6f33c2dc99437d71df83b34bf1603c59.ppt
- Количество слайдов: 53



CBP End of Life Neil Mclean Feb 4, 2010

Case • A 32 -year-old Asian male is brought into the ICU after a 14 -hour attempt at an IC-MCA bypass for a giant cerebral aneurysm. The surgery did not go well and his graft clotted completely. He is now in the ICU and CT and MRI have demonstrated a diffuse anoxic brain injury. He still has brainstem reflexes and is not brain dead. A neurological opinion has confirmed no prognosis for meaningful recovery.

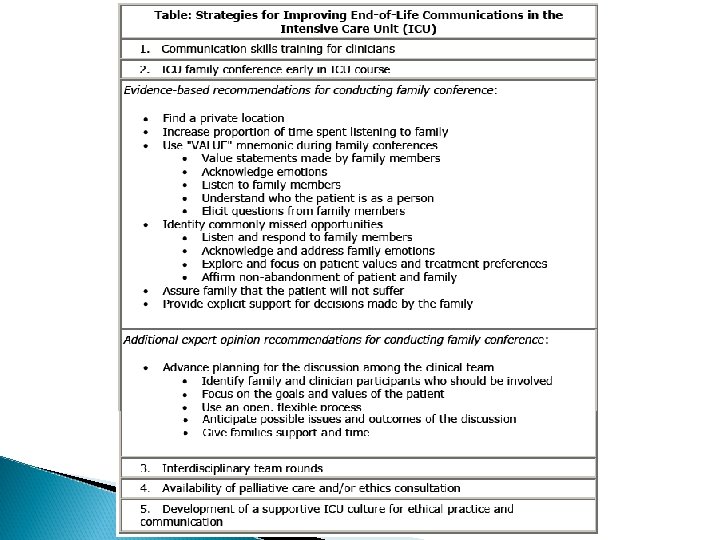
What are some key strategies to implement when discussing withdrawal of care in the ICU? Focus on the family meeting (ERIK)

End of Life in the ICU Case Based Presentation: • The Family Meeting

Setting the stage Prior studies have shown that < 5% of ICU patients are able to communicate with clinicians at the time that decisions are made about withholding or withdrawing lifesustaining therapies. Therefore, when ICU clinicians must discuss these issues, they often discuss them with patients’ families.

RN foundation in the ICU

✔ ✔ F. I. F. E. -erize them! ✪ ✔✔

Ethics Four guiding principles 1. 2. 3. 4. Autonomy Beneficence Non-maleficience Justice

Consulting Services It can be beneficial to have them represented at the family conference. However, the family conference is not the forum for debating issues about prognosis and therapy. Disagreements about patient care generally should be resolved between clinicians before the family conference.

Deep thoughts… • “…care vs cure…only different in one letter but their difference in meaning…” Vu-diggity (PICU model) • • • “…from cure to comfort…. ” J. Curtis “Patients [and their families] don’t care how much you know, they just want to know that you care” B. Mohr “No information is better then misinformation” R. Arseneau
, the wife tells you")
When you meet with the family (wife and parents), the wife tells you that her husband told her that he did not ever want to be a “vegetable”? What is an advanced directive? (FEDERICO)

Discuss the controversies of Advanced Care Planning as it pertains to the ICU? (TODD)

Advance Care Planning in the ICU Decisions regarding intensity and duration of care made under a variety of circumstances, and may not be applicable to critical illness. ◦ Advance directives made while well and independent are usually hypothetical exercises, and/or based on the experiences of loved ones.

Advance Care Planning: Challenges in Critical Care Setting • • Patients often end up in ICU whether they like it or not… “DNR” is appropriate for sudden cardiac death or catastrophic injury, but once patients are in ICU, it is more common for deterioration to take place over hours to days. – Or weeks to months… • It is impractical to specify wishes for any given scenario. – i. e. “Do everything, but not if you don’t think I’ll survive…” – The unexpected (especially the unexpectedly bad) is to be expected.

Know When To Say “When” • The timing of advance directives is crucial. – Example: Wishes expressed when independent may not reflect patient’s wishes if significant disability (i. e. injury, stroke) arises. – Example: Laryngeal CA patient with “No CPR/ETT/ ICU” documented prior to ENT consult suggesting that tumor was resectable with potential cure. As a result, revisited advance directive was upgraded. • Changes mid-stream may be required, as the patient’s situation worsens or improves. – “Cast in stone” directives may not therefore apply

What About Real-Time Directives? Perhaps taking advance directive in context of overall history, presentation, treatment plan and prognosis is a better strategy, especially with family/reliable SDM available. ◦ As the situation evolves, the patient’s wishes may change. Doing “everything” may not really mean everything.

