f2e0a5c5bd09b034a51deaded7ce3e99.ppt
- Количество слайдов: 63



Bipolar Disorder In Primary Care Settings Christopher Schneck, M. D. Associate Professor of Psychiatry Director, Outpatient Consultation Services University of Colorado Denver Depression Center Aurora, CO

Disclosure: Funding Sources NIMH No pharmaceutical funding

Case Example

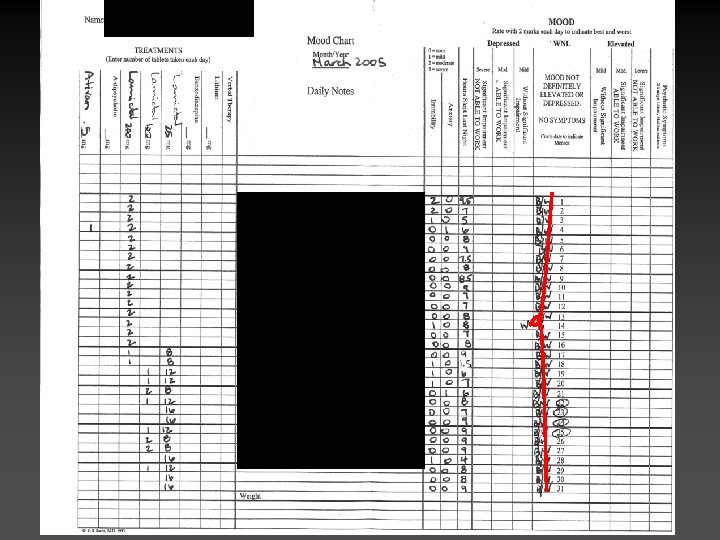
Patient L. R. • 33 year old single female, presents with chronic depression. – Depressed for 15 years – Current symptoms: hypersomnic, eating more, craves carbohydrates/sweets, feels like she is “nailed to the bed in the mornings, ” crying spells, not suicidal but sometimes “prays she will not wake up, ” irritable, anxious. – Never psychotic; no suicide attempts.

Patient L. R. • Denies manic symptoms. At times, can feel more self-confident, “project a different self, ” more impulsive. • No family history of mood disorder • Past Medical Hx: – Appendectomy – Mild asthma • Working 3 jobs; wants to return to graduate school • Intermittent alcohol problems • In psychotherapy

Patient L. R. • All antidepressants “work for a while, then stop. ” – – – – Paroxetine (Paxil) Fluoxetine (Prozac) Sertraline (Zoloft) Venlafaxine (Effexor) Buproprion (Wellbutrin) Amphetamine/d-amphetamine (Adderall) Escitalpram (Lexapro) Nefazodone (Serzone)

Next Step? Diagnosis? Treatment?

Bipolar Disorder in Patients Treated for Depression in a Family Medicine Clinic 21% MDQ+ 649 Hirschfeld RM, et al. J Am Board Fam Pract. 2005; 18: 233 -239.

Waiting Room Patients in a Family Practice Bipolar 8% 10% MDQ+ Neither 12% Depression 80% 1146 Outpatients Das AK, et al. JAMA. 2005; 293(8): 956.

Challenges in the Diagnosis and Treatment of Bipolar Disorder • Unrecognized Often • Untreated • Misdiagnosed • Inadequately treated • Worsened by wrong treatment Ghaemi SN, et al. Can J Psychiatry. 2002; 47: 125 -134.

Misdiagnosis Percent of Bipolar Disorder Initial Diagnosis Hirschfeld RM, et al. J Clin Psychiatry. 2004; 65(suppl 15): 5 -9.

Possible Red Flags • Antidepressant Failure • Increased irritability/agitation on antidepressants • Post-partum depression • Seasonal mood changes • Legal, interpersonal, occupational chaos Marchand WR. Hosp Physician. 2003; 39: 21 -30. Manning JS. Curr Psychiatry. 2003; 2: 6 -9. Geller B, Luby J. J Am Acad Child Adolesc Psychiatry. 1997; 36: 1168 -1176. Akiskal HS, et al. J Affect Disord. 1983; 5: 115 -128.

Possible Red Flags • Rapid onset/offset • “Too many to count” • Psychosis • Family history • Substance abuse

Clinical Features of Bipolar Disorder

Symptom Domains of Bipolar Disorder Manic Mood and Behavior • Euphoria • Grandiosity • Pressured speech • Impulsivity • Excessive libido • Recklessness • Social intrusiveness • Diminished need for sleep Psychotic Symptoms • Delusions • Hallucinations Dysphoric or Negative Mood and Behavior • • • BIPOLAR DISORDER Depression Anxiety Irritability Hostility Violence or suicide Cognitive Symptoms • • Racing thoughts Distractibility Disorganization Inattentiveness Slide courtesy of Keck PE Jr. ; adapted from Goodwin FK, Jamison KR. Manic-Depressive Illness. Oxford University Press: New York, NY; 1990.

