

5ec2a3d6c5db66c074a59d2d872f50df.ppt
- Количество слайдов: 34
 Carcinoma of the larynx • Epidemiology • Accounts for 1% of all new cancers diagnosed in the U. S. and 0. 75% of all cancer deaths. • Accounts for 30% in all head and neck cancers. • More frequently happened in patients at 50~70 years of age. • M: F ratio: 5~10: 1 (foreign country), 6. 75: 1(shanghai).
Carcinoma of the larynx • Epidemiology • Accounts for 1% of all new cancers diagnosed in the U. S. and 0. 75% of all cancer deaths. • Accounts for 30% in all head and neck cancers. • More frequently happened in patients at 50~70 years of age. • M: F ratio: 5~10: 1 (foreign country), 6. 75: 1(shanghai).
 Carcinoma of the larynx • Etiology • Cigarette • Wine (combined smoking and alcohol abuse increases the risk by 50% over the additive rate ) • air pollution • Virus (HPV) • precancerous lesions (Leukoplakia, Papilloma) • sex hormones
Carcinoma of the larynx • Etiology • Cigarette • Wine (combined smoking and alcohol abuse increases the risk by 50% over the additive rate ) • air pollution • Virus (HPV) • precancerous lesions (Leukoplakia, Papilloma) • sex hormones
 Leukoplakia of the larynx
Leukoplakia of the larynx
 Carcinoma of the larynx • Pathology • Nearly 98% are squamous cell carcinoma. • adenocarcinoma and undifferentiated carcinoma is rare.
Carcinoma of the larynx • Pathology • Nearly 98% are squamous cell carcinoma. • adenocarcinoma and undifferentiated carcinoma is rare.
:well differentiated, late metastasis •") Carcinoma of the larynx • Clinical classification: • Glottic (60%):well differentiated, late metastasis • Supraglottic (30%):poor differntiated, early metastasis • Subglottic (6%):poor differentiated, early metastasis
Carcinoma of the larynx • Clinical classification: • Glottic (60%):well differentiated, late metastasis • Supraglottic (30%):poor differntiated, early metastasis • Subglottic (6%):poor differentiated, early metastasis
 Anatomic divisions of the larynx
Anatomic divisions of the larynx
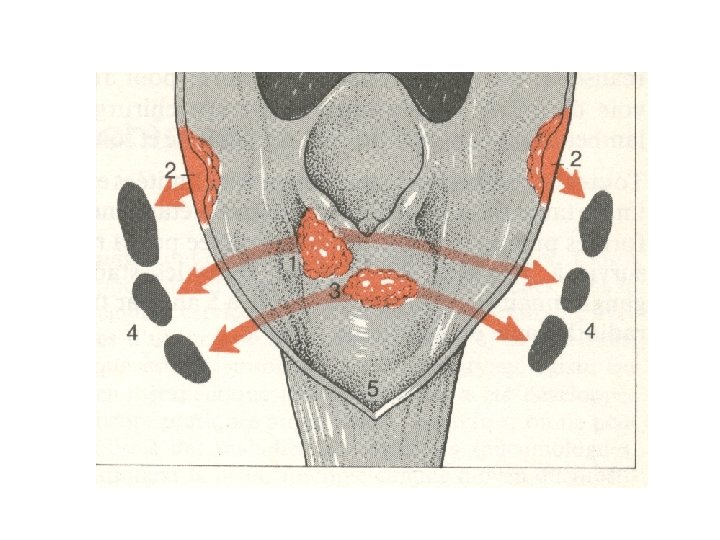
 Carcinoma of the larynx • Spread of tumor Direct spread Supraglottic cancer→ epiglottis, pre-epiglottic space, vallecula, and tongue base. piriform sinus, lateral wall of hypopharynx. paraglottic space, ventricle or the VC.
Carcinoma of the larynx • Spread of tumor Direct spread Supraglottic cancer→ epiglottis, pre-epiglottic space, vallecula, and tongue base. piriform sinus, lateral wall of hypopharynx. paraglottic space, ventricle or the VC.
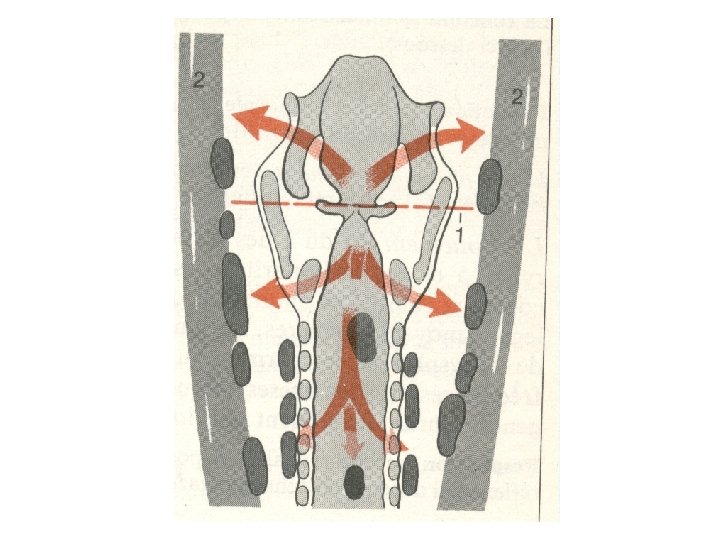
 Carcinoma of the larynx • Spread of tumor Direct spread Glottic cancer→ anteriorly, contralateral VC. posteriorly, arytenoid cartilage superiorly, supraglottic area. inferiorly, paraglottic space and subglottic area.
