c404bc54c2296f802ccc0c68aad593cd.ppt
- Количество слайдов: 26
 Case 1 – My Organs are rotting
Case 1 – My Organs are rotting
 PC -Maria, 20 yo female - Presents with low mood HPC -Low mood for past 3 weeks - no energy, profound and pervasive anhedonia - slow thinking - missed appointment with customers received warning at work - overwhelming sense that something bad is about to happen but can’t identify - lost 4 kg unintentionally -Lying awake at night thinking how pointless her life is -Has suicidal ideation but no plan (thought would hurt her family too much) -Feels dead inside, but not actually believe this
PC -Maria, 20 yo female - Presents with low mood HPC -Low mood for past 3 weeks - no energy, profound and pervasive anhedonia - slow thinking - missed appointment with customers received warning at work - overwhelming sense that something bad is about to happen but can’t identify - lost 4 kg unintentionally -Lying awake at night thinking how pointless her life is -Has suicidal ideation but no plan (thought would hurt her family too much) -Feels dead inside, but not actually believe this
 Past Medical Hx & Surgical Hx -Nil sometimes presented with multiple physical complaints but always been fit and healthy -Past Psychiatric Hx -Anxiety & difficulties coping with work and relationships -Alcohol abuse in the past - Eating disorder (binging and purging) -Received in the past supportive counselling due to childhood sexual abuse Medication Nil Allergies Nil
Past Medical Hx & Surgical Hx -Nil sometimes presented with multiple physical complaints but always been fit and healthy -Past Psychiatric Hx -Anxiety & difficulties coping with work and relationships -Alcohol abuse in the past - Eating disorder (binging and purging) -Received in the past supportive counselling due to childhood sexual abuse Medication Nil Allergies Nil
 Substance Abuse -Et. OH abuse in the past - Smoking? -Illicit drugs? Personal and social Hx -Occ: Sales rep - Living at home with parents -Abused sexually when 12 yrs old at her friend’s house during sleep over Family Hx of Med and Psych Nil
Substance Abuse -Et. OH abuse in the past - Smoking? -Illicit drugs? Personal and social Hx -Occ: Sales rep - Living at home with parents -Abused sexually when 12 yrs old at her friend’s house during sleep over Family Hx of Med and Psych Nil
 Questions: Q 1. What is your provisional diagnosis and differential diagnosis? Justify the reasons for your answer. Q 2. What further information would you seek to clarify your diagnosis and management - justify each of your answers? Q 3. What physical investigations would you request - justify each of your answers? Q 4. Would you raise the issue of Maria's childhood trauma at this point in the consultation? Why or why not?
Questions: Q 1. What is your provisional diagnosis and differential diagnosis? Justify the reasons for your answer. Q 2. What further information would you seek to clarify your diagnosis and management - justify each of your answers? Q 3. What physical investigations would you request - justify each of your answers? Q 4. Would you raise the issue of Maria's childhood trauma at this point in the consultation? Why or why not?
 Trigger 2: -Dx with Major Depression treated with Fluvoxamine 100 mg and to return in 3 days - When returned: MSE – ASEPTIC Appearance Exhausted Speech Slow Emotion (Mood & affect) Low feels better dead Perception Nil hallucination and illusion Thought content & process ? Is spacing out a form of thought disorder? ? Insight & Judgement Won’t kill herself but can’t articulate why Cognition
Trigger 2: -Dx with Major Depression treated with Fluvoxamine 100 mg and to return in 3 days - When returned: MSE – ASEPTIC Appearance Exhausted Speech Slow Emotion (Mood & affect) Low feels better dead Perception Nil hallucination and illusion Thought content & process ? Is spacing out a form of thought disorder? ? Insight & Judgement Won’t kill herself but can’t articulate why Cognition
 Trigger 2. . . : Other -Not eating anything - Refusing to go to hospital but agree to see private psychiatrist Questions Q 5. What treatment options are available at this time? Q 6. Give the reasons for and against the use of involuntary treatment for hospitalisation? Q 7. What things might you do to reduce the risk of harm befalling Maria?
