fec3c51f0148e0728c4120d04eac2414.ppt
- Количество слайдов: 157



Cerebral Oximetry and Neuroprotection 10 th International Conference Heart Summits Lahore October 13 th 2017 Sean Bennett Consultant Cardiothoracic Anaesthetist and Intensivist King Abdulaziz Medical City, Jeddah

Aim is to…. • Understand neuroprotection. Should we insult the brain and try to limit the damage or keep the brain well oxygenated throughout? • Ischaemia is a time line to infarction • Does cerebral oximetry play a role in protecting the brain?

Method • Demonstrate where physiology, that we control, effects the patient outcome. • And how we can use Near Infra. Red Spectroscopy (NIRS) as a means of measuring the physiological changes. • Literature • Case histories
, partially (longer")
We can… • Stop the supply of oxygen, completely (for short periods), partially (longer periods). • Reducing the flow or pressure • Cause embolic events, plaque, debris, bubbles, thrombus, etc.

What do we do if…. • • • In response to bleeding……measure Hb In response to ventilation…. . Sa. O 2/Pa. CO 2 In response to renal insuff. . . measure urine In response to myocardial insult…. ECG In response to dysrhythmia…. . K+ In response to neuro insult…. . ? ? ?

• We tend to mitigate the insult by: • Drugs, cooling, keeping the pressure up
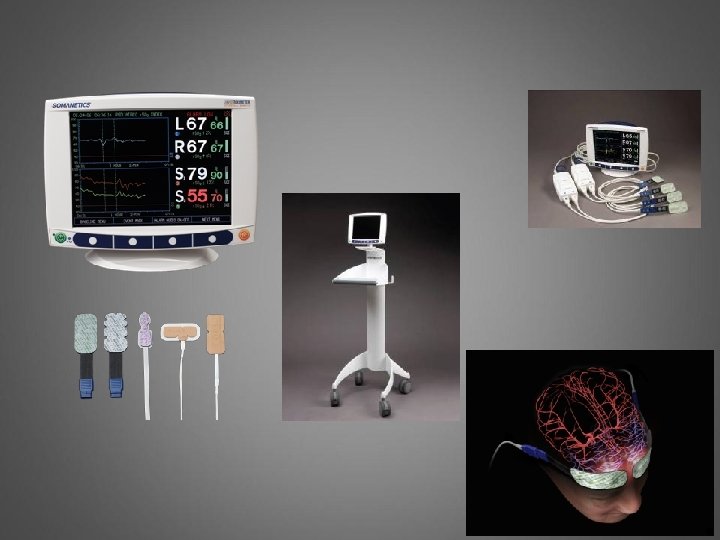

Review of the Technology Penetration of NIRS Light The human skull is easily penetrated by near-infrared light Longer wavelength infrared light penetrates better than visible light

Empirically Validated in Human Subjects Distal Detector Proximal Detector LED Emitter Signal from surface tissues are subtracted out Hongo K, Kobayashi S, Okudera H, Hokama M, Nakagawa F. Noninvasive cerebral optical spectroscopy: Depth-resolved measurements of cerebral haemodynamics using indocyanine green. Neurol Res. 1995; 17(2): 89 -93. 9 |

Empirically Validated in Human Subjects Distal Detector Proximal Detector LED Emitter Signal from surface tissues are subtracted out Hongo K, Kobayashi S, Okudera H, Hokama M, Nakagawa F. Noninvasive cerebral optical spectroscopy: Depth-resolved measurements of cerebral haemodynamics using indocyanine green. Neurol Res. 1995; 17(2): 89 -93. 10 |
 Clinical Characteristic")
Combines Sp. O 2 and SJO 2 Cerebral Oximetry (r. SO 2) Clinical Characteristic Noninvasive • Does not require pulsatile flow Pulse (Arterial) Oximetry (Sp. O 2) Clinical Characteristics Noninvasive • Requires pulsatility and flow • Jugular (Venous) Oxygen (Sj. O 2) Clinical Characteristics Invasive • Venous sample Think more Mixed Venous O 2 saturations for the brain

The Current Situation: is the brain OK? ØSV 02 CO ØCPP/MAP/Pa. CO 2 and Sa 02 ØSerum lactate and urine output

Calcified aorta: patientoutcomes • One patient required AVR and CABG who intra-operatively was found to have a calcified aorta. • What do you do?

