1b50ca67181cce4f5fb7ddefdf31edfe.ppt
- Количество слайдов: 27



Can Health Information Exchanges Improve Public Health? Farzad Mostashari, MD SM New York City Department of Health and Mental Hygiene fmostash@health. nyc. gov

Is There a Problem? • State/local officials are not engaged • Inadequate representation of PH perspectives (and state/local officials) in NHIN institutions • A lost opportunity (at best) • Standards (and investments) that don’t take PH into consideration could have negative impact

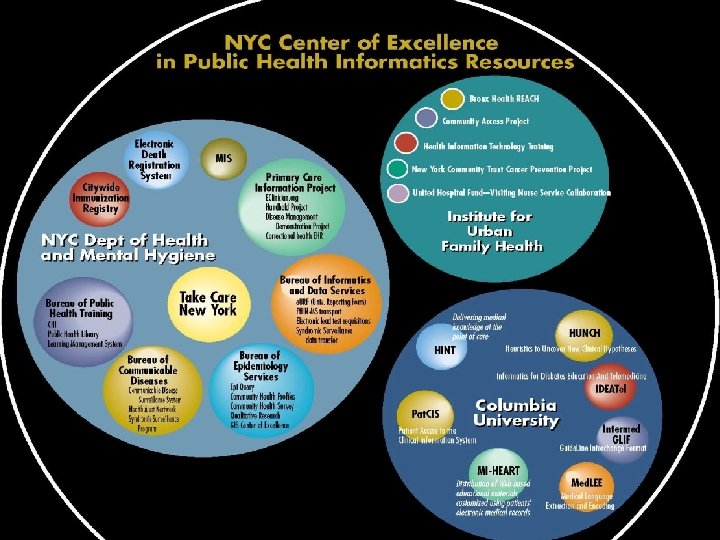
Active Government Role in NY • NY City Mayoral EHR initiative – $27 million for interoperable EHRs • NY State HEAL-NY Bond Grants – $53 million to 26 proposed HIEs (9 in NYC) – Requirement for “Public Health Reporting” • DOHMH is partner in multiple HIEs • NYC Center of Excellence in Public Health Informatics (CDC)

PCIP Roadmap 1. Citywide EHR Network • • 2. Procure “best of breed” Electronic Health Record Add Public Health/Quality Improvement functionality Prepare Network and Hardware Infrastructure Extend to Correctional Health and community providers Citywide Quality Improvement Network • • • 3. Citywide automated quality measurement and reporting Decision supports and other quality improvement Extend to other ambulatory EHRs Citywide Health Information Exchange Network • • • Interfaces to other systems (e. g. , HHC) Syndromic and Notifiable Disease Reporting Citywide Immunization, Lead Registries, and School Health Medicaid medication history Linkages to RHIOs
 All ADT from Member 2) NYCLIX Central Data Request 3)")
Radiology Cardiology ADT 1) All ADT from Member 2) NYCLIX Central Data Request 3) NYCLIX Data Source Result Care Provider Transactions 1) NYCLIX Care Provider Request Data Repository 4) NYCLIX Central Result NYCLIX Layer Security Mgmt & Access Controls Participating Entity & Level NYCLIX Application Layer Lab Data Source Transactions NYCLIX Central Presentation Pharm Interface Engine/API CIS/EMR Technical Components Strawman Interface Engine Participating Member (both care provider & data source) Patient matching & Record Locator Aggregation & Standardization Audit Trails NYCLIX Web • NYCLIX Data Repository • NYCLIX Audit & Control Public Health Member Center • NYCLIX Layer can be provided by NYCLIX or internally built according to standards • NYCLIX Central acts a clearing house for all requests and routes transactions based on participation level, patient matching, and record locator services • Member sends ADT for all patients registered/admitted • Request for NYCLIX information can be initiated by member via Web or triggered via ADT in member’s ED • Request for Member information is initiated by NYCLIX central to each member who has patient in record locator • ADT transaction from members comprise data supporting record locator and patient matching services. No clinical data is stored • Security management and access controls govern who has access to what

Pharm Lab PACS Cards ADT EMR Pharm Interface Engine/ API Lab PACS Cards ADT EMR Interface Engine/ API Data Repository Pub Hlth RHIO 1 RHIO 2 (MPI, Audit, Authentication, etc) Public Health Data Repository Interface Engine/ API Pharm Lab PACS Cards ADT EMR

Prior Conceptual Framework • Leverage infrastructure developed for RHIOs • Reduce burden of public health reporting requirements • Standards-based messaging to population quality warehouse – – – Demographic (age group, zip, gender, “hashed ID”) Encounter data (Chief complaint, disch. dx, dispo) Problem list (Diabetes, CAD) Physical exam (measured temperature, BP) Procedures (mammo, colonoscopy, immuniz. , eye exam) Lab Results (A 1 C, lipids, viral testing results, lead) • Functions – Clinical Preventive Services – Quality Benchmarking – Infection Disease and Outbreak Surveillance

Health Information Exchange FIND Provider asks if there are records for his/her patient Source sends index information Index sends location of any records LO C AT OR Patient Index GET Individual Care Providers Provider asks for and receives records De-Identified Data Message Transfer SEND Data Sources Records are sent to Provider Source may push data for reporting G IN DA TA RT PO RE Public Health Reporting Router Source: © 2004 The Markle Foundation Graphic adapted from Tom Benthin original.

