

37ef4706a7fa2eac7e2dd3fe29cc24d3.ppt
- Количество слайдов: 46
 Cancer Registration and Cancer Control in Asia IACR Workshop: Beijing 16 th Sept. 2004
Cancer Registration and Cancer Control in Asia IACR Workshop: Beijing 16 th Sept. 2004
 THE POPULATION BASED CANCER REGISTRY IS THE INDISPENSIBLE FOUNDATION OF A SURVEILLANCE SYSTEM
THE POPULATION BASED CANCER REGISTRY IS THE INDISPENSIBLE FOUNDATION OF A SURVEILLANCE SYSTEM
 A cancer surveillance programme exists to: · To assess the current magnitude of the cancer burden and its likely future evolution · To provide a basis for research on cancer causes and prevention · To provide information on prevalence and trends in risk factors, · To monitor the effects of early detection, screening, treatment, and palliative care.
A cancer surveillance programme exists to: · To assess the current magnitude of the cancer burden and its likely future evolution · To provide a basis for research on cancer causes and prevention · To provide information on prevalence and trends in risk factors, · To monitor the effects of early detection, screening, treatment, and palliative care.
 PURPOSES AND USES OF CANCER REGISTRATION 1 Epidemiological Research Descriptive Epidemiology Analytic Epidemiology 2 Health Care Planning and Monitoring Patient Care Survival Screening Prevention
PURPOSES AND USES OF CANCER REGISTRATION 1 Epidemiological Research Descriptive Epidemiology Analytic Epidemiology 2 Health Care Planning and Monitoring Patient Care Survival Screening Prevention
 EPIDEMIOLOGY 1 Descriptive The information on exposure comes from routine sources (registers, records, surveys. . . ) The variables are non-specific (indirect link to ‘causes’) 2 Analytic Information on exposure is collected from individual subjects Association between “risk factors” [possible ‘causes’] and disease
EPIDEMIOLOGY 1 Descriptive The information on exposure comes from routine sources (registers, records, surveys. . . ) The variables are non-specific (indirect link to ‘causes’) 2 Analytic Information on exposure is collected from individual subjects Association between “risk factors” [possible ‘causes’] and disease
 Cervix Uteri, Incidence Rates by Education Level, Quito Residents. 1985 -1999 Rate per 100, 000 80. 0 In-situ Invasive 70. 0 60. 0 50. 0 40. 0 30. 0 20. 0 10. 0 None Primary Secondary Higher Education level Source N. T. R. Cancer in Ecuadorian regions 1997 -1999 NCR, Solca Quito, 2001
Cervix Uteri, Incidence Rates by Education Level, Quito Residents. 1985 -1999 Rate per 100, 000 80. 0 In-situ Invasive 70. 0 60. 0 50. 0 40. 0 30. 0 20. 0 10. 0 None Primary Secondary Higher Education level Source N. T. R. Cancer in Ecuadorian regions 1997 -1999 NCR, Solca Quito, 2001
 Cancer in Scotland 1975 -1980 Large Bowel, Females IARC Scientific Publications No. 72, 1985
Cancer in Scotland 1975 -1980 Large Bowel, Females IARC Scientific Publications No. 72, 1985
, MALES Singapore Chinese Hong") Trends in Colon Cancer Incidence: ASIA Age Standardised Rate (World), MALES Singapore Chinese Hong Kong Osaka Manila Bombay ………………… …. …………………. .
Trends in Colon Cancer Incidence: ASIA Age Standardised Rate (World), MALES Singapore Chinese Hong Kong Osaka Manila Bombay ………………… …. …………………. .