Carcinoma of the larynx • Spread of tumor Direct spread Glottic cancer→ anteriorly, contralateral VC. posteriorly, arytenoid cartilage superiorly, supraglottic area. inferiorly, paraglottic space and subglottic area.
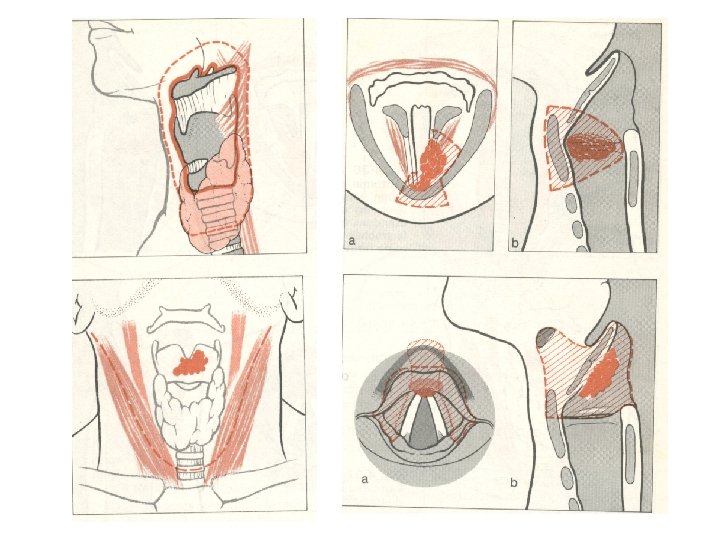
 Carcinoma of the larynx • Spread of tumor Direct spread Subglottic cancer→superiorly, glottis. anteriorly and laterally, strap muscle and thyroid gland. posteriorly, esophagus.
Carcinoma of the larynx • Spread of tumor Direct spread Subglottic cancer→superiorly, glottis. anteriorly and laterally, strap muscle and thyroid gland. posteriorly, esophagus.
 Carcinoma of the larynx • Spread of tumor Lymph nodes metastases • Supraglottic cancer →have a propensity to spread to cervical lymph nodes bilaterally at the early stages. • Generally, the risk of occult or actual metastases from T 1, T 2, T 3 and T 4 tumors is 20, 40, 60, and 80%.
Carcinoma of the larynx • Spread of tumor Lymph nodes metastases • Supraglottic cancer →have a propensity to spread to cervical lymph nodes bilaterally at the early stages. • Generally, the risk of occult or actual metastases from T 1, T 2, T 3 and T 4 tumors is 20, 40, 60, and 80%.
 Carcinoma of the larynx • Spread of tumor Lymph nodes metastases Glottic cancer →CV is virtually devoid of lymphatics, involvement of cervical nodes at the early stages is not common. < 8% of patients with T 1 and T 2 tumors will have nodal involvement.
Carcinoma of the larynx • Spread of tumor Lymph nodes metastases Glottic cancer →CV is virtually devoid of lymphatics, involvement of cervical nodes at the early stages is not common. < 8% of patients with T 1 and T 2 tumors will have nodal involvement.
 Carcinoma of the larynx • Spread of tumor Lymph nodes metastases Glottic cancer →Only at the later stages, prelaryngeal nodes, paratracheal nodes and other cervical nodes could be involved.
Carcinoma of the larynx • Spread of tumor Lymph nodes metastases Glottic cancer →Only at the later stages, prelaryngeal nodes, paratracheal nodes and other cervical nodes could be involved.
 Carcinoma of the larynx • Spread of tumor Lymph nodes metastases Subglottic cancer →tend to spread to paratracheal lymphatics and then to superior mediastinual nodes.
Carcinoma of the larynx • Spread of tumor Lymph nodes metastases Subglottic cancer →tend to spread to paratracheal lymphatics and then to superior mediastinual nodes.
 Carcinoma of the larynx • Spread of tumor Distant metstases via blood Distant metastasis only occurs in the very later stage of laryngeal carcinoma.
Carcinoma of the larynx • Spread of tumor Distant metstases via blood Distant metastasis only occurs in the very later stage of laryngeal carcinoma.
