86abef49ce6b35e11ff48021c65a3c19.ppt
- Количество слайдов: 57



CASE MANAGEMENT • JUNE 16, 2014 Dr. Lulubel F. Ilagan Second year resident

General Data: • • • JC 5 months old, female Filipino Catholic Hagonoy, Bulacan

Enlarging Mass on Upper Lip

History of Present Illness At birth At 1 month - reddish, elevated skin lesion, less than 5 mm with irregular borders on the lip, lateral to the philtrum, left - size: 1 x 1 cm with elevation and thickening -pediatrician: hemangioma. 3 months old - 3. 5 x 3 cm, violet-red, causing slight eversion of the left side of the upper lip. - referred to a hematologist

Example* PREDNISONE Upon birth size color character 1 month 2 month 4 month
 - prednisone at 2")
History of Present Illness - Doppler UTZ - CBC (normal) - prednisone at 2 mg/kg/day 4 months old - Followed up - Decrease in size to 2. 5 x 2. 0 cm, lighter in color 5 months - Followed up - Prednisone stopped due to ulceration - Increasing in size

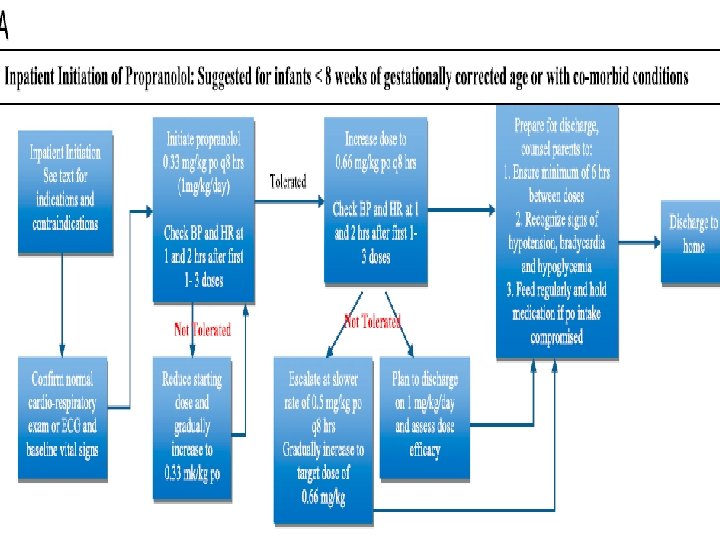
History of Present Illness Advised to start propranolol Day of Admission 2 d Echo done

Review of Systems • General: No weakness, no fever, no weight loss • Skin: No pruritus, no jaundice, no easy bruisability • HEENT: No headache, no dizziness, no hearing loss, no epistaxis, no hoarseness, no excessive salivation, no blurring of vision • Neck: No pain, no limitation of movement • Respiratory: No cough, no colds, no difficulty of breathing • Cardiovascular: No palpitations, no easy fatiguability, no chest pain • Gastrointestinal: , no diarrhea, no hematemesis, no melena, no hematochezia Endocrine: No polyuria, polydipsia, polyphagia • Genitourinary: No discharge, no incontinence, no dysuria • Musculoskeletal: No limitation of movement, no joint pains • Nervous system: No behavioral changes, no seizure • Hematologic: No bleeding, No bruising
")
Birth and Maternal History • • 29 -year old, G 1 P 1 (1001) Prenatal checkup - 2 months AOG; health center Nonsmoker, nonalcoholic beverage drinker Ultrasound – 3 rd trimester: normal Second trimester – cough for 5 days Delivered term, spontaneous vaginal delivery at a lying-in clinic Newborn screening - normal

Nutritional History • Mixed feeding for < 1 month bottlefed • Complementary feeding - 4 months, cereals • At present: Bonna, 1: 2 dilution, 4 oz q 3 h • Served daily with mashed potato, banana, or cereals at least twice/day • Given multivitamins and ascorbic acid daily.