 PURPOSES AND USES OF CANCER REGISTRATION 1 Epidemiological Research Descriptive Epidemiology Analytic Epidemiology 2 Health Care Planning and Monitoring Patient Care Survival Screening Prevention
PURPOSES AND USES OF CANCER REGISTRATION 1 Epidemiological Research Descriptive Epidemiology Analytic Epidemiology 2 Health Care Planning and Monitoring Patient Care Survival Screening Prevention
 USES OF CANCER REGISTRY PLANNING & EVALUATION OF CCPs I DEFINING THE PROBLEM • Burden of cancer • Past trends • Future projections
USES OF CANCER REGISTRY PLANNING & EVALUATION OF CCPs I DEFINING THE PROBLEM • Burden of cancer • Past trends • Future projections
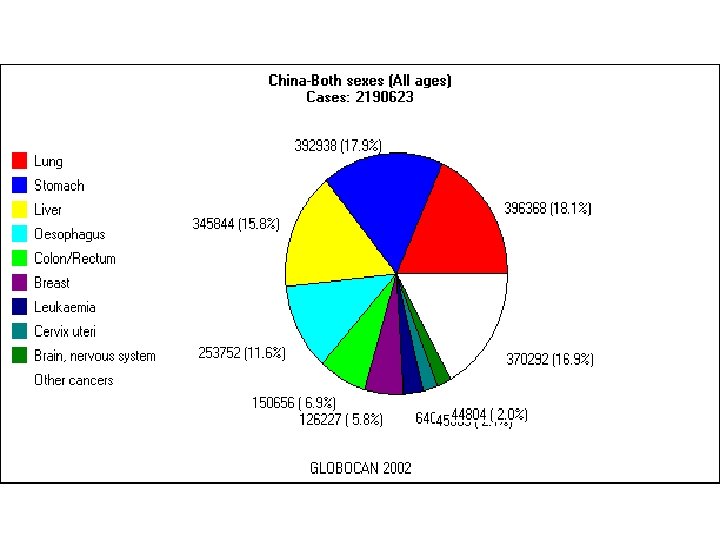
 CANCER INCIDENCE “Burden” of cancer as number of new cases • Priority for cancer control (prevention, treatment) • Estimating the resources required, based on numbers of new cases ( by age, stage, etc)
CANCER INCIDENCE “Burden” of cancer as number of new cases • Priority for cancer control (prevention, treatment) • Estimating the resources required, based on numbers of new cases ( by age, stage, etc)
 CERVIX BREAST rural urban rural MORTALITY TRENDS: CHINA 1987 -1999 urban
CERVIX BREAST rural urban rural MORTALITY TRENDS: CHINA 1987 -1999 urban
 Estimates and projections of national cancer incidence & mortality
Estimates and projections of national cancer incidence & mortality
 PLANNING & EVALUATION OF CCP MONITORING CANCER CONTROL 1 Primary prevention Time trends ? Control areas? 2 Screening & early detection • Outcomes (incidence or mortality) • Time trend studies (in relation to inputs) • Linkage with screening programme records (distinguish screened/unscreened individuals) Incidence per 100, 000 women-years • 75 Intermediate endpoints 50 ØNever screenedand stage of screen-detected cases Size screened ØEver. Incidence of interval cancers Normal test Ø Incidence of advanced cancers DENMARK Reference period 1958 -67 FINLAND ICELAND NORWAY SWEDEN 0 25 20 30 1945 40 1950 50 1955 60 1960 70 1970 80 1975 901980 1965
PLANNING & EVALUATION OF CCP MONITORING CANCER CONTROL 1 Primary prevention Time trends ? Control areas? 2 Screening & early detection • Outcomes (incidence or mortality) • Time trend studies (in relation to inputs) • Linkage with screening programme records (distinguish screened/unscreened individuals) Incidence per 100, 000 women-years • 75 Intermediate endpoints 50 ØNever screenedand stage of screen-detected cases Size screened ØEver. Incidence of interval cancers Normal test Ø Incidence of advanced cancers DENMARK Reference period 1958 -67 FINLAND ICELAND NORWAY SWEDEN 0 25 20 30 1945 40 1950 50 1955 60 1960 70 1970 80 1975 901980 1965
 PLANNING & EVALUATION OF CCP MONITORING CANCER CONTROL 1 Primary prevention Time trends ? Control areas? 2 Screening & early detection Outcomes (incidence or mortality) Time trend studies (in relation to inputs) Linkage with screening programme records (distinguish screened/unscreened individuals) Intermediate endpoints Incidence of interval cancers Size and stage of screen-detected cases Incidence of advanced cancers 3 Treatment : Study of SURVIVAL 4 Cancer care
PLANNING & EVALUATION OF CCP MONITORING CANCER CONTROL 1 Primary prevention Time trends ? Control areas? 2 Screening & early detection Outcomes (incidence or mortality) Time trend studies (in relation to inputs) Linkage with screening programme records (distinguish screened/unscreened individuals) Intermediate endpoints Incidence of interval cancers Size and stage of screen-detected cases Incidence of advanced cancers 3 Treatment : Study of SURVIVAL 4 Cancer care