You can see strokes happening 40 20

Cerebral Oximetry for Cardiac and Vascular Surgery Harvey L. Edmonds Seminars in Cardiothoracic and Vascular Anesthesia, Vol 8, No 2 (June), 2004: pp 147– 166 • The overwhelming consensus of studies is the use of cerebral oximetry during cardiac and vascular operations is associated with significant and cost-effective reductions in neurocognitive injury and hospital cost drivers. The risk of brain oxygen monitoring is nil.

Cerebral Near-Infrared Spectroscopy Monitoring and Neurologic Outcomes in Adult Cardiac Surgery Patients: A Systematic Review Zheng, Sheinberg et al. Anesth Analg 2013; 116: 663– 76

Cerebral Near-Infrared Spectroscopy Monitoring and Neurologic Outcomes in Adult Cardiac Surgery Patients: A Systematic Review • 1 st; are decrements in cerebral oximetry during cardiac surgery are associated with: Ø Stroke Ø postoperative cognitive dysfunction Ø delirium • 2 nd; whether interventions aimed at correcting cerebral oximetry decrements improve neurologic outcomes.

Cerebral Near-Infrared Spectroscopy Monitoring and Neurologic Outcomes in Adult Cardiac Surgery Patients: A Systematic Review • 13 case reports, 27 observational and 2 RCT using NIRS during cardiac surgery. Ø Stroke: No studies powered to show a difference. Ø Postoperative cognitive dysfunction: 6/9 studies reported worse POCD with acute falls in NIRS. Ø Delirium: older age, lower MMSE score, neurologic disease, low baseline r. SO 2, but not intraoperative r. SO 2 desaturation.

Cerebral Near-Infrared Spectroscopy Monitoring and Neurologic Outcomes in Adult Cardiac Surgery Patients: A Systematic Review • Secondly whether interventions aimed at correcting cerebral oximetry decrements improve neurologic outcomes. Ø No evidence that changing the r. SO 2 values modified the outcomes.

Cerebral Near-Infrared Spectroscopy Monitoring and Neurologic Outcomes in Adult Cardiac Surgery Patients: A Systematic Review Did they find anything positive? Ø 7/9 studies showed a reduction in ICU or hospital length of stay. Ø A correlation between pre-op low r. SO 2 and post-op outcome in general. But not modifiable Ø Mal-positioning of aortic cannula identifiable by NIRS.

Cerebral Near-Infrared Spectroscopy Monitoring and Neurologic Outcomes in Adult Cardiac Surgery Patients: A Systematic Review Ø hospital length of stay- so something improved. Ø A correlation between pre-op low r. SO 2 and post-op outcome, not modifiable-does this mean we shouldn’t monitor it and intervene? Ø Mal-positioning of aortic cannula identifiable by NIRS. - does ‘modifying this change outcome?

Cerebral Near-Infrared Spectroscopy Monitoring and Neurologic Outcomes in Adult Cardiac Surgery Patients: A Systematic Review Why no stronger data? Ø Studies too few and too small. Ø Several different NIRS devices in use which are not be comparable. Ø Definition of ‘ischaemic levels’ not uniform or clear. Ø Most outcomes are time dependent.

Slater JP, Cerebral oxygen desaturation predicts cognitive decline and longer hospital stay after cardiac surgery. Ann Thorac Surg. 2009; 87 (1): 36 -44 Ø Powered for neurological outcomes but no difference in the de-saturation episodes between the control group and the study group. He therefore re-analysed the groups retrospectively and showed improvement in early neurocognitive and LOS outcomes. But not late. Ø This meant that it was impossible to say if the low r. SO 2 was a modifiable risk factor.