Immunization History • BCG: 1 dose

Past Medical History • No previous admission • No previous surgical procedure • No allergies

Growth and Developmental History • Gross Motor: good head control at 3 months; rolls over at present • Fine motor: Grasped objects at 4 months • Adaptive: social smile at 2 months of age. • Language: cooed at 3 months
 DM – maternal grandmother")
Family History 29 27 Father: fish retailer Mother: housewife (+) DM – maternal grandmother (+) HPN – paternal grandfather (-) vascular lesions (-) bronchial asthma

Environmental History • • • 2 -bedroom, well lit, well ventilated house 3 other household members Purified drinking water Garbage collected 3 x times/day No nearby factories With exposure to cigarette smoke •

Physical Examination General Survey: Awake, not in cardiorespiratory distress Vital Signs: BP: 90/60 CR: 102 RR: 24 Temp 36. 2 degrees Celsius Anthropometrics: Weight: 6. 4 kg (z score 0) Height: 65 (z score 0)

Physical Examination • Skin: Violet-red mass, nontender, 4. 5 x 4 cm, with irregular borders on the upper lip, lateral to the philtrum • Head: Open anterior fontanel about 1 x 1 cm, soft and flat, pink palpebral conjunctivae, anicteric sclerae, no alar flaring, violet-red mass, nontender, 5 x 4 cm, with irregular borders on the upper lip, lateral to the philtum, no cervical lymphadenopathy

Physical Examination Chest: Symmetrical chest expansion, no retractions, clear breath sounds Heart: Adynamic precordium, normal rate and rhythm, no murmurs Abdomen: Globular, normoactive bowel sounds, soft, non palpable liver and spleen Extremities: Warm, pulses full and equal, crt<2 sec

Physical Examination Neurological Examination MSE: Calm, appropriately dressed Cranial Nerves: pupils 2 -3 mm equally reactive to light, extra ocular muscles are full and equal, good masseter tone, can smile with no facial asymmetry. Patient turns to sound, can turn head side to side with good gag. Motor: symmetric movement of all extremities Reflexes: Deep tendon reflex 2+ on all extremities Meningeals: No Babinski, no nuchal rigidity Autonomics: No excessive sweating

Salient Features • 5 months old, Female • Violet-red mass on upper lip, increasing in size • Treated with hydrocortisone

Working Impression • Hemangioma, left upper lip

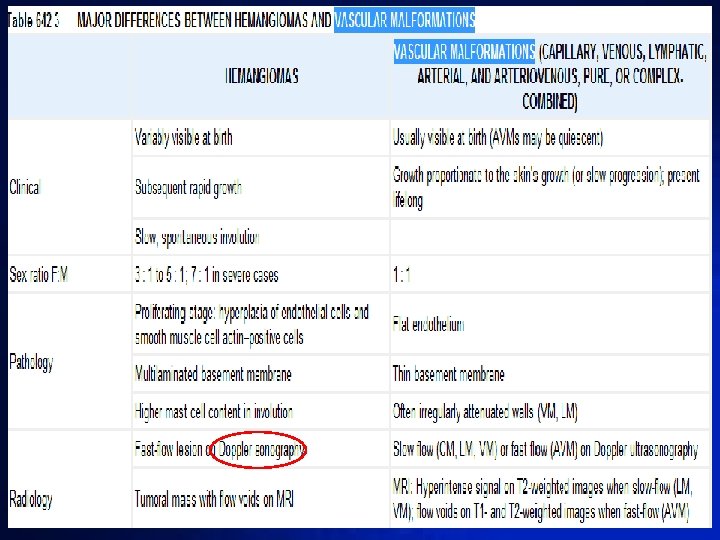
Vascula r lesions Birthmarks Nevus Café-au-lait Cutaneous lesions -Benign acquired disorders - Genetic disorders - Vascular birthmarks

Benign Acquired disorders Pyogenic granuloma, angiokeratoma of mibelli, spider angioma Genetic disorders Blue-rubber bleb, Malfucci syndrome, Osler-Weber-Rendu disease Vascular lesions Malformation Vascular birthmarks Tumors

Vascular tumors • most common is hemangioma Vascular Birthmarks • developmental error Vascular in blood vessel formation Malformat • do not regress but ion slowly enlarges

Vascular Tumors Hemangioma Tufted Angioma Kaposiform hemangioend othelioma Diffuse Hemangioma

Vascular Tumors Hemangioma Tufted Angioma Kaposiform hemangioend othelioma Diffuse Hemangiomatosis Numerous hemangiomas are widely distributed