 EVALUATION OF CANCER CONTROL PROGRAMMES SURVIVAL DATA Effectiveness of Treatment in delaying/preventing death BUT, consider other factors influencing survival especially earlier diagnosis
EVALUATION OF CANCER CONTROL PROGRAMMES SURVIVAL DATA Effectiveness of Treatment in delaying/preventing death BUT, consider other factors influencing survival especially earlier diagnosis
 FACTORS INFLUENCING SURVIVAL FROM CANCER Disease: Treatment: Availability Access Quality Natural history Clinical extent Definitions Host: Early Detection: Age Sex Early clinical detection SES Screening Comorbidity Behaviour
FACTORS INFLUENCING SURVIVAL FROM CANCER Disease: Treatment: Availability Access Quality Natural history Clinical extent Definitions Host: Early Detection: Age Sex Early clinical detection SES Screening Comorbidity Behaviour
 Trends in 5 -Year Relative Survival from Selected Cancers in Women, Singapore, 1968 -92
Trends in 5 -Year Relative Survival from Selected Cancers in Women, Singapore, 1968 -92
 PLANNING & EVALUATION OF CCP MONITORING CANCER CONTROL 1 Primary prevention Time trends ? Control areas? 2 Screening & early detection Outcomes (incidence or mortality) Time trend studies (in relation to inputs) Linkage with screening programme records (distinguish screened/unscreened individuals) Intermediate endpoints Incidence of interval cancers Size and stage of screen-detected cases Incidence of advanced cancers 3 Treatment : Study of SURVIVAL 4 Cancer care
PLANNING & EVALUATION OF CCP MONITORING CANCER CONTROL 1 Primary prevention Time trends ? Control areas? 2 Screening & early detection Outcomes (incidence or mortality) Time trend studies (in relation to inputs) Linkage with screening programme records (distinguish screened/unscreened individuals) Intermediate endpoints Incidence of interval cancers Size and stage of screen-detected cases Incidence of advanced cancers 3 Treatment : Study of SURVIVAL 4 Cancer care
 EVALUATING CLINICAL CARE IN CCP Patterns of clinical care • Place of treatment • Percent treated by “specialists” • Percent of cases with adequate staging • Percentage on treatment protocols • Delay (diagnosis-treatment)
EVALUATING CLINICAL CARE IN CCP Patterns of clinical care • Place of treatment • Percent treated by “specialists” • Percent of cases with adequate staging • Percentage on treatment protocols • Delay (diagnosis-treatment)
 ã Why do we need cancer registries ã Current situation in Asia
ã Why do we need cancer registries ã Current situation in Asia
 ASIA – 12 COUNTRIES REPRESENTED Russia Kazakhstan Mongolia Kyrgyzstan Turkey JAPAN KOREA Turkmenstan Tajikstan CHINA Syria ISRAEL Iran Iraq Lebanon Afghanistan Jordan PAKISTAN KUWAIT Egypt Bhutan Nep al Qatar. Saudi Arabia U. A. E. Karachi INDIA Bangladesh Burma Laos PHILIPPINES OMAN Sudan Yemen THAILAND VIET NAM Cambodia Arabian Sea Sri Lanka Malaysia So m al ia Ethiopia Uganda Kenya SINGAPORE Manila & Rizal
ASIA – 12 COUNTRIES REPRESENTED Russia Kazakhstan Mongolia Kyrgyzstan Turkey JAPAN KOREA Turkmenstan Tajikstan CHINA Syria ISRAEL Iran Iraq Lebanon Afghanistan Jordan PAKISTAN KUWAIT Egypt Bhutan Nep al Qatar. Saudi Arabia U. A. E. Karachi INDIA Bangladesh Burma Laos PHILIPPINES OMAN Sudan Yemen THAILAND VIET NAM Cambodia Arabian Sea Sri Lanka Malaysia So m al ia Ethiopia Uganda Kenya SINGAPORE Manila & Rizal
 India Afghanistan 9 registries INDIA – 9 registries China Pakistan Delhi Nepal Bhutan Bangladesh Ahmedabad Burma Nagpur Mumbai (Bombay) Poona Bay of Bengal Arabian Sea Bangalore Chennai (Madras) Karunagappally Trivandrum Sri Lanka
India Afghanistan 9 registries INDIA – 9 registries China Pakistan Delhi Nepal Bhutan Bangladesh Ahmedabad Burma Nagpur Mumbai (Bombay) Poona Bay of Bengal Arabian Sea Bangalore Chennai (Madras) Karunagappally Trivandrum Sri Lanka
