

3ebd8de6350563a6c1b5db195230921c.ppt
- Количество слайдов: 8
 Case 1 • 49 yo male with hypertension on a potassium-sparing diuretic
Case 1 • 49 yo male with hypertension on a potassium-sparing diuretic
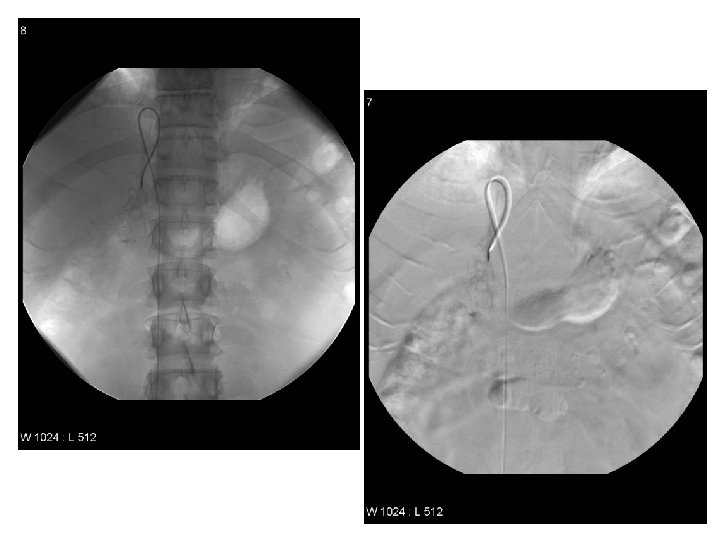
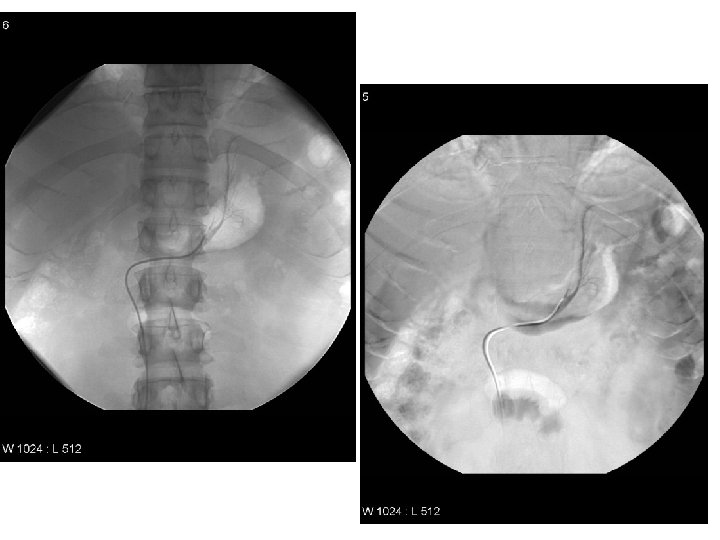
 Findings • Access from right iliac vein • Selection of left and right adrenal veins • Gentle venography to confirm location at adrenal veins; formal venography unnecessary • Subsequent bilateral adrenal vein and IVC sampling • CT useful in planning by demonstrating the anatomy and position of the adrenal veins.
Findings • Access from right iliac vein • Selection of left and right adrenal veins • Gentle venography to confirm location at adrenal veins; formal venography unnecessary • Subsequent bilateral adrenal vein and IVC sampling • CT useful in planning by demonstrating the anatomy and position of the adrenal veins.
 Why do Adrenal vein sampling? ? ? • Done to assess whether autonomous hormone production is uni or bilateral in known endocrine disease. • Adrenal lesions rarely require catheter-based imaging for diagnosis; typically done with CT and MRI • Most commonly performed in primary aldosteronism, which is the most common hypersecretory adrenal disease. • Less commonly, in proven pheo, when no source is visible on CT or other imaging. • Rarely performed in adrenal Cushing disease or syndromes of androgen excess
Why do Adrenal vein sampling? ? ? • Done to assess whether autonomous hormone production is uni or bilateral in known endocrine disease. • Adrenal lesions rarely require catheter-based imaging for diagnosis; typically done with CT and MRI • Most commonly performed in primary aldosteronism, which is the most common hypersecretory adrenal disease. • Less commonly, in proven pheo, when no source is visible on CT or other imaging. • Rarely performed in adrenal Cushing disease or syndromes of androgen excess
 Aldosteronism • Secreted by the adrenal cortex that induces Na retention and K excretion. • A patient with diastolic HTN and K < 3. 5 m. Eq/L is suggestive of Conn’s. May also check plasma renin, 24 hr urine • In primary dz – hypersecretion by either an adenoma (2/3) or bilateral hyperplasia (1/3). <1% of cases due to carcinoma. • Secondary dz – response to renal artery stenosis, CHF, pregnancy or cirrhosis. • Initial imaging is with CT or MRI with angiography after definitive dx is made
Aldosteronism • Secreted by the adrenal cortex that induces Na retention and K excretion. • A patient with diastolic HTN and K < 3. 5 m. Eq/L is suggestive of Conn’s. May also check plasma renin, 24 hr urine • In primary dz – hypersecretion by either an adenoma (2/3) or bilateral hyperplasia (1/3). <1% of cases due to carcinoma. • Secondary dz – response to renal artery stenosis, CHF, pregnancy or cirrhosis. • Initial imaging is with CT or MRI with angiography after definitive dx is made
 Adrenal sampling Discussion • Samples may be obtained before and after ACTH adm. Eval for aldosterone and cortisol, with assumption that cortisol is the same for both glands. • Cortisol used to confirm adrenal vein is sampled and to help distinguish adenoma from hyperplasia. • Adenomas: ratio of aldosterone/cortisol is higher before and after ACTH (>4), whereas the ratio in the opposite gland is similar to the femoral vein. • Tx for unilateral adenoma is surgical resection. Bilateral hyperplasia is managed medically as resection would result in insufficiency.
Adrenal sampling Discussion • Samples may be obtained before and after ACTH adm. Eval for aldosterone and cortisol, with assumption that cortisol is the same for both glands. • Cortisol used to confirm adrenal vein is sampled and to help distinguish adenoma from hyperplasia. • Adenomas: ratio of aldosterone/cortisol is higher before and after ACTH (>4), whereas the ratio in the opposite gland is similar to the femoral vein. • Tx for unilateral adenoma is surgical resection. Bilateral hyperplasia is managed medically as resection would result in insufficiency.
 Thoughts and limitations • Previously thought if aldosteronism was diagnosed an adenoma was seen on CT then sampling was unnecessary – wrong! – Sampling v CT showed CT to be inaccurate or noncontributory in 68% for lesions <1 cm. • CT value is twofold: – Allows assessment of mass lesions – Demonstrates the anatomy/position of adrenal veins • Sampling limitations – Quiescent phase of aldosterone production – Venous drainage in vein other than one cannulated – Superselective sampling does not house an adenoma
Thoughts and limitations • Previously thought if aldosteronism was diagnosed an adenoma was seen on CT then sampling was unnecessary – wrong! – Sampling v CT showed CT to be inaccurate or noncontributory in 68% for lesions <1 cm. • CT value is twofold: – Allows assessment of mass lesions – Demonstrates the anatomy/position of adrenal veins • Sampling limitations – Quiescent phase of aldosterone production – Venous drainage in vein other than one cannulated – Superselective sampling does not house an adenoma