e976c9f3fd8f3b2f8df89d57c4f73b4f.ppt
- Количество слайдов: 22



Case Presentation: Myelomeningocele Stephen Confer, MD Ben O. Donovan, MD Brad Kropp, MD Dominic Frimberger, MD University of Oklahoma Department of Urology Section of Pediatric Urology

Case Presentation • NICU Consultation • HPI : 1 day old male transferred to NICU from outside facility – No prenatal history available – Identified to have myelomeningocele – Going to OR in am with Neurosurgery

Case Presentation • PMHx – Denies prenatal US – ‘Normal’ Prenatal Course – Good Apgars – Good amniotic fluid from birth –per report • Social Hx – Small Town – 21 yo Non smoker – Denied alcohol and illicit drug usage – Single, no children • Medications : – ES Tylenol PRN

Case Presentation • Family Hx – No malignancy • ROS As in HPI

Physical Examination • Vitals signs : AFVSS • General : NAD • GU: uncirc, bilateral testes descended • Abd : ND, no masses, no hepatosplenomegaly. No inguinal hernia, umbilical stump is clear • Ext : No edema or cyanosis. MAE x 4 • Back: large patch of irregular tissue at midline


What would you recommend?

General Recommendations • • Renal Ultrasound VCUG CIC times 3 Baseline Urodynamics

Types of Myelodysplasia* • Spina bifida occulta • Lipomeningocele • Myelomeningocele = Spina Bifida *defective development of the spinal cord
 A condition involving nonfusion of the")
Neurologic pathology Spina bifida occulta (occulta = closed) A condition involving nonfusion of the halves of the vertebral arches without disturbance of the underlying neural tissue
 lipoma or fatty tumor located over the lumbosacral")
Neurologic pathology Lipomeningocele (lipo = fat) lipoma or fatty tumor located over the lumbosacral spine. Associated with bowel & bladder dysfunction Lipomeningocele
 Fluid-filled sac with meninges involved but neural tissue")
Neurologic pathology Meningocele (cele = sac) Fluid-filled sac with meninges involved but neural tissue unaffected

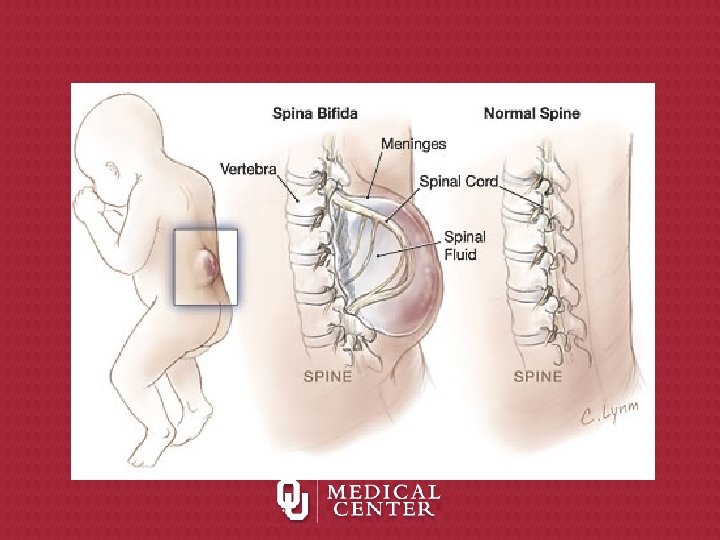
Types of Myelodysplasia Myelomeningocele or spina bifida: meninges and spinal tissue protruding through a dorsal defect in the vertebrae

The spinal defect with myelomeningocele

Incidence and Prevalence • Incidence – 1/1000 • Prevalence – Increased incidence in families of Celtic and Irish heritage (genetic or environmental? ) – Increased incidence in minorities (genetic or environmental? ) – Increased incidence in families

When do neural tube defects occur?

Neural Tube Development Normal embryological development ÞNeural plate development -18 th day ÞCranial closure 24 th day (upper spine) ÞCaudal closure 26 th day (lower spine)

Preventive Care • The United States Public Health Service recommends that: "All women of childbearing age in the United States who are capable of becoming pregnant should consume 0. 4 mg of folic acid per day for the purpose of reducing their risk of having a pregnancy affected with spina bifida or other neural tube defects. " Folic acid is a "B" vitamin that can be found in such foods as: cereals, broccoli, spinach, corn and others, and also as a vitamin supplement.

Clinical Considerations What factors contribute to neural tube defects?

High Risk for Renal Injury • Increasing age, evidence of hydroureteronephrosis and vesicoureteric reflux, high leak pressures, and low bladder volume define a high risk bladder in our population and predispose to renal injury in patients of myelodysplasia. • Early referral for bladder risk assessment and management of all myelodysplasia patients is recommended. Indian Pediatr. 2007 Jun; 44(6): 417 -20. Risk factors for renal injury in patients with meningomyelocele. Arora G, Narasimhan KL, Saxena AK, Kaur B, Mittal BR.

Future Directions? Support M M Clinics & Research
e976c9f3fd8f3b2f8df89d57c4f73b4f.ppt