 Carcinoma of the larynx • Clinical manifestations • Supraglottic carcinoma: • Might be asymptomatic • Foreign body sensation • Pain while swallowing • Throat burns • Enlargement of cervical lymph nodes
Carcinoma of the larynx • Clinical manifestations • Supraglottic carcinoma: • Might be asymptomatic • Foreign body sensation • Pain while swallowing • Throat burns • Enlargement of cervical lymph nodes
 Carcinoma of the larynx • Clinical manifestations • Glottic carcinoma: • Hoarsenenss is the early symptom • Respiratory obstruction will happen in late stage
Carcinoma of the larynx • Clinical manifestations • Glottic carcinoma: • Hoarsenenss is the early symptom • Respiratory obstruction will happen in late stage
 Carcinoma of the larynx • Clinical manifestations • Subglottic carcinoma: • There are no definitive symptoms in the early stage. • Dyspnea and lymph nodes metastasis is the late symptoms
Carcinoma of the larynx • Clinical manifestations • Subglottic carcinoma: • There are no definitive symptoms in the early stage. • Dyspnea and lymph nodes metastasis is the late symptoms
 Supraglottic carcinoma
Supraglottic carcinoma
 Glottic carcinoma
Glottic carcinoma
 Carcinoma of the larynx • Physical examination • Laryngoscopic examination can find a mass on one or both vocal cords • fixation of the vocal cords is common • mass in the neck
Carcinoma of the larynx • Physical examination • Laryngoscopic examination can find a mass on one or both vocal cords • fixation of the vocal cords is common • mass in the neck
 Carcinoma of the larynx
Carcinoma of the larynx
 Carcinoma of the larynx • Differential diagnosis • Tuberculosis of the larynx :chest X-ray film • Papilloma of the larynx • Syphilis of the larynx
Carcinoma of the larynx • Differential diagnosis • Tuberculosis of the larynx :chest X-ray film • Papilloma of the larynx • Syphilis of the larynx
 Treatment • The modality of treatment depends on: • the exact site of the lesion • early or advanced stage • presence or absence of neck metastasis • distant metastasis • age and sometimes the patient’s wish
Treatment • The modality of treatment depends on: • the exact site of the lesion • early or advanced stage • presence or absence of neck metastasis • distant metastasis • age and sometimes the patient’s wish
 is usually managed with single modality") Treatment • Early laryngeal carcinoma (T 1/T 2) is usually managed with single modality of treatment and responds well to radiation, transoral laser resection, or partial laryngeal surgery. • Primary cure rates of 80 to 85% are expected.
Treatment • Early laryngeal carcinoma (T 1/T 2) is usually managed with single modality of treatment and responds well to radiation, transoral laser resection, or partial laryngeal surgery. • Primary cure rates of 80 to 85% are expected.
 Treatment • The management of advanced laryngeal carcinoma is more controversial. • The aim is to optimize disease-free and overall survival while preserving quality of life.
Treatment • The management of advanced laryngeal carcinoma is more controversial. • The aim is to optimize disease-free and overall survival while preserving quality of life.
 Treatment • Generally, combined therapy is widely used, as it shows better survival rates than singlemodality treatment. • Surgery + radiotherapy or radiotherapy + surgery are two commonly used modalities.
Treatment • Generally, combined therapy is widely used, as it shows better survival rates than singlemodality treatment. • Surgery + radiotherapy or radiotherapy + surgery are two commonly used modalities.
 Surgical treatment • Partial laryngectomy • Laryngofissure with cordectomy • Vertical partial laryngectomy • Frontolateral partial laryngectomy • Horizontal vertical partial laryngectomy • Supracricoid partial laryngectomy • Near total laryngectomy(Pearson’s operation) • Transoral laser resection
Surgical treatment • Partial laryngectomy • Laryngofissure with cordectomy • Vertical partial laryngectomy • Frontolateral partial laryngectomy • Horizontal vertical partial laryngectomy • Supracricoid partial laryngectomy • Near total laryngectomy(Pearson’s operation) • Transoral laser resection
 Surgical treatment • Total laryngectomy • Neck dissection • Radical neck dissection • Functional neck dissection • Selective neck dissection
Surgical treatment • Total laryngectomy • Neck dissection • Radical neck dissection • Functional neck dissection • Selective neck dissection
 Surgical treatment • Rehabilitation of speech after total laryngectomy • Blom- Singer valve • Esophageal speech • Electrical larynx
Surgical treatment • Rehabilitation of speech after total laryngectomy • Blom- Singer valve • Esophageal speech • Electrical larynx
 Radiotherapy • T 1 N 0 M 0 tumors located at the mid-portion of the VC • Contraindication for surgery because of poor general condition • Pre-operative irradiation for some advanced tumors
Radiotherapy • T 1 N 0 M 0 tumors located at the mid-portion of the VC • Contraindication for surgery because of poor general condition • Pre-operative irradiation for some advanced tumors
 Other treatment modality • Chemotherapy • Genetherapy
Other treatment modality • Chemotherapy • Genetherapy