Predicting the Limits of Cerebral Autoregulation During Cardiopulmonary Bypass Joshi et al. Anesth Analg 2012; 114(3): 503 -10 Lower limits of autoregulation in 232 (7 no limit) patients using Cerebral Doppler and Correlating it with NIRS

Predicting the Limits of Cerebral Autoregulation During Cardiopulmonary Bypass Joshi et al. Anesth Analg 2012; 114(3): 503 -10 Lower limits of autoregulation in 232 (7 no limit) patients using Cerebral Doppler and Correlating it with NIRS

Predicting the Limits of Cerebral Autoregulation During Cardiopulmonary Bypass Joshi et al. Anesth Analg 2012; 114(3): 503 -10 • We cannot do cerebral Doppler but we can use NIRS • When NIRS falls below baseline then we are loosing autoregulation and closing the gap on MOM v. In 66 year old patients MAP 66 mm. Hg was lower limit of autoregulation

How does the stroke occur? Watershed strokes after cardiac surgery: diagnosis, etiology, and outcome Gottesman RF. Stroke. 2006 Sep; 37(9): 2306 -11 • Patients with a decrease in mean arterial pressure of at least 10 mm Hg (intraoperative compared with preoperative) were 4 times more likely to have bilateral watershed infarcts than other infarct patterns.

Why dispute in cardiac, Ø Watershed strokes after cardiac surgery: diagnosis, etiology, and outcome Gottesman RF. Stroke. 2006; 37(9): 2306 -11 • 98 patients with clinical stroke after cardiac surgery who underwent MRI with diffusionweighted imaging. • Explores the relationships between; MAP and watershed infarcts; infarcts and outcome; MRI versus CT

Why dispute in cardiac, Ø Watershed strokes after cardiac surgery: diagnosis, etiology, and outcome Gottesman RF. Stroke. 2006 Sep; 37(9): 2306 -11 • Bilateral watershed infarcts were present on 48% of MRIs and 22% of CTs (P<0. 0001). Perioperative stroke patients with bilateral watershed infarcts, compared with those with other infarct patterns, were 17. 3 times more likely to die.

In cardiac, trying to keep on track • Maintain a MAP that is right for the individual patient. Go figure. Ø Risk for impaired cerebral autoregulation during CPB and post-operative stroke. Ono, Joshi, Br J Anaesth 2012; 109: 391 -8 • 20% of patients had impaired autoregulation and a 12% incidence of stroke compared with 2% in normo-regulated patients.

Hypertensive 1 • Pre-anaesthesia MAP 144 • Initial fall. Good LV

Hypertensive 1

Hypertensive 1 What happens next?

• Patient on ICU moving all 4 limbs. Communicates. 2 hours post-op extubated. • One hour later not moving left hand. Weakness increases over 24 hours.

Right temporal Cerebral infarction

Next slice shows old lacuna infarctions

This was the trace, what could have been done differently? • • Better control preop Higher BP throughout Monitor bigger area Did we avoid a bigger infarct. • Renal function was good • Monitor post-op?

Cerebral oximetry and Bleeding BP 40 BP BP 100 35 mins

Hypertensive 2. 1 st BP over 200.

Hypertensive 2.

June 28 case 2015

CVP slowly rising. Surgical move corrected r. SO 2.

Next case-elective CABG

On Adrenaline BP 120 –r. SO 2 low 30 s. What next? Surgery just starting.

Adrenaline, next – change the ventilation. What happens when we go on bypass? p. CO 2 3. 9 k. Pa p. CO 2 5. 2 k. Pa

What happens when we go on bypass? p. CO 2 3. 9 k. Pa p. CO 2 5. 2 k. Pa

CO 2 or inotropes ET CO 2 was 4. 6 k. Pa

Next case Bilateral 70% carotid diseasesymptomatic. For CABG Just after induction r. SO 2 below 40. Needed to adjust CO 2, BP and on CPB Hb. 1 hour scale.

Bilateral 70% carotid disease-symptomatic. For CABG Constant adjustment. Kept r. SO 2 up she made a quick and complete recovery.

Bilateral 70% carotid disease-symptomatic. For CABG Constant adjustment. Kept r. SO 2 up she made a quick and complete recovery.

Common event

Unstable angina and carotid stenosis. Preop Sa. O 2 88%. What do you do?

Unstable angina and R carotid stenosis. Preop Sa. O 2 88%. What do you do?

Unstable angina and carotid stenosis. Preop Sa. O 2 88%. What do you do?

Routine Mitral Valve. 36 years old. Start of coffee break

A Guide to cardiac output. Routine AVR

Echo shows a patch on the posterior aortic annulus and a defect to the anterior mitral leaflet

What happened in INVOS?

INVOS crashes? • • • Go back on CPB? Give blood? Alter the CO 2? Give inotropes? Pacemaker? Shout at the surgeon?