10 Public Health Use Cases Send • Mandated Laboratory Reporting • Mandated Clinical Reporting • Non-mandated Laboratory Reporting • Non-mandated Clinical Reporting • Population-level Quality Reporting Find 6. Mass Casualty Events Get 7. Public Health Investigation 8. Disaster Medical Response 9. Patient-level Public Health Alerting 10. Population-level Public Health Alerting

“Send” • Interface engines and standardized clinical data repositories at each federated site • Automated algorithms could identify and report events of public health significance directly from data sources Data Sources SEND Source may push data for reporting G IN RT PO RE Public Health Reporting Router DA TA

1. Mandated Laboratory Reporting • Public health surveillance cornerstone • Electronic lab reporting improves timeliness, but adoption has been slow due to local mapping • HIE’s standardized “edge” data repositories could facilitate electronic lab reporting Data Sources • Named data Source may SEND push data for reporting G IN RT PO RE Public Health Reporting Router DA TA

2. Mandated Clinical Reporting • Under-reporting by physicians very common • Automated algorithms could trigger review based on diagnoses, medications, and procedures • Ambulatory EHR example (Klompas) Data • Named data Sources SEND Source may push data for reporting G IN RT PO RE Public Health Reporting Router DA TA

3. Non-mandated Lab Reporting • Not all diseases are “notifiable” by law • Some common diagnoses (Abx resistance, viral dz) may not require individual action, but population trends can inform public health actions • Anonymized or aggregated Source may Data Sources SEND push data for reporting Public Health G IN RT PO RE Reporting Router DA TA
 • Pre-diagnostic data (e. g. , ED chief")
4. Non-mandated Clinical Reporting (“Syndromic Surveillance”) • Pre-diagnostic data (e. g. , ED chief complaints, measured temperature) tied to statistical algorithms can provide real-time outbreak alerting and disease trends • Anonymized or aggregated Source may • Investigable push data for Data Sources SEND reporting Public Health G IN RT PO RE Reporting Router DA TA
 needed for performance")
5. Population-level Quality Reporting • Core data elements (medications, procedures, diagnoses) needed for performance indicators • Reporting to quality data warehouse • pseudonymized or aggregated SEND Source may push data for reporting Public Health G IN RT PO RE Reporting Router Data Sources DA TA

“Find” • Master Patient Index • Aka “Record Locator Service” • Demographic data + ADT messages Patient Index Provider asks if there are records for his/her patient LO C Index sends location of any records Individual Care Providers Source sends index information AT OR Data Sources
 • Common need to")
6. Mass Casualty Events • Dislocation and confusion (9/11, Katrina) • Common need to meet overwhelming volume of “missing person” requests • RLS, limited to recent ADT messages Patient Index Call center asks if there are records for missing person LO C Index sends location of any records Emergency Call Centers Source sends index information AT OR Data Sources

“Get” • Individual queries for patient data • Typically for treatment purposes GET Individual Care Providers Provider asks for and receives records Message transfer Data Sources Records are sent to Provider
 for dislocated")
7. Disaster Medical Response • Improved medical care (including public health issues) for dislocated individuals and refugees • Authorization rules may be relaxed during emergency GET Individual Care Providers Provider asks for and receives records Message transfer Data Sources Records are sent to Provider

8. Public Health Investigation • Cases reported through other means (e. g. , laboratory reporting) • “shoe leather” epidemiology can be time consuming and labor intensive • Rapid investigation feasible (“armchair”) • Public health authorization to receive clinical data GET Public Health Message transfer Public Health asks for and receives records Data Sources Records are sent to Public Health

9. Patient-level Public Health Alerting • Public Health acts as data source • ED physician querying HIE could receive patient-specific public health alert (e. g. active TB, sought-for contact) • Isolation, decreased nosocomial spread • Early notification back to public health GET Individual Care Providers Provider asks for and receives records Message transfer Public Health Records are sent to Provider

10. Population-level Public Health Alerting • HIE serves as gateway for relevant epidemiologic data to providers (patients) • Ideally in context of patient and practice (e. g. age/zip, ED vs. Ambulatory) – Trends in influenza or asthma – Antibiograms – Preventive services recommendations GET Individual Care Providers Provider asks for and receives records Message transfer Public Health Records are sent to Provider

10 Public Health Use Cases FIND LO C AT OR GET Data Requestor Data Sources SEND G IN RE RT PO DA TA

Universal public health node? Patient Queries: Anonymized Line Lists OR Analytic Queries: Mass Casualty- 311 Patient Locator Non-Mandated Reporting Disaster Medical Response • Syndromic Surveillance Mandated Reporting • Viral (incl. Influenza) Surveillance Public Health Investigation • Abx resistance patterns Tuberculosis All Points Bulletin (APB) • Quality Reporting

New RHIO Requirements? • Ability to distribute analytic queries – Line lists – Aggregation queries (counts, num/denom) • • Anonymization & Reidentification Aggregation with ability to drill down/ audit Standard Health Query Language? Messaging standards for aggregate information?

Conclusion • HIEs can have many potential benefits for public health agencies • Demonstration of public health value may help sustain HIEs financially • Involvement of public heath agencies in the design, governance, and funding of HIEs in their communities is necessary for these goals to be realized
1b50ca67181cce4f5fb7ddefdf31edfe.ppt