Trigger 2. . . : Other -Not eating anything - Refusing to go to hospital but agree to see private psychiatrist Questions Q 5. What treatment options are available at this time? Q 6. Give the reasons for and against the use of involuntary treatment for hospitalisation? Q 7. What things might you do to reduce the risk of harm befalling Maria?
 Trigger 2. . . : Maria returned the next day Appearance & Behaviour Nil eye contact Speech Emotion Perception -Complains of repugnant smell coming from her body and believes her organs are rotting Thought -believes she is already dead -Believes world would be better without her as she is so evil Insight & Judgment Cognition Other Family Hx: Mother actually had these episodes many yrs ago ECT Not eating and drinking mildly dehydrated
Trigger 2. . . : Maria returned the next day Appearance & Behaviour Nil eye contact Speech Emotion Perception -Complains of repugnant smell coming from her body and believes her organs are rotting Thought -believes she is already dead -Believes world would be better without her as she is so evil Insight & Judgment Cognition Other Family Hx: Mother actually had these episodes many yrs ago ECT Not eating and drinking mildly dehydrated
 Q 8. What is the likely diagnosis and what symptoms have made this diagnosis more probable? Q 9. How are you going to manage this situation in your general practice?
Q 8. What is the likely diagnosis and what symptoms have made this diagnosis more probable? Q 9. How are you going to manage this situation in your general practice?
 Trigger 3 -BIBA to hospital -Continues to express that she is dead and rotting inside -Refuses to eat, drink, wash or bathe -Treated as involuntary pt under MHA -Plan: ECT father angry as mother was never the same after receiving ECT and mother had bruising from being held Q 10. What information can you provide to the father about ECT? Q 11. How has the treatment changed from 40 years ago?
Trigger 3 -BIBA to hospital -Continues to express that she is dead and rotting inside -Refuses to eat, drink, wash or bathe -Treated as involuntary pt under MHA -Plan: ECT father angry as mother was never the same after receiving ECT and mother had bruising from being held Q 10. What information can you provide to the father about ECT? Q 11. How has the treatment changed from 40 years ago?
 Trigger 3. . . -Returned 1 month later to see you -Dx with MDD with Psychotic Features -Medication: Venlafaxine XR 225 mg Mane and Risperidone 2 mg Nocte -Euthymic & little recollection of events prior to hospitalisation Q 12. What advice will you give Maria regarding side effects of the antidepressant and the atypical antipsychotics such as risperidone? Q 13. What physical examination and investigations will you do at base line and follow up for a patient on atypical antipsychotics? Q 14. How long will Maria need to stay on these medications? Q 15. During one of her appointments, Maria asks if the abuse she experienced in childhood is the cause of her psychotic depression? What is the association between the childhood trauma that Maria experienced and her psychotic depression?
Trigger 3. . . -Returned 1 month later to see you -Dx with MDD with Psychotic Features -Medication: Venlafaxine XR 225 mg Mane and Risperidone 2 mg Nocte -Euthymic & little recollection of events prior to hospitalisation Q 12. What advice will you give Maria regarding side effects of the antidepressant and the atypical antipsychotics such as risperidone? Q 13. What physical examination and investigations will you do at base line and follow up for a patient on atypical antipsychotics? Q 14. How long will Maria need to stay on these medications? Q 15. During one of her appointments, Maria asks if the abuse she experienced in childhood is the cause of her psychotic depression? What is the association between the childhood trauma that Maria experienced and her psychotic depression?
 Question 4 Would you raise the issue of Maria's childhood trauma at this point in the consultation? Why or why not?
Question 4 Would you raise the issue of Maria's childhood trauma at this point in the consultation? Why or why not?
