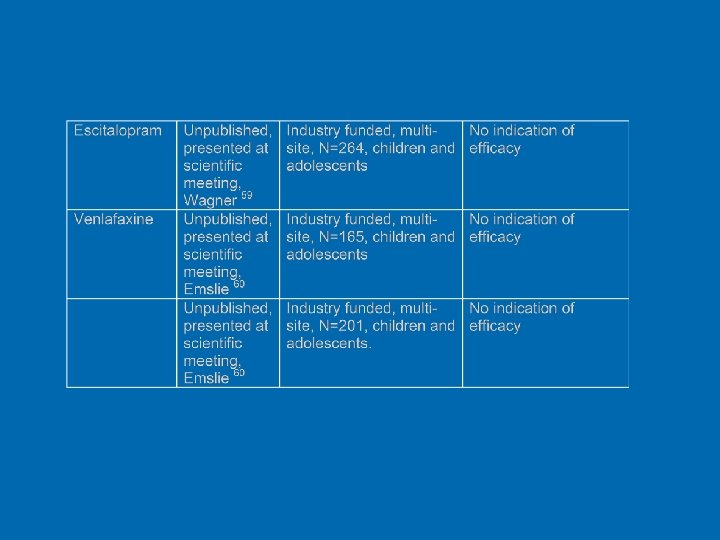
 Summary Ø Fluoxetine best replicated Ø FDA does not feel that data available for other agents sufficient for indication Ø Data not bad for citalopram and sertraline Ø Data quite mixed for paroxetine
Summary Ø Fluoxetine best replicated Ø FDA does not feel that data available for other agents sufficient for indication Ø Data not bad for citalopram and sertraline Ø Data quite mixed for paroxetine
") Putting Child and Adolescent Depression in it’s place (compared to adult depression)
Putting Child and Adolescent Depression in it’s place (compared to adult depression)
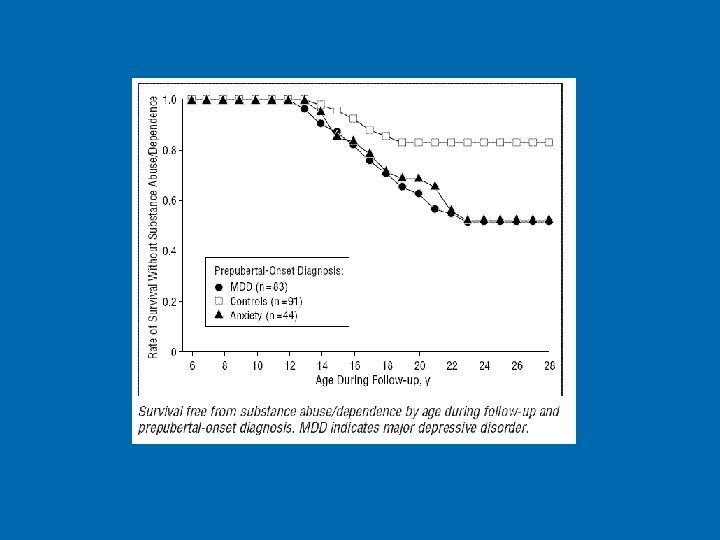
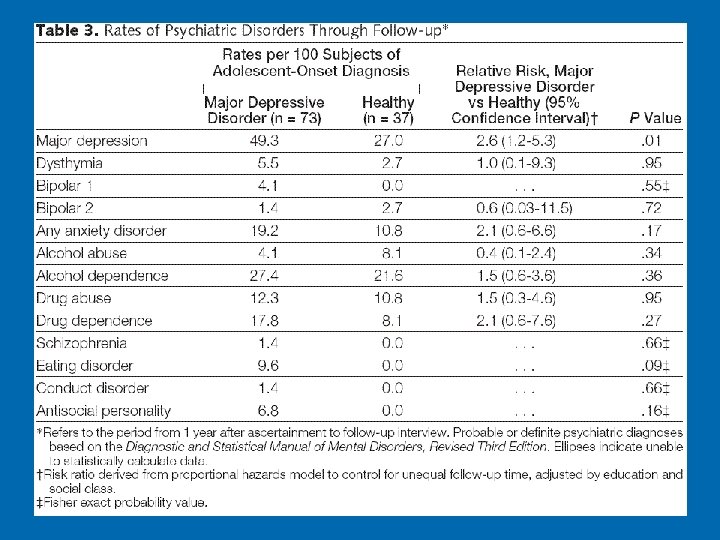
 No difference in rates of adult MDD between MDD, anxiety and control prepubs, but 59% of prepub MDD had recurrence of depression. In those, there was elevated rate of MDD in relatives.