Do Advanced Directives work? “Death Panels” “Nancy Cruzon” PDSA In US SUPPORT Study ◦ Retrospective and intervention ◦ Conclusions Physicians not aware or involved No change in care Better documentation of AD but were not followed

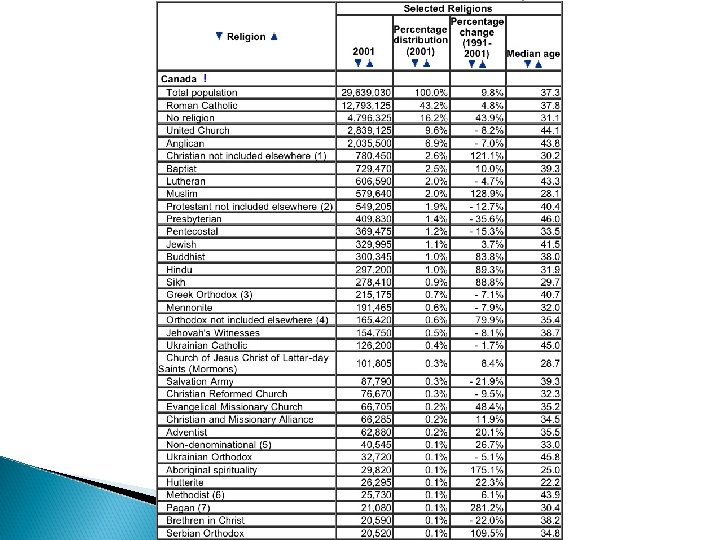
As your discussion continues, the patients parents are strongly against withdrawing care and are convinced a miracle will happen Discuss end of life issues with respect to the influences of religion (IBRAHIM)

Religions’ Influences on EOL decisions in ICU Ibrahim Momen. Khan

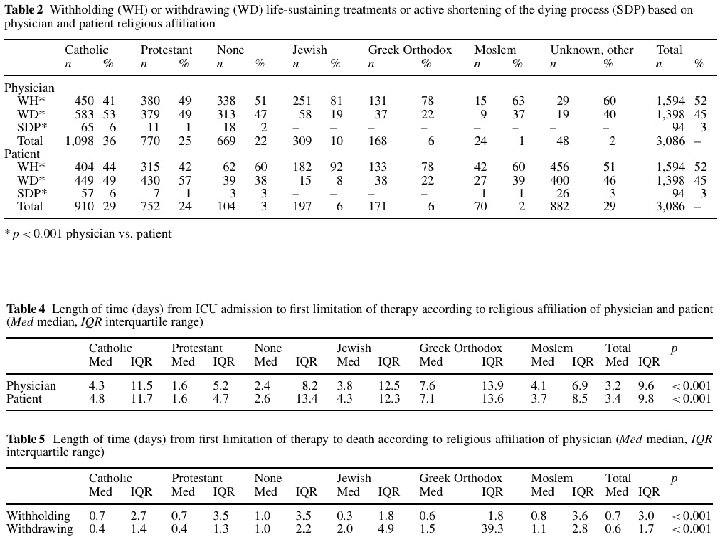
References The world’s major religions’ points of view on endof-life decisions in the intensive care unit, Bulow et al, Intensive Care Med. 2008 The importance of religious affiliation and culture on end-of-life decisions in European intensive care units, Sprung at al, Intensive Care Med. 2007

Both patients families and physicians are influenced. Different opinions exist within populations of same religion! Health care professionals should be aware of the major religion’s POV in regards to critical decisions, such as EOL issues.

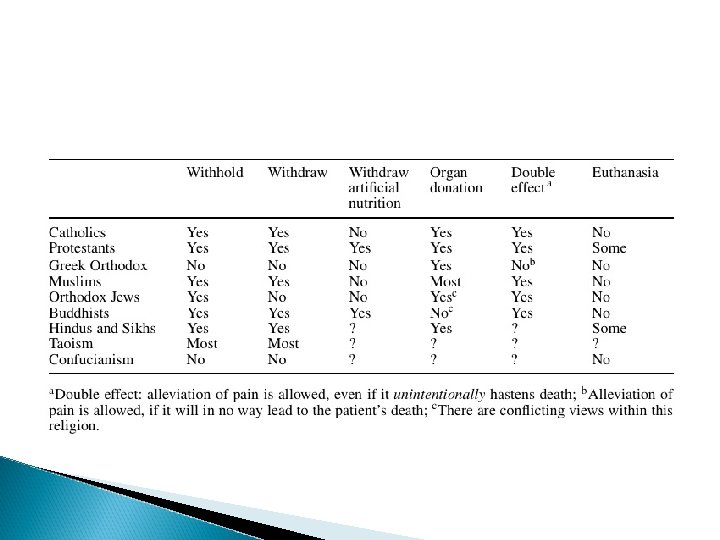
Some Definitions Futile: adj. having no purpose because there is no chance of success Oxford Dictionary Euthanasia: comes from the Greek for “good death”, and the Greek Orthodox Church defines good death as a peaceful death with dignity and without pain. On the contrary, the current international meaning of “active euthanasia” is perceived rather as “mercy killing”. Double effect: Alleviation of pain, even if unintentionally results in death.
; allowed withholding and withdrawing of FUTILE therapy if")
Catholics Pope John Paul II (1996); allowed withholding and withdrawing of FUTILE therapy if it is burdensome, dangerous, extraordinary or disproportionate to the expected outcome. But, against withdrawing nutrition for chronic vegetative state.