Coming off CPB-home and dry

Optimizing intraoperative cerebral oxygen delivery using noninvasive cerebral oximetry decreases the incidence of stroke for cardiac surgical patients. Goldman S Heart Surgery Forum 2004; 7(5): E 376 -81 Ø We hypothesized that optimization of cerebral oxygen delivery variables by using noninvasive cerebral oximetry could reduce the incidence of stroke.

Optimizing intraoperative cerebral oxygen delivery using noninvasive cerebral oximetry decreases the incidence of stroke for cardiac surgical patients. Goldman S Heart Surgery Forum 2004; 7(5): E 376 -81 Ø Cerebral oximetry was used to optimize cerebral oxygen delivery (n = 1034, treatment group) to maintain r. SO 2 at or near the patient's pre-induction baseline. Ø Control, no cerebral oximetry (n = 1245)

Optimizing intraoperative cerebral oxygen delivery using noninvasive cerebral oximetry decreases the incidence of stroke for cardiac surgical patients. Goldman S Heart Surgery Forum 2004; 7(5): E 376 -81 Ø Study group NYHA classes III and IV. ØStudy group permanent strokes 10 [0. 97%] versus 25 [2. 5%]; p<. 044 Ø Study group requiring prolonged ventilation 6. 8% versus 10. 6%; p<. 0014 Ø Study group LOS shorter p<0. 046 Ø Statistical reduction in NYHA I-III

Thank you for your attention

Carotid endarterecomy. Left internal carotid. TIAs

Block goes in BP high. Fentanyl given, then BP drops with INVOS but still >110 sys. Breathing and then BP recover along with INVOS

Clamp goes on common carotid. Effects L INVOS immediately. But continues to squeeze the ball. So decide not to shunt.

INVOS continues to fall. In parallel the patient squeezes less and less. Shunt inserted and immediate improvement in Sats% followed a few seconds later in return of ball squeezing.

Shunt removed for final closure. Brief dip then clamp off and recovery

Finish with the R and L converging. Patient fully alert. ü Absolute match of intervention and r. SO 2 ü BP effects r. SO 2 above ‘normal’ autoregulation ü Absolute match of r. SO 2 and conscious level

Ø General anaesthesia does not contribute to long-term post-op cognitive dysfunction in adults: a meta analysis. Ind J Anaesth. Guay, 2011; 55: 358 -63 Ø Cognitive outcomes 7. 5 yrs after angioplasty compared with off-pump CABG. Sauer, Ann Thor Surg 2013; 96: 1294 -300 Rigorous 9 stage testing showed no difference between those randomized to surgery (GA) and angioplasty (no GA). No clear theory that cognitive dysfunction is related to hypoxia.

End result

Concept • Broad brush studies fail to prove that correcting decrements in r. SO 2 improve outcomes. • But higher r. SO 2 improve outcome. Why? Because it reflects pre-op cardiac function which predicts outcome and this does not change overall. (anaesthetic techniques can improve r. SO 2 short term). • Adverse events eg bleeding causing a stroke, position of cannula etc are modifiable but requires large studies to prove.

Thank you for your attention.

• Todays cardiac surgery is the success it is because it is the pinnacle of controlling survivable physiology in the face of massive insult made possible by modern drugs and monitoring.

Redo MV, AVR, TVR, ASD CVP 28, Sats 93. Can’t lie flat. Still trying to find access. What to do?

TOE shows

Redo MV, AVR, TVR, ASD. Inotropes, CVP 23, BP 93 still pre-bypass

Redo MV, AVR, TVR, ASD. Steep drop. Recovery. Drop. Long period on bypass.

Redo MV, AVR, TVR, ASD. Drops before bypass. ? ?

Redo MV, AVR, TVR, ASD. Drops again a few minutes after bypass. ? ? Next day…….

Redo MV, AVR, TVR, ASD. 36 hrs later post extubation


Comment on LV LVESWT =1. 6 cm

Next case LV SAX view

Now LV looks like this

What about this?