 Question 4 There’s conflicting advice amongst the literature as to when it’s best to address the issue of sexual assault. Whilst some say that it is necessary to address the issue of sexual assault regardless of whether it’s the underlying cause of emotional distress, others suggest a more tactful approach – addressing the issue initially only if it is the underlying cause of the emotional distress but the practitioner may wish to address the issue at a later time point once the patient is less distressed. Personally, I feel that the second approach would possibly be better in this scenario. l However, if Maria brought up the issue, then I think it should be addressed l Alternatively, however, it’s perhaps possible to address the issue with Maria by asking whether she’s still partaking in supportive counselling of any form.
Question 4 There’s conflicting advice amongst the literature as to when it’s best to address the issue of sexual assault. Whilst some say that it is necessary to address the issue of sexual assault regardless of whether it’s the underlying cause of emotional distress, others suggest a more tactful approach – addressing the issue initially only if it is the underlying cause of the emotional distress but the practitioner may wish to address the issue at a later time point once the patient is less distressed. Personally, I feel that the second approach would possibly be better in this scenario. l However, if Maria brought up the issue, then I think it should be addressed l Alternatively, however, it’s perhaps possible to address the issue with Maria by asking whether she’s still partaking in supportive counselling of any form.
 Question 5 What treatment options are available at this time?
Question 5 What treatment options are available at this time?
 Question 5 Antidepressants are more effective for moderate to severe depression, although concurrent psychological therapies may often be helpful. About 50% of patients with major depression respond to treatment with an initial antidepressant. Pharmacological treatment: Evidence-based medicine reviews indicate that all antidepressants are of similar efficacy in the treatment of major depression. l Individual drugs differ in their adverse effect profiles, their potential for drug interactions and their safety. l E. g. sertraline (initial dose: 25 -50 mg/day; maintenance: 50 -100 mg/day) Non-pharmacological treatment l CBT Behavioural therapy (including graded task assignment) Homework Cognitive therapy/cognitive restructuring Skill building IPT l ECT
Question 5 Antidepressants are more effective for moderate to severe depression, although concurrent psychological therapies may often be helpful. About 50% of patients with major depression respond to treatment with an initial antidepressant. Pharmacological treatment: Evidence-based medicine reviews indicate that all antidepressants are of similar efficacy in the treatment of major depression. l Individual drugs differ in their adverse effect profiles, their potential for drug interactions and their safety. l E. g. sertraline (initial dose: 25 -50 mg/day; maintenance: 50 -100 mg/day) Non-pharmacological treatment l CBT Behavioural therapy (including graded task assignment) Homework Cognitive therapy/cognitive restructuring Skill building IPT l ECT
 Question 6 Give the reasons for and against the use of involuntary treatment for hospitalisation?
Question 6 Give the reasons for and against the use of involuntary treatment for hospitalisation?
 Question 6 FOR: A lack of insight into their conditions may act as a barrier to necessary treatment A majority of persons suffering from severe mental illness show limited insight into their illness. Schizophrenic patients, in particular, may show no recognition that they have a mental illness or need treatment. Depressed patients who are unable to envision hope or recall a better time may be suicidal and unwilling to seek treatment. Manic individuals who have become markedly grandiose and deny that they have any kind of problem or illness that needs treatment may display behaviors that put themselves or others in danger. Other patients may recognize their symptoms as part of an illness, but disagree with and refuse recommended treatment. Untreated depression, mania, and psychosis can have devastating effects on both the affected individual and those around him or her: suicide, assaults on others, inadvertent tragedies stemming from delusional thinking, financial and social ruin, and inability to adequately care for one’s own needs. AGAINST: There is controversy surrounding involuntary treatment of mental health patients as many critics argue that it violates basic human liberty. Critics argue that patients with cancer are not forced to have chemotherapy and thus, this should also apply to mental health disorders Self-harm does not justify interference with an individual’s right of autonomy (Donnelly, M From autonomy to dignity: treatment for mental health disorders and the focus for patient rights)
Question 6 FOR: A lack of insight into their conditions may act as a barrier to necessary treatment A majority of persons suffering from severe mental illness show limited insight into their illness. Schizophrenic patients, in particular, may show no recognition that they have a mental illness or need treatment. Depressed patients who are unable to envision hope or recall a better time may be suicidal and unwilling to seek treatment. Manic individuals who have become markedly grandiose and deny that they have any kind of problem or illness that needs treatment may display behaviors that put themselves or others in danger. Other patients may recognize their symptoms as part of an illness, but disagree with and refuse recommended treatment. Untreated depression, mania, and psychosis can have devastating effects on both the affected individual and those around him or her: suicide, assaults on others, inadvertent tragedies stemming from delusional thinking, financial and social ruin, and inability to adequately care for one’s own needs. AGAINST: There is controversy surrounding involuntary treatment of mental health patients as many critics argue that it violates basic human liberty. Critics argue that patients with cancer are not forced to have chemotherapy and thus, this should also apply to mental health disorders Self-harm does not justify interference with an individual’s right of autonomy (Donnelly, M From autonomy to dignity: treatment for mental health disorders and the focus for patient rights)
 Question 13 What physical examination and investigations will you do at base line and follow up for a patient on atypical antipsychotics?