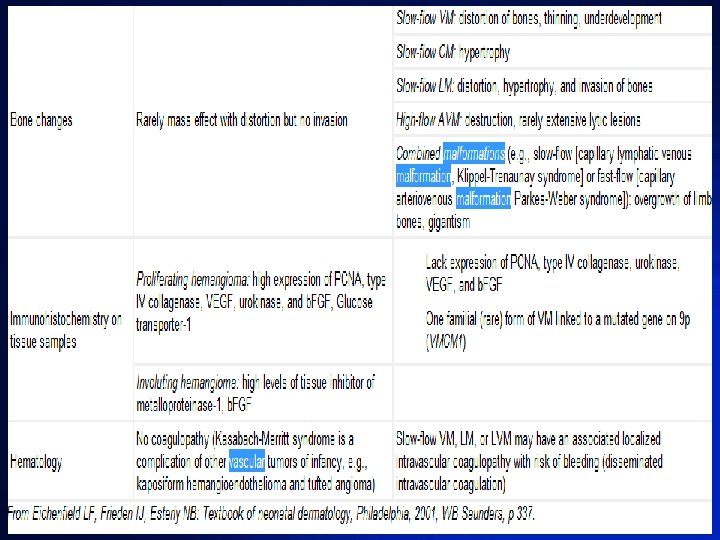
Vascular Tumors Hemangioma Tufted Angioma Kaposiform hemangioend othelioma -Very aggressive locally -Solitary, firm and deep purple -Do not regress spontaneously -Associated with Kasabach-Meritt syndrome Diffuse Hemangioma

Vascular Tumors Hemangioma Tufted Angioma Kaposiform hemangioend othelioma Diffuse Hemangioma - Histologically: “cannonball-like tufts of blood vessels - Slowly expanding dusky reddish-blue plaque with satellite lesions (regression not expected) or solitary vascular nodule

Vascular Tumors Hemangioma Tufted Angioma Kaposiform hemangioend othelioma Diffuse Hemangioma Most common tumor of infancy (5% of all infants) Proliferation of the vascular endothelium

• J. C. - Precursor lesion at birth - Rapid growth - F>M

Classification • SUPERFICIAL - bright red, protuberant, compressible, sharply demarcated • DEEP - more diffuse, less defined; cystic, firm overlying skin may appear normal or with bluish hue

PHASE 1. Rapid expansion/ Proliferative phase 2. Stationary phase 3. Involution - not correlated with size or site - lesions on the lip seem to persist most of the time

• Reminder: • If may literature sources ka, don’t forget to acknowldege author at the bottom. . • Eg. Ilagan et al 2010

PATHOPHYSIOLOGY - Not elucidated - Proliferation of benign endothelial like cells that possess histochemical markers (GLUT-1, Lewis Yantigen, Fcy. RII and merosin - present also in placental BV

PATHOPHYSIOLOGY PLACENTAL THEORY - explains programmed life cycle - genetic similarity ENDOTHELIAL PROGENITOR CELL (EPC) THEORY - increased circulating EPC - Human IH EPC injected to mice

SYNDROMES ASSOCIATED WITH HEMANGIOMA PHACE SYNDROME - GORHAM posterior fossa brain defects, hemangioma, arterial malformations, cardiac, eye abnormalities (sternal raphe defects/ supraumbilical raphe) - cutaneous hemangiomas with massive osteolysis - macrocephaly lipomas, hemangiomas of autosomal dominant inheritance BANNAYAN-RILEY-RUVALCABA

TREATMENT • OBSERVE • INDIVIDUALIZE - sign of regression: - Cochrane analysis “lack of well-designed blanched or pale gray - 60% involutes at 5 years old clinical trials and the absence of US FDA- 90 -95% - 9 year old approved medications IH, limits ability to clearly identify the single best option”.
 Segmental")
HIGH RISK INFANTILE HEMANGIOMA Location Type Growth Phase Periorificial (eyes, nose, mouth *) Segmental Maximal Proliferation phase (usually 3 -6 months) Central Facial Multiple Lumbosacral Rapidly proliferating Genital