 South-East Asia China Burma VIETNAM Hanoi Chiang Mai Laos Lampang THAILAND Khon Kaen Bangkok Cambodia Andaman Sea Gulf of Thailand Ho Chi Minh City South China Sea Songkhla Malaysia Indonesia Malaysia SINGAPORE Indonesia
South-East Asia China Burma VIETNAM Hanoi Chiang Mai Laos Lampang THAILAND Khon Kaen Bangkok Cambodia Andaman Sea Gulf of Thailand Ho Chi Minh City South China Sea Songkhla Malaysia Indonesia Malaysia SINGAPORE Indonesia
 Japan and Korea Russia China Yamagata KOREA Kangwha Seoul Miyagi North Pacific Ocean Daegu JAPAN Busan Hiroshima Saga Nagasaki East China Sea Osaka
Japan and Korea Russia China Yamagata KOREA Kangwha Seoul Miyagi North Pacific Ocean Daegu JAPAN Busan Hiroshima Saga Nagasaki East China Sea Osaka
 Russia Kazakhstan China 10 Mongolia registries Korea Beijing Tianjin Cixian Wuhan Jiashan Qidong County Shanghai Ne pa l Bhutan Changle India Taiwan Bangladesh Burma Viet Nam Hong Kong Laos South China Sea Bay of Bengal Thailand Philippines
Russia Kazakhstan China 10 Mongolia registries Korea Beijing Tianjin Cixian Wuhan Jiashan Qidong County Shanghai Ne pa l Bhutan Changle India Taiwan Bangladesh Burma Viet Nam Hong Kong Laos South China Sea Bay of Bengal Thailand Philippines
 CI 5 incidence data % population coverage, 1995 26. 2% 32% 4. 7% 3% 12. 7% 1 % 82%
CI 5 incidence data % population coverage, 1995 26. 2% 32% 4. 7% 3% 12. 7% 1 % 82%
 INTERNATIONAL ASSOCIATION OF CANCER REGISTRIES Membership 447 385 402 366 Oceania 191 Europe 134 N. America S. America Asia Africa 91 92 ASIAN MEMBERS 458
INTERNATIONAL ASSOCIATION OF CANCER REGISTRIES Membership 447 385 402 366 Oceania 191 Europe 134 N. America S. America Asia Africa 91 92 ASIAN MEMBERS 458
 Incidence data % population coverage, around 1995 36. 5% 99% 7% 19. 6% 8 % 10. 5% 86%
Incidence data % population coverage, around 1995 36. 5% 99% 7% 19. 6% 8 % 10. 5% 86%
 ã Why do we need cancer registries ã Current situation in Asia ã What’s new?
ã Why do we need cancer registries ã Current situation in Asia ã What’s new?
 GULF STATES: 6 population-based registries Now joined by Yemen: The Aden Cancer Registry
GULF STATES: 6 population-based registries Now joined by Yemen: The Aden Cancer Registry
 THE INDIAN CANCER ATLAS Using pathology-based data to obtain clues about geography of cancer
THE INDIAN CANCER ATLAS Using pathology-based data to obtain clues about geography of cancer
 Per 100, 000 Stomach (ICD") Fig 8. Districtwise Microscopic Age Adjusted Incidence Rates (MAAR) Per 100, 000 Stomach (ICD 10 : C 16) Males Year 2001 - 2002 Imphal West (12. 2) Dimapur (10. 0) Lahul & Spiti (15. 1) Senapati (8. 7) Tamenglong (9. 1) Churachandpur (19. 2) Kolasib (56. 1) East Sikkim (15. 4) North Sikkim (27. 7) Kohima (34. 0) Ukhrul (11. 2) Aizawl (47. 0) Champai (46. 3) Serchhip (70. 2) Saiha (23. 0) Lawngtlai (10. 2) Lunglei (25. 3) Mamit (53. 4) Thiruvallur (10. 7) Thrissur (12. 6)
Fig 8. Districtwise Microscopic Age Adjusted Incidence Rates (MAAR) Per 100, 000 Stomach (ICD 10 : C 16) Males Year 2001 - 2002 Imphal West (12. 2) Dimapur (10. 0) Lahul & Spiti (15. 1) Senapati (8. 7) Tamenglong (9. 1) Churachandpur (19. 2) Kolasib (56. 1) East Sikkim (15. 4) North Sikkim (27. 7) Kohima (34. 0) Ukhrul (11. 2) Aizawl (47. 0) Champai (46. 3) Serchhip (70. 2) Saiha (23. 0) Lawngtlai (10. 2) Lunglei (25. 3) Mamit (53. 4) Thiruvallur (10. 7) Thrissur (12. 6)
 Population -based cancer registry Active surveillance Tehran
Population -based cancer registry Active surveillance Tehran
 KOREA: National population-based cancer registry network Using the existing “Korean Central Cancer Registry” – a hospital based system providing national level, but incomplete, data since 1980.