Question 13 What physical examination and investigations will you do at base line and follow up for a patient on atypical antipsychotics?
 Question 13 Atypical antipsychotic: Clozapine, Risperidone, Olanzapine, Quetiapine, Ziprasidone, Aripiprazole Shared side Effects 1. Neurological Acute EPS: pseudoparkinonism, dystonia, akathisia, akinesia Chronic EPS: Tardive dyskinesia, tardive dystonia, neuroleptic malignant syndrome (Tetrad of: fever, rigidity, mental status change, autonomic instability) 2. Sedation 3. Cardiovascular Postural hypotension Tachycardia QT prolongation 4. Anticholinergic and antriadrenergic effects Dry mouth, blurred vision, constipation, tachycardia, urinary retention, thermoregulatory effects Central anticholinergic: confusion, delirium, somnolence, hallucinations
Question 13 Atypical antipsychotic: Clozapine, Risperidone, Olanzapine, Quetiapine, Ziprasidone, Aripiprazole Shared side Effects 1. Neurological Acute EPS: pseudoparkinonism, dystonia, akathisia, akinesia Chronic EPS: Tardive dyskinesia, tardive dystonia, neuroleptic malignant syndrome (Tetrad of: fever, rigidity, mental status change, autonomic instability) 2. Sedation 3. Cardiovascular Postural hypotension Tachycardia QT prolongation 4. Anticholinergic and antriadrenergic effects Dry mouth, blurred vision, constipation, tachycardia, urinary retention, thermoregulatory effects Central anticholinergic: confusion, delirium, somnolence, hallucinations
 Question 13 5. Weight gain and metabolic abnormalities Metabolic abnormalities: diabetes and hyperlipidemia 6. Disturbance in sexual function and Hyperprolactinemia Breast tenderness, breast enlargement, lactation, decreased gonadal hormones (incl. Estrogen and Testosterone), eliminate menstrual cycles, reduced sexual interest and function Specific Side Effects Clozapine: agranulocytosis, sialorrhea, drooling, myocarditis, seizures, rare: pancreatitis, DVT, PE, hepatitis, eosinophilia, weight gain Risperidone: small increase in risk of stroke in pt with dementia Olanzapine: nil specific Quetiapine: increased risk of cataracts in beagles (not proven in human) Ziprasidone: Insomnia Aripiprazole: Insomnia
Question 13 5. Weight gain and metabolic abnormalities Metabolic abnormalities: diabetes and hyperlipidemia 6. Disturbance in sexual function and Hyperprolactinemia Breast tenderness, breast enlargement, lactation, decreased gonadal hormones (incl. Estrogen and Testosterone), eliminate menstrual cycles, reduced sexual interest and function Specific Side Effects Clozapine: agranulocytosis, sialorrhea, drooling, myocarditis, seizures, rare: pancreatitis, DVT, PE, hepatitis, eosinophilia, weight gain Risperidone: small increase in risk of stroke in pt with dementia Olanzapine: nil specific Quetiapine: increased risk of cataracts in beagles (not proven in human) Ziprasidone: Insomnia Aripiprazole: Insomnia
 Question 13 Monitoring For all: Do initial exam and monitor for shared side effects: Cardiovascular health (Pulse, BP, ECG, electrolytes), Extrapyramidal side effects, sedation, weight gain, hyperlipidemia, diabetes, hyperprolactinemia (prolactin level) Then monitor specific, eg: Clozapine: monitor WBC and neutrophils Quetiapine: Ophtalmology exam is recommended