No difference in rates of adult MDD between MDD, anxiety and control prepubs, but 59% of prepub MDD had recurrence of depression. In those, there was elevated rate of MDD in relatives.

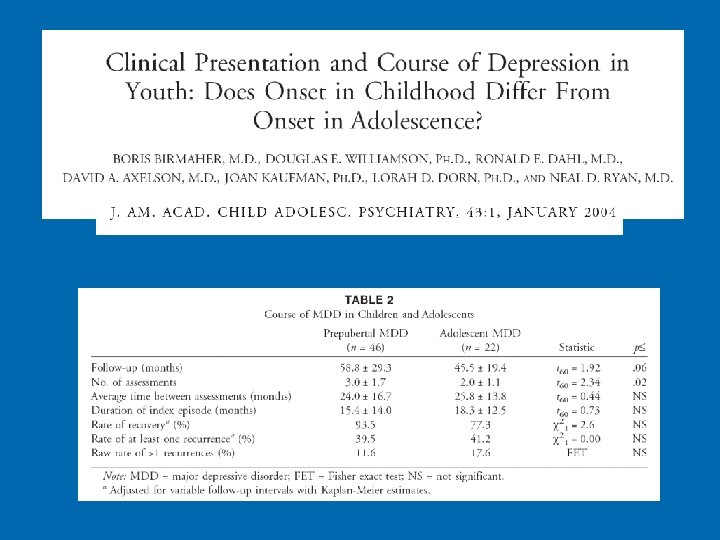
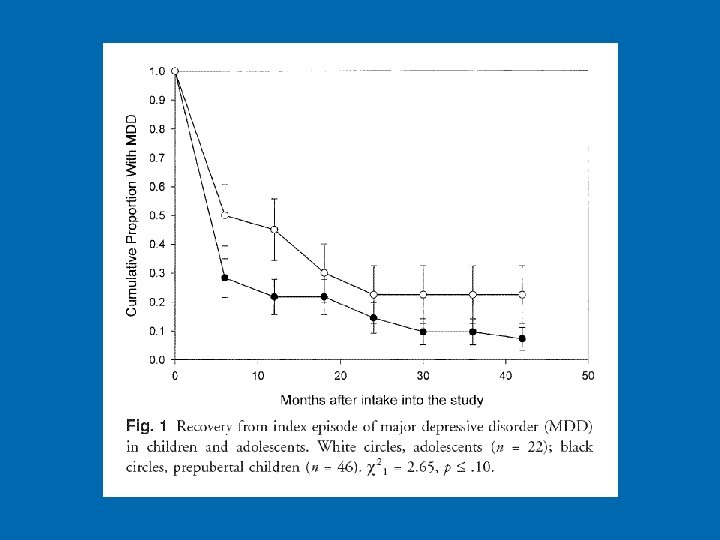
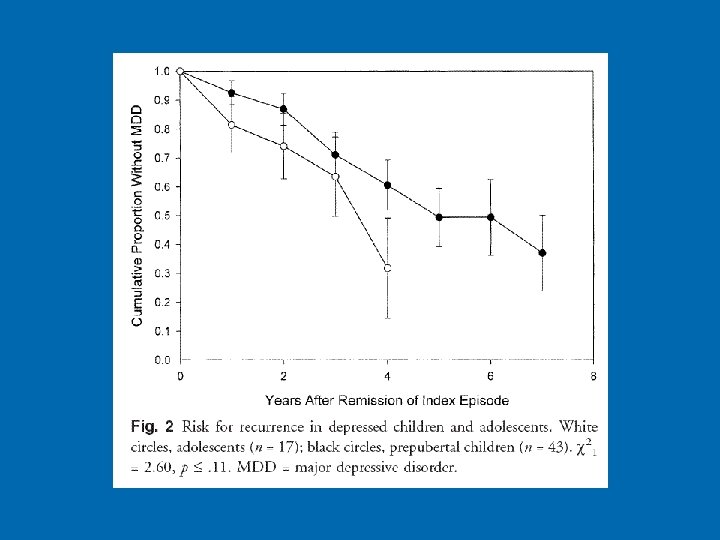
 Results Ø Ø Ø Ø Ø More melancholic symptoms in depressed adolescents but otherwise children and adolescents have similar symptomatology, duration, and severity of the index episode Similar rates of recovery and recurrence Similar comorbid disorders Similar parental history of psychiatric disorders Index episode of both groups lasted on average 17 months. 85% of children and adolescent recovered 40% had at least one recurrence Guilt and female sex predicted longer episodes Prior history of MDD and father MDD predicted lower recovery and increased risk for recurrence
Results Ø Ø Ø Ø Ø More melancholic symptoms in depressed adolescents but otherwise children and adolescents have similar symptomatology, duration, and severity of the index episode Similar rates of recovery and recurrence Similar comorbid disorders Similar parental history of psychiatric disorders Index episode of both groups lasted on average 17 months. 