KOREA: National population-based cancer registry network Using the existing “Korean Central Cancer Registry” – a hospital based system providing national level, but incomplete, data since 1980.
 THAILAND Cancer in Thailand, vol III based on the established 5 Registries There another 5 -6 start-ups
THAILAND Cancer in Thailand, vol III based on the established 5 Registries There another 5 -6 start-ups
 CHINA: Survey of cancer registries nationwide Information from 48 PBCRs They cover 5. 7% population Qiqihaer Haerbin of China Wuwai Tianjin Boli Ningan Shenyang Anshan Chicheng Beijing Jiamusi Dalian Ganyu Zanghuang Jiaxian Yangcheng Huaian Shexian Linqu Cixian Feicheng Linzhou Jianhu Taixing Luoyang Jintan Lueyang Yanting Jiaxing Wuhan To be published in Eur. J. Cancer Prevn. Shanghai Jiashan Haining Hangzhou Changle Gejiu Tin Mine Fusui Guangzhou (1, 2) Shenzhen Sihui Hong Kong Zhongshan Dafeng Yangzhong Haian Haimen Qidong Shanghai
CHINA: Survey of cancer registries nationwide Information from 48 PBCRs They cover 5. 7% population Qiqihaer Haerbin of China Wuwai Tianjin Boli Ningan Shenyang Anshan Chicheng Beijing Jiamusi Dalian Ganyu Zanghuang Jiaxian Yangcheng Huaian Shexian Linqu Cixian Feicheng Linzhou Jianhu Taixing Luoyang Jintan Lueyang Yanting Jiaxing Wuhan To be published in Eur. J. Cancer Prevn. Shanghai Jiashan Haining Hangzhou Changle Gejiu Tin Mine Fusui Guangzhou (1, 2) Shenzhen Sihui Hong Kong Zhongshan Dafeng Yangzhong Haian Haimen Qidong Shanghai
 ã Why do we need cancer registries ã Current situation in Asia ã What’s new ã The role of IACR
ã Why do we need cancer registries ã Current situation in Asia ã What’s new ã The role of IACR
 International Association of Cancer Registries Founded in 1966 Aims: To improve quality of data and comparability between registries To disseminate information on the uses of cancer registry data Ottawa, 1992
International Association of Cancer Registries Founded in 1966 Aims: To improve quality of data and comparability between registries To disseminate information on the uses of cancer registry data Ottawa, 1992
 SUPPORT TO CANCER REGISTRIES 1. International Standards 2. Publications related to cancer registration 3. Consultancy (+ WHO regions) 4. Training of staff 5. Fellowships 6. Computer software
SUPPORT TO CANCER REGISTRIES 1. International Standards 2. Publications related to cancer registration 3. Consultancy (+ WHO regions) 4. Training of staff 5. Fellowships 6. Computer software
 CANCER REGISTRATION PRINCIPLES AND METHODS
CANCER REGISTRATION PRINCIPLES AND METHODS
 Comparability and quality control in Cancer Registration Manual for Cancer Registry Personnel ICD Conversion Programs for Cancer International Classification of Childhood Cancer 1996 Guidelines on Confidentiality in the Cancer registry Histological Groups for Comparative Studies
Comparability and quality control in Cancer Registration Manual for Cancer Registry Personnel ICD Conversion Programs for Cancer International Classification of Childhood Cancer 1996 Guidelines on Confidentiality in the Cancer registry Histological Groups for Comparative Studies
 IACR MEETINGS 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 Hamburg, Germany Quito, Ecuador Ottawa, Canada Bratislava, Slovakia Bangalore, India Rio de Janeiro, Brazil Edinburgh, UK Abidjan, Ivory Coast Atlanta, USA Lisbon, Portugal Khon Kaen, Thailand Havana, Cuba Tampere, Finland 2003 Honolulu, Hawaii
IACR MEETINGS 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 Hamburg, Germany Quito, Ecuador Ottawa, Canada Bratislava, Slovakia Bangalore, India Rio de Janeiro, Brazil Edinburgh, UK Abidjan, Ivory Coast Atlanta, USA Lisbon, Portugal Khon Kaen, Thailand Havana, Cuba Tampere, Finland 2003 Honolulu, Hawaii
") Beijing, China, 2004 THANK YOU. See you next year (and before that, I hope!)
Beijing, China, 2004 THANK YOU. See you next year (and before that, I hope!)