Unstable angina and carotid stenosis. Preop Sa. O 2 88%. Good result

Does the use of cerebral oximetry lead to an increased incidence of blood transfusion in adult cardiac surgery? ACTA November 2014 S. Bennett 1, M. Bennett 2, N. Smith 3 1 King Faisal Cardiac Centre, King Abdulaziz Hospital, Jeddah, Saudi Arabia 2 Newcastle University School of Medicine, Newcastle, UK 3 Castle Hill Hospital, Hull, UK

Results Number of patients transfused with homologous blood Age, years Pre-op Hb, g/l Total Bypass time, min Lowest temp, o. C Lowest Hb, g/l Total blood loss, mls Discharge Hb, g/l INVOS n=91 unless* 5 Non-INVOS n=88 unless* 3 P values 67. 5 (8. 81) 137 (14. 4) 79. 9 (36. 9) 32. 9 (2. 54) 97. 9 (19. 6) 756 (666) *n=90 96. 6 (15. 5) *n=90 66. 8 (11. 2) 137 (15. 1) 72. 1 (25. 8) 33. 0 (2. 86) 97. 3 (19. 0) 636 (552) *n=84 98. 2 (13. 5) *n=84 0. 617 0. 844 0. 102 0. 907 0. 828 0. 199 0. 459 0. 500 Table 1 Patient data for Cardiopulmonary Bypass and Homologous Blood Transfusion. Values are given as mean (standard deviation) or absolute values.

SHOULD WE GIVE BLOOD WHEN THE r. SO 2 falls? Letter JICS 2011: Transfusion of stored blood cells in critical illness: impact on tissue oxygenation

Emergency case. VT, diabetic, EF 35%, bilateral carotid disease, Hb 8. 3, creatinine 170, arteriopath, ST-elevation. 1. Inotropes v Noradrenaline? 2. Clear fluids v blood? 3. Operate, postpone, cancel? 4. Any change in plan?

Emergency case. VT, diabetic, EF 35%, bilateral carotid disease, Hb 8. 3, creatinine 170, arteriopath, ST-elevation. 1. Inotropes 2. Normal fluids 3. Shorten surgical time 4. Not great 30

Emergency case. VT, diabetic, EF 35%, bilateral carotid disease, Hb 8. 3, creatinine 170, arteriopath, ST-elevation. 1. More inotropes v IABP 2. More blood/plts 3. Better on bypass 30

Emergency case. • Outcome • Extubated 4 hrs postop neurologically intact. Passing urine. • 12 hrs post-op inotropes and fluids stopped 1. What happens next day?

Emergency case. • Outcome Day 1 • Urine output 10 mls/hr • Creatinine 210 advised to dialyse. • Dopamine and furosemide • Respiratory fine 1. What happens Day 2?

Emergency case. • Outcome Day 2 • Urine output 1020 mls/hr • Creatinine 250. Pushing fluids. • Advised to dialyse. • Dopamine and furosemide • Respiratory fine 1. What happens Day 3?

Emergency case. • Outcome Day 3 • Urine output 100 mls/hr • Creatinine 210 then 165. • Dopamine and furosemide stopped • Respiratory fine Ends with Hb 9. 3 after 5 units blood (4 in OR and 1 post-op)

What do you do? Arteriopath, MI last week followed by blackouts, no cause found. Next case June 29 2015

Hypertensive Case Pre-op BP 220/100 and sats 51/41.

Acute pericardial effusion. 36 yrs very low baseline 34/30. Effects of pre-O 2. Anaesthesia but then a dip. Not usual. What happens next?

Acute pericardial effusion. CVP down Arterial pressure up. What happens to INVOS?

Acute pericardial effusion. CVP down Arterial pressure up. INVOS directly reflects cardiac output?

Don’t give up!

European guidelines on management of PE. 2008 Euro Heart J

The whole set-up

We used Cerebral Oximetry to guide management and weaning. Day 2 attempt

Cardiac output paradigm ü If NIRS >50% and Sa. O 2 >95% then CO fine ü If NIRS >50% with low Sa. O 2 then probably hypoxic but not due to low CO ü If NIRS <50% and Sa. O 2 low then hypoxia and CO inadequate. v. If NIRS <50% and Sa. O 2 >95% then CO inadequate.

What would you do next? r. SO 2 has just dropped below baseline before surgery Your text here Et. CO 2 low. Pa. CO 2 4. 8

r. SO 2 below baseline. Options • Correct Et. CO 2 - Pa. CO 2 4. 8 k. Pa • Systolic pressure: preop 190 mm. Hg now 150 • Sa. O 2 -100% • Cardiac Output? • Volume colloid? Blood?

r. SO 2 below baseline. Options

Cardiac Output?