85% of children and adolescent recovered 40% had at least one recurrence Guilt and female sex predicted longer episodes Prior history of MDD and father MDD predicted lower recovery and increased risk for recurrence
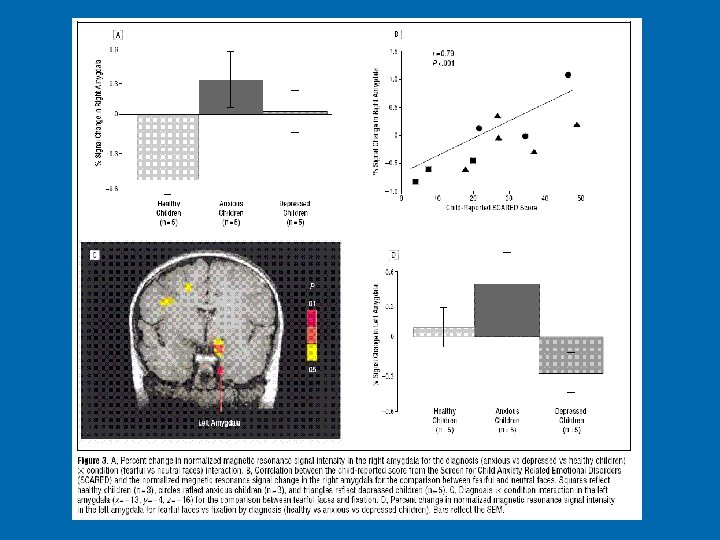
 • trait-like marker for depression (or depression and anxiety • stable through development and adulthood • may be result of early life stressors (e. g. macaque variable foraging paradigm)
• trait-like marker for depression (or depression and anxiety • stable through development and adulthood • may be result of early life stressors (e. g. macaque variable foraging paradigm)
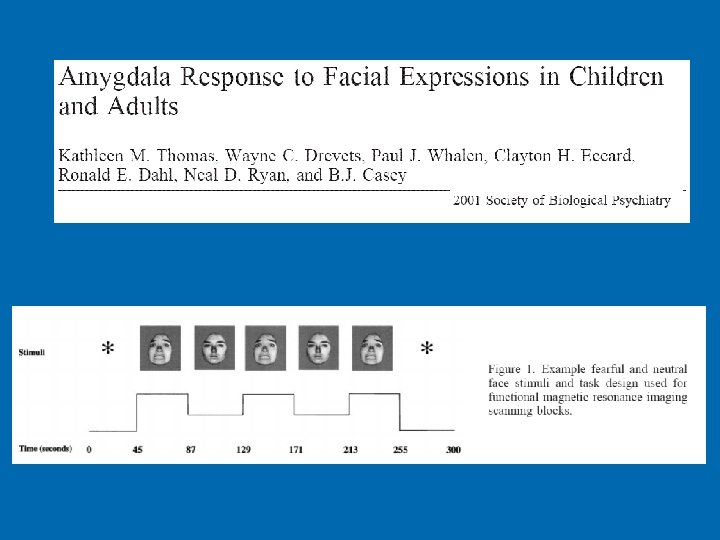
 Results Increased activity in amygdala during presentation of fearful faces and a decrease in activation with repeated exposure to fearful faces Ø Developmental differences in amygdala response to fearful and neutral faces Ø l l Adults show increased amygdala activity for fearful faces Children show more amygdala activity in response to neutral faces • Children may find neutral faces to be more ambiguous than adults do or even more ambiguous than fearful faces.