Question 13 Monitoring For all: Do initial exam and monitor for shared side effects: Cardiovascular health (Pulse, BP, ECG, electrolytes), Extrapyramidal side effects, sedation, weight gain, hyperlipidemia, diabetes, hyperprolactinemia (prolactin level) Then monitor specific, eg: Clozapine: monitor WBC and neutrophils Quetiapine: Ophtalmology exam is recommended
 Question 14 Q 14. How long will Maria need to stay on these medications? From uptodate: Duration of treatment depends on diagnosis. Pt with delirium, agitation, brief psychotic disorders, or impulsivity may require only a few days or weeks of treatment. Schizophrenic patients, in contrast, benefit from continuous treatment and are at risk for relapse with medication discontinuation or even dose reduction
Question 14 Q 14. How long will Maria need to stay on these medications? From uptodate: Duration of treatment depends on diagnosis. Pt with delirium, agitation, brief psychotic disorders, or impulsivity may require only a few days or weeks of treatment. Schizophrenic patients, in contrast, benefit from continuous treatment and are at risk for relapse with medication discontinuation or even dose reduction
 Question 15 During one of her appointments, Maria asks if the abuse she experienced in childhood is the cause of her psychotic depression? What is the association between the childhood trauma that Maria experienced and her psychotic depression? From Uptodate Short term sequelae (2 yrs of assault) of sexual abuse in childhood: fear, disturbances in sleep and eeating, phobias, guilt, shame, anger, depression, school problems, delinquency, aggression, hostility, antisocial behaviour, inappropriate sexual behaviour, and running away Longer term: depression, sleep problems, eating disorders, obesity, feelings of isolation, stigmatization, poor self-esteem, problems with interpersonal relationships, negative effect on sexual function, revictimization, substance abuse, suicidal behavior, and psychosis Depends on: Severity of the assault eg: penetration, duration, frequency, force, relationship to abuser, maternal support Protective factors: family, teacher caring, other adult caring, school safety
Question 15 During one of her appointments, Maria asks if the abuse she experienced in childhood is the cause of her psychotic depression? What is the association between the childhood trauma that Maria experienced and her psychotic depression? From Uptodate Short term sequelae (2 yrs of assault) of sexual abuse in childhood: fear, disturbances in sleep and eeating, phobias, guilt, shame, anger, depression, school problems, delinquency, aggression, hostility, antisocial behaviour, inappropriate sexual behaviour, and running away Longer term: depression, sleep problems, eating disorders, obesity, feelings of isolation, stigmatization, poor self-esteem, problems with interpersonal relationships, negative effect on sexual function, revictimization, substance abuse, suicidal behavior, and psychosis Depends on: Severity of the assault eg: penetration, duration, frequency, force, relationship to abuser, maternal support Protective factors: family, teacher caring, other adult caring, school safety
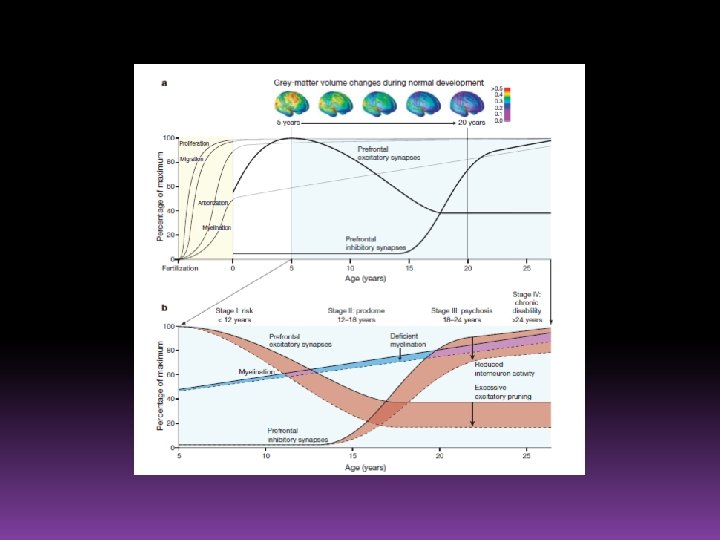