Volume. Clue bottom left

End result

It tells us the oxygenation of the finger or even the toe!



What about sick patients on ICU? Just after intubation Sa. O 2 79% 24 hrs later Sa. O 2 94%

Is this a stroke? 65% 38% • Mitral valve. • Woke with a Left hemiparesis. Not complete. • CT negative x 2

Is this a stroke? DW MRI scan • Left hemiparesis. • Small lesion deep in the Right cerebral hemisphere. • Are we ever going to be able to stop this?

Early warning system? • The STS Adult Cardiac database began collecting cerebral oximetry data in January of 2008 • Initial database findings showed that in over 23% of the 36, 548 procedures submitting cerebral oximetry data, “cerebral oximetry provided the first indication of a technical problem or physiological change in the patient that could potentially lead to an adverse patient outcome. ” www. sts. org/document/Adult. CVDataspecification

Not just early warning on bypass. Minimal access MVR bypass

INVOS suddenly 20 s despite normal BP. HR to 20, manual pacing for 20 mins. Despite complete heart block as we were closing.

Or even earlier? • Perhaps not to operate. • Frail 41 kg. 72 yrs old. • Good LV, renal OK, no strokes, nonsignificant carotid dis. • • • Preop L R 38 38 Pre-bypass 40 41 On-bypass 50+ Post bypass 41 43 • 12 hours post extubation grandmal seizure and stroke

‘Better to shine the light, than curse the darkness’. • Murkin J. • Editorial. Euro J Cardio. Thorac. Surg 2013 • There remain many gaps if what we would like to achieve. NIRS bridges some of these gaps and is the current best step forward in reducing post-operative morbidity and mortality.

Conclusion • Avoiding cerebral desaturation during surgery is a good thing. Unless you monitor it you have no idea what is happening. • It is an indirect, complication free monitor of cardiac output. • Cannot improve individual outcomes purely on population based data.

Thank you for your attention

Other cases 1. De-saturation during mammary harvest 2. De-saturation during aortic dissection requiring bilateral carotid cannulation 3. De-saturation during circulatory arrest. In all cases active intervention lead to excellent outcomes.

Which one today?

Are we in full control? What causes this decline? MICRO BUBBLES? Cerebral micro-embolism most likey cause of neurocognitive dysfunction Anesth Analg 2009: 109: 320 -30

What more do we need before r. SO 2 is routine? Ø Double blind clinical trials. Murkin and Slater studies and/or Ø Direct evidence of cause and effect. I have seen disasters develop resulting in stroke and death. v Slater. Cerebral oxygen desaturation predicts cognitive decline and longer hospital stay after cardiac surgery. Ann Thorac Surg. 2009 Jan; 87(1): 36 -44 v Murkin. Monitoring brain oxygen saturation during coronary bypass surgery: a randomized, prospective study. Anesth Analg. 2007 Jan; 104(1): 51 -8.

Existing work • Relatively small groups. • Outcomes disappointing. • Length of stay and early neurological outcome. • But these groups were low risk CABG patients and yet we seem to accept INVOS in ‘high risk’ groups.

Is there a need for more randomised studies? • With reference to Murkin and Slater papers. ØIntervene early and hard. ØPowered for LOS and neurocognitive decline ØThe brain as an index organ? - too much noise later. Protecting the brain is good enough for a monitor ØIt is a transfusion trigger.

Double blind, randomized, control trail in elective cardiac surgery • 182 patients, pre and x 2 post op neurocognitive testing. Stroke, LOS. • Underway but surgeons now insisting that we have INVOS for more cases.