Results Increased activity in amygdala during presentation of fearful faces and a decrease in activation with repeated exposure to fearful faces Ø Developmental differences in amygdala response to fearful and neutral faces Ø l l Adults show increased amygdala activity for fearful faces Children show more amygdala activity in response to neutral faces • Children may find neutral faces to be more ambiguous than adults do or even more ambiguous than fearful faces.
 14 MDD and 17 control children 9 -17 years Of 14 with MDD, 10 also had comorbid anxiety disorder
14 MDD and 17 control children 9 -17 years Of 14 with MDD, 10 also had comorbid anxiety disorder
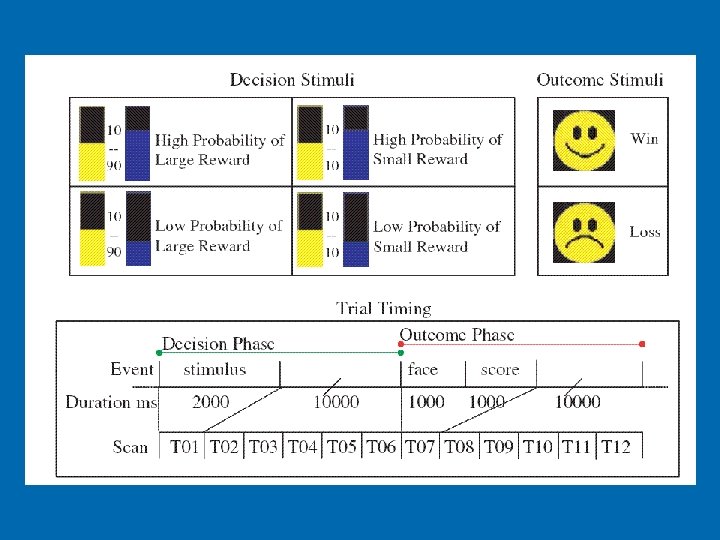
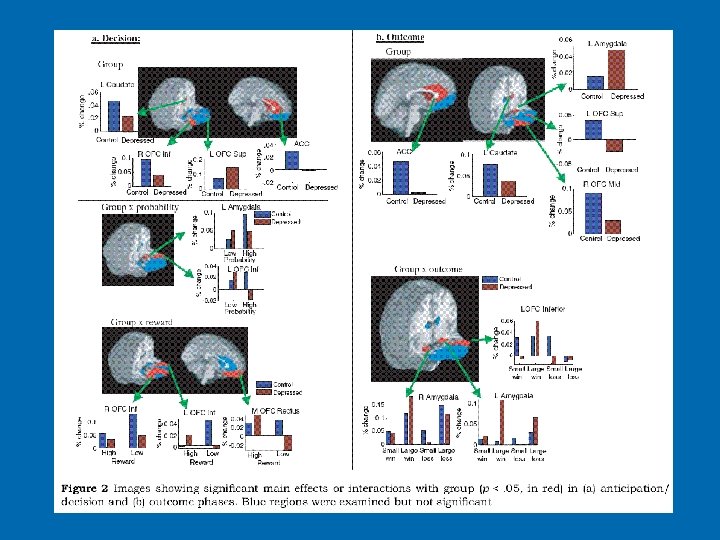
 Reward Related Decision Making Ø Anxiety disorders l Increased response in cingulate and left caudate (reward related areas) during anticipation of reward and in caudate after receiving large-magnitude reward Ø MDD l Decreased response caudate after receiving a large-magnitude reward.
Reward Related Decision Making Ø Anxiety disorders l Increased response in cingulate and left caudate (reward related areas) during anticipation of reward and in caudate after receiving large-magnitude reward Ø MDD l Decreased response caudate after receiving a large-magnitude reward.
 Thanks
Thanks