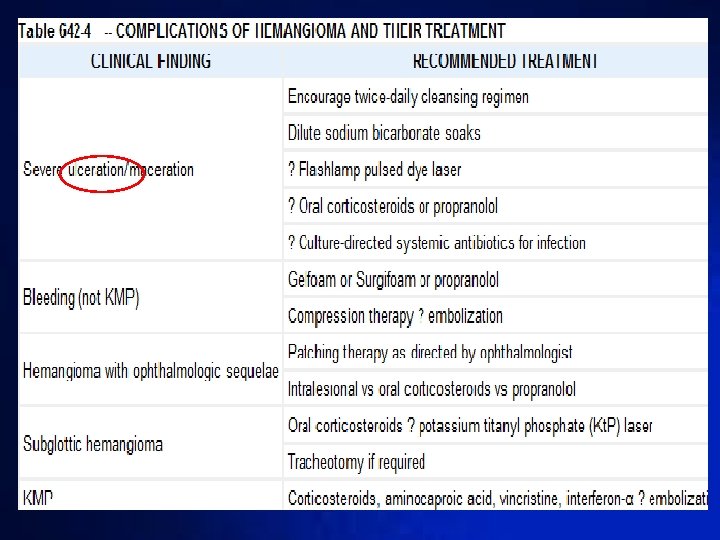
RATIONALE FOR TREATMENT 1. To prevent or improve functional impairment or pain 2. Prevent or improve scarring and/or disfigurement* 3. To avoid life-threatening complications

TREATMENT • CORTICOSTEROIDS • - 1960 s Prednisone 2 -3 mg/kg/day Regression evident after 2 -4 weeks * Response obtained: taper

TREATMENT • INTRALESIONAL CORTICOSTEROID INJECTION - Triamcinolone - 1 -2 mg/kg - Bleeding, skin atrophy, skin necrosis, infection, anaphylaxis, adrenal suppression

TREATMENT • VINCRISTINE - Vinca alkaloid microtubule inhibitor - 1. 0 to 1. 5 mg/m 2 weekly - Immunosuppression, neuropathy, alopecia
, neurotoxicity")
TREATMENT • INTERFERON - antiangiogenic properties - effective - Spatstic diplegia (20%), neurotoxicity
,")
TREATMENT • PULSED DYE LASER - Very superficial lesions - Small (<4 -5 cm), ulcerated hemangioma * - Ulceration, scarring

TREATMENT • TOPICAL THERAPY - Timolol 0. 5% gel - Superficial IH • No large clinical trials

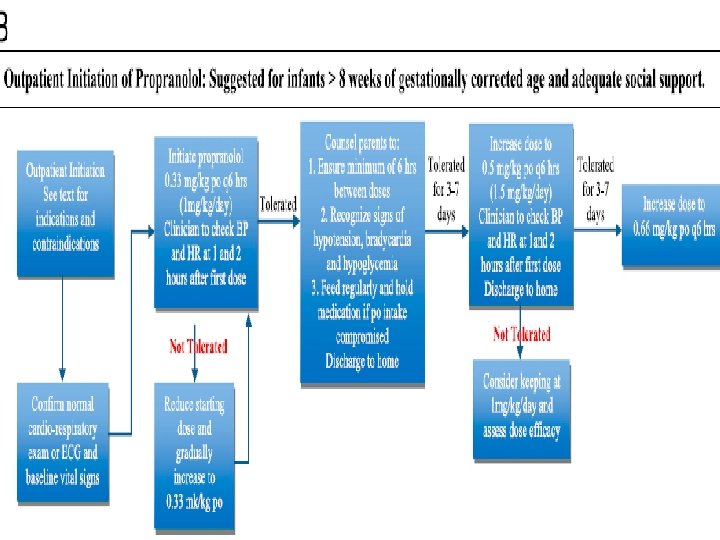
TREATMENT • PROPRANOLOL • Complications - 2 mg/kg/day * - Bradycardia, Hypotension, - Excellent results Hypoglycemia - “exact indications, dosage, length of treatment, and long-term sequelae have not been thoroughly investigated”

• After propranolol, ano nangyari? If u plan to do the time line as seen earlier sa HPI, you can show it again here to emphasize if size has decreased. .

TREATMENT • SURGICAL - Pedunculated or exophytic hemangiomas in which scarring is highly probable - Chronically ulcerated hemangiomas causing pain - Will lead to disfigurement, bleeding

RECOMMENDATIONS • Facial hemangioma >/= 5 cm • Evaluate for PHACE • >/= 5 cutaneous lesions • Hepatic ultrasound

You may want to add: • Ano nangyari after propranolol? nagtachy ba cya? Lumiit ba yung mass? • When do we rrefer hemangiomas to a hematologist? • When does it become alarming? VS saying to Mom na “observe” lng?

• Pls do not forget to remind your moderator/reactor • Be early tom kasi may flagcem. . We cant help u na if mag 8 am na. . • Good Luck!

THANK YOU
86abef49ce6b35e11ff48021c65a3c19.ppt