Protestants If “little hope” it’s okay to w/d. Theologians in the reformed tradition, e. g. in the Netherlands, defend active euthanasia.

Greek Orthodox Death is not as a biological event but as a mystery with a sacred, spiritual character and as a great blessing. For human to decide anything to do with death is insult to God, beside of the potential human error and “unforeseen miracles”. D/C M. V only Okay in confirmed brain dead, and organ donation, only with patient or family consent. Some of their ruling is similar to some Muslim scholars (Azhar, Egypt).
, and withholding")
Jews Difference between withdrawal (sustained therapy, like mechanically ventilated patients in ICU), and withholding (intermittent therapy, like intubation, chemo, surgery). So to make M. V changes from “sustained” to “intermittent”, connect it to a timer, and then can “withhold”, which is allowed! Feeding is not therapy but basic need, so not allowed to d/c, unless there is patient’s informed consent.

Muslims Similar to Catholics, only if futile therapy and inevitable death, by the decision of 3 physicians. For the brain dead, requires the strict and documented definition, and consider no death till “cardiac arrest”, after which harvesting can take place. D/C M. V is allowed in the confirmed brain dead, which will lead eventually to cardiac arrest and then harvesting can take place (CIJA, ISNA, others). “For that cause We decreed for the Children of Israel that whosoever killeth a human being for other than manslaughter or corruption in the earth, it shall be as if he had killed all mankind, and whoso saveth the life of one, it shall be as if he had saved the life of all mankind” (Qura’an, 5: 32). This verse also shows that euthanasia is forbidden.

If not futile, and thought to be treatable case, it is strongly deferred (most say forbidden, Azhar and others), even if it was the patient wish to withhold or withdraw therapy and patient should be urged to take the treatment. “and be not cast by your own hands to ruin; and do good. ” (Qura’an, 2: 195). Nutrition is a basic need and starving the patient may make them suffer, so not allowed to d/c “no harm and no harassment” (Mohammad PBUH), and this also indicates that “double effect” is allowed.

Hindu and Sikh Hindu: No single central authority, different opinions exist. Sikh and Hindu share duties but not rights Both believe in “karma”, good acts and thoughts lead to good rebirth, bad lead to bad.

ICU death is considered “bad death” (premature, not at home, signified by vomit, feces, and urine). So, DNR is acceptable to avoid such “bad death”, and to hasten spiritual purification and detachment. Euthanasia is illegal by law, which is derived from the British ruling, but longstanding tradition in certain cases still approve it, also to avoid “bad death”.

Chinese Confucians: Death is good if one has fulfilled one’s moral duties in life, and resistance to accept terminal illness or insisting on futile treatment may reflect the patient’s perception of unfinished business. Taoism: Philosophical: death is simply accepted naturally and no need to prolong the process. Religious: Death will lead to afterlife torture in hell, so cling to any mean of life sustaining measures to postpone that.

Buddhists Most moral issues acculturated locally as there is no central authority. The believe of immortality led to acceptance of w/d of life sustaining measures. Western Buddhists accept organs donation.

How to Cope? “The key to resolving ethical problems lies in clarifying the patient’s interests” Stanford Univ. Ethical Committee Klessig, West J Med. 1992

At one point, during your discussion, the patient’s father states that ‘in our culture we value life” Discuss some of the influences of culture on attitudes towards dying and withdrawal of care, especially in ICU patients (NOEMIE)

AAFP policy statement on ethical principles of EOL care: “ Care at the end of life should recognize, assess, and address the psychological, social, spiritual/religious issues, and cultural taboos realizing that different cultures may require significantly different approaches. ” Am Fam Physician 2005; 71: 515 -522

Basic dimensions in EOL treatment that vary culturally “Communication of bad news” “Locus of decision making” Attitude towards advance directive and EOL care” Am Fam Physician 2005; 71: 515 -522