 • During childhood and teen brain brings") Just for Interest (from Additional resources Blackboard) • During childhood and teen brain brings major upgrades to neural networks that generate powers of judgement, cognition, and behavioural control • The idea is: schizophrenia arises from miscues or shoddy work in this complicated and delicate time • Particular area of interest: DLPFC (Dorsolateral prefrontal cortex) important to tying threads of experience, memory, thought and emotion into coherent, consistent view of the world. • DLPFC builds its circuitry during childhood and adolescence, responding to both genes and experience
Just for Interest (from Additional resources Blackboard) • During childhood and teen brain brings major upgrades to neural networks that generate powers of judgement, cognition, and behavioural control • The idea is: schizophrenia arises from miscues or shoddy work in this complicated and delicate time • Particular area of interest: DLPFC (Dorsolateral prefrontal cortex) important to tying threads of experience, memory, thought and emotion into coherent, consistent view of the world. • DLPFC builds its circuitry during childhood and adolescence, responding to both genes and experience
 Just for Interest: It has mainly 2 types of cells 1. Pyramidal neurons spans several layers of cortex • Generate complex electrical signallying in DLPFC and in prefrontal cortex as a whole • Adult with schizo smaller cell bodies and fewer of dendritic spines that receive input of synapses • Thought due to abnormal synaptic pruning during adolescence (Pruning is thought to eliminate weak synapses and leave strong ones). In schizo thought that pruning ‘indiscriminately’ • In monkey brain however, found that pyramidal neurons functionally mature before pruning started. Alternative hypothesis that schizophrenic had weaker synapses before pruning ever began 2. Chandelier cells sit near the base of pyramidal cells • Only connected to pyramical cells • Take huge hits in schizo proteins reduced by 40% • Thought that schizophrenic chandelier cells fail at its task of cultivating pyramidal cells during childhood or early adolescence • Failure of chandelier & pyramidal do not generate enough neural traffic required prefrontal cortex incapable of creating vigorous & coordinated firing (‘gamma synchrony’) that generates working memory shattered mind of schizophrenia
Just for Interest: It has mainly 2 types of cells 1. Pyramidal neurons spans several layers of cortex • Generate complex electrical signallying in DLPFC and in prefrontal cortex as a whole • Adult with schizo smaller cell bodies and fewer of dendritic spines that receive input of synapses • Thought due to abnormal synaptic pruning during adolescence (Pruning is thought to eliminate weak synapses and leave strong ones). In schizo thought that pruning ‘indiscriminately’ • In monkey brain however, found that pyramidal neurons functionally mature before pruning started. Alternative hypothesis that schizophrenic had weaker synapses before pruning ever began 2. Chandelier cells sit near the base of pyramidal cells • Only connected to pyramical cells • Take huge hits in schizo proteins reduced by 40% • Thought that schizophrenic chandelier cells fail at its task of cultivating pyramidal cells during childhood or early adolescence • Failure of chandelier & pyramidal do not generate enough neural traffic required prefrontal cortex incapable of creating vigorous & coordinated firing (‘gamma synchrony’) that generates working memory shattered mind of schizophrenia