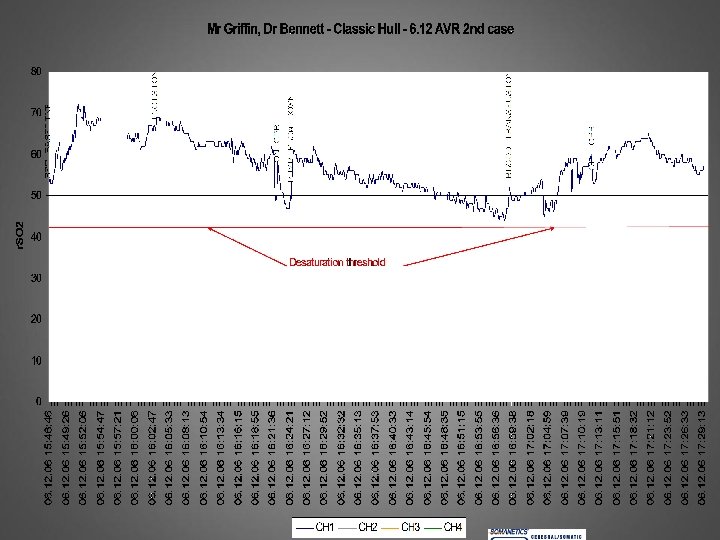
Final case • Routine CABG: found to have calcified aorta. Surgeon managed to find a soft spot. • Post op on ICU we had NIRS monitoring

NIRS trace post op

Brief NIRS on day 7

What about sick patients on ICU? Just after intubation Sa. O 2 79% 24 hrs later Sa. O 2 94%

Other cases 1. De-saturation during mammary harvest 2. De-saturation during aortic dissection requiring bilateral carotid cannulation 3. De-saturation during circulatory arrest. In all cases active intervention lead to excellent outcomes.

It gives me 2 unique pieces of information • 1. What flow does the patient tolerate (not what flow the surgeon asks for!) • 2. What Hct is tolerated by the patient (not a population guess)

Patients where is it used? Peri-operative period: Ø Cardiac surgery üVascular surgery üCardiac Cath Lab üNeurology / Neurosurgery (sitting) üGeneral surgery üSpinal injury

Intervention protocol Specific changes in bypass management. • Pump flow to be re-calculated to ensure flow is 2. 4 l/m 2/min/ or greater. • Mean pressure increased to 60 mm. Hg using metaraminol in the first instance. • Pa. CO 2 increased to 5. 3 mmol. • Fi. O 2 increased to 1. 0 • Depth of anaesthesia: all patients will be anaesthetised with a minimum of 1% isoflurane during CPB, this will be increased to 2 and 3%. • Transfusion if haematocrit <25%. • Change of surgical plan

Early days • At present it is on a separate display, but it is clear. (Minimum monitoring on CPB) • Does not help with focal events only generalised neuro dysfunction which is more common. • Would you like to have it for your cardiac bypass without r. S 02 monitoring?

Hard to believe

Pre-oxygenation works

How did the case go? 30

Regional cerebral saturation monitoring with nearinfrared spectroscopy during selective antegrade cerebral perfusion: diagnostic performance and relationship to postoperative stroke. Olsson C. J Thorac Cardiovasc Surg. 2006; 131(2): 371 -9 • 46 patients, 6 died, 6 had a stroke • Regional cerebral tissue oxygen saturation between 76% and 86% of baseline had a sensitivity up to 83% and a specificity up to 94% in identifying individuals who recovered with a stroke.

VSD repair- again better on bypass. BLEEDING

Bleeding post bypass

Is this a stroke in waiting?

Cases Ø 1. Wrong cannulation or errors at cannulation site Ø 2. Wrong positioning of mammary retractor Ø 3. Wrong flows/cannula position on ECMO or any mechanical assist

Intervention protocol Specific changes in bypass management. • Pump flow to be re-calculated to ensure flow is 2. 4 l/m 2/min/ or greater. • Mean pressure increased to 60 mm. Hg using metaraminol in the first instance. • Pa. CO 2 increased to 5. 3 mmol. • Fi. O 2 increased to 1. 0 • Depth of anaesthesia: all patients will be anaesthetised with a minimum of 1% isoflurane during CPB, this will be increased to 2 and 3%. • Transfusion if haematocrit <25%. • Change of surgical plan

Bold- restrictive fluids; light normal. Y-axis Hct. Xaxis time. Result; less blood used in restrictive fluid

Slater JP, Cerebral oxygen desaturation predicts cognitive decline and longer hospital stay after cardiac surgery. Ann Thorac Surg. 2009; 87 (1): 36 -44 Ø Definition of hypoxia or desaturation threshold. % time in seconds below the average for all the patients. Average was 50%. Therefore 40% r. SO 2 for 300 secs = 3, 000%secs. Slater says it is only then that problems arise and staying above this is safe- therefore it is modifiable.
fec3c51f0148e0728c4120d04eac2414.ppt