Communication of bad news Emphasis on pt informed consent and “truth -telling” In certain cultures, family protects their loved one from knowledge of their condition ◦ Hispanics, Chinese, Pakistani, Native American. ◦ Special status of the elderly ◦ Importance of a translator Am Fam Physician 2005; 71: 515 -522

Four reasons for non-disclosure: Certain cultures may ◦ view discussion of serious illness and death as disrespectful or impolite ◦ believe open discussion may provoke unnecessary depression or anxiety ◦ Believe that direct disclosure may eliminate hope (Bosnia, Philippines) ◦ Believe that speaking about a condition in a hypothetical sense makes death or terminal illness real (Bosnia, Philippine, Native americans) Am Fam Physician 2005; 71: 515 -522

Locus of decision making Emphasize pt autonomy Alternate decision making models ◦ Family-based (eg. Koreans, Mexican) ◦ Physician-based (eg. eastern European) ◦ Physician-family (eg. India, Pakistan) Some cultures value beneficence and nonmaleficence > autonomy. Am Fam Physician 2005; 71: 515 -522

Advance Directives and EOL care 40% of US Caucasian elderly have advanced care directives 16% of US African American have advanced care directive ◦ ? Mistrust of medical system Family-based decision model ◦ Involved the whole family in the decision Am Fam Physician 2005; 71: 515 -522

Am Fam Physician 2005; 71: 515 -522


The family turns to the surgeon at the meeting and asks why he can’t to do more surgery to fix his brain Discuss the issues around surgical “buy in” with respect to withdrawal of care on their patients (MARIOS)

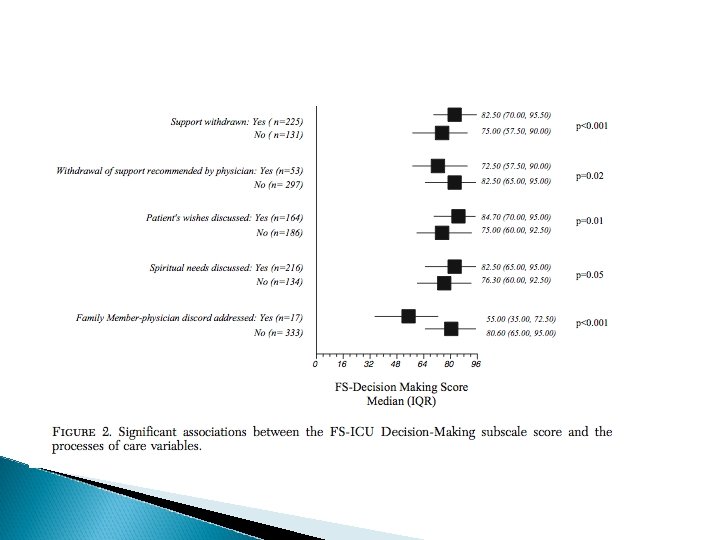
• • • After much discussion and numerous meetings the family comes to you and states that they agree that you should move to comfort care and the patient passes away without issue Discuss the current literature on factors that improve patient and family satisfaction in the ICU, focusing on end of life decisions (OMAR)

Factors associated with improved patient and family satisfaction Higher severity of illness Providing emotional support Good communication Offering spiritual care Being involved in decision making process of withdrawing support

Early identification of poor outcomes Documentation of family conferences Lower nurse : patient ratio

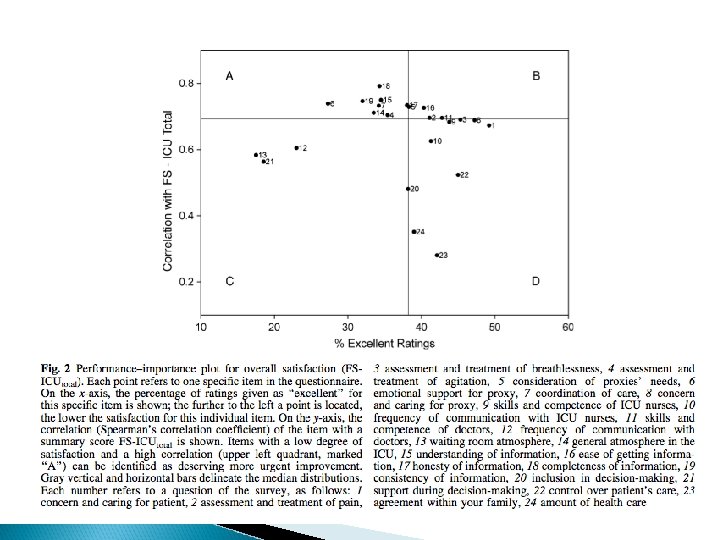
FS-ICU Family satisfaction in the intensive care unit 24 items filled in by pt’s and scored (0 -100)
6f33c2dc99437d71df83b34bf1603c59.ppt