Time Depressed vs. Manic 37: 1 Percent of Weeks depressed Weeks manic 3: 1 1. Judd LL et al. Arch Gen Psychiatry. 2002; 59: 530 -537. 2. Judd LL et al. Unpublished data.

Psychosocial Impairment: Depression More Impairing than Mania Percent With Disruption* Due to depressive symptoms Due to manic symptoms 35 32 30 25 20 27 23 20 22 17 15 10 5 0 Work/School P < 0. 01 Social/Leisure P < 0. 0001 *Marked or extreme over past 4 weeks Hirschfeld RM. Eur Neuropsychopharmacol. 2004; 14(suppl 2): S 83 -S 88. Family Life P < 0. 0001

Mania Depression

Bipolar I vs Bipolar I II Bipolar II • Manic or mixed episode • Hypomania + major • • depression • Female: male = 2: 1 • Diagnostic challenges: Highly familial Female: male = 1: 1 Suicide: 10%– 15% 60% Comorbid substance – Hypomania not experienced as “abnormal” – Prior hypomania often not reported American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision. Washington, DC: American Psychiatric Association; 2000.

The Spectrum of Bipolar Disorder Major depression w/ strong family hx of bipolar disorder Rapidly changing mood swings Antidepressant-induced manias & hypomanias Bipolar II Secondary manias Bipolar I Cyclothymia Major Depression Bipolar Spectrum Disorders Gorman JM, Sullivan G. J Clin Psychiatry. 2000; 6(1 Suppl 1): 13 -16. Bipolar
 19. 6 24.")
Difficulties in Diagnosis: Bipolar Patients Previously Diagnosed with Unipolar MDD (N=29) 19. 6 24. 7 25. 2 30 33. 2 34. 3 Depression DX: Bipolar Mania 9. 1 years Ghaemi SN et al. J Clin Psych 61: 10, 2000

Consequences of Misdiagnosis ATD Monotherapy Switches, Cycling ↑ Suicide Attempts ↑ Comorbidity ↑ Mortality ↑ Psychosocial Impairment Goldberg JF, Ernst CL. J Clin Psychiatry. 2002; 63: 985 -991. Goldberg JF, Truman CJ. Bipolar Disord. 2003; 5: 407 -420.

Reasons for Misdiagnosis • Hypomania hard to identify – Patients typically do not seek care for hypomania – Patients often omit hypomania from clinical histories • Patients tend to seek care during depressive episode • Bipolar II may be common in primary care setting Zylstra RG, et al. Primary Care Companion J Clin Psychiatry. 1999; 1: 47 -49.

Can you tell the difference between bipolar & unipolar depression?

Features Indicative of Bipolar versus Unipolar Depression Bipolar Substance Abuse Family History First Episode < 25 yrs Postpartum Illness Psychosis < 35 yrs Atypical Features Rapid On/Off Pattern Recurrent MDE (> 3) Unipolar Very High Moderate Almost Uniform Sometimes Very Common Sometimes Highly Predictive Uncommon Common Occasional Typical Unusual Common Unusual Brief MDE (avg < 3 months) Suggestive MDE = major depressive episode Kaye NS. J Am Board Fam Pract. 2005; 18: 271 -281. Uncommon

Screening for Bipolar Disorder

Bad day at the office
 + - Greater than 7 “yes” responses -”yes” to")
The Mood Disorder Questionnaire (MDQ) + - Greater than 7 “yes” responses -”yes” to Question 2 -”Moderate” or “Serious” to Question 3 7 or fewer “yes” responses -no to Question 2 -”No problem” or “minor problem” to Question 3 Hirschfeld RMA, et al. Am J Psychiatry. 2000; 157: 1873 -1875. Hirschfeld RMA, et al. Am J Psychiatry. 2003; 160: 178 -180. Hirschfeld RMA, et al. J Clin Psychiatry. 2003; 64: 53 -59. www. psycheducation. org/PCP/handouts/mdq. doc

Bipolar Spectrum Diagnostic Scale √ √ √ √ Ghaemi SN et al. J Affect Dis, vol 84, 2005 √ √

“Has there ever been a time in your life, when, for several days or even weeks, you slept a lot less than usual and found you didn’t miss it? ”

Treatment

Suicide Risk: Various Conditions Observed/Expected 1. 8 Malignancy 7. 1 Personality D/O 5. 9 Alcohol 19. 2 Mixed Drugs 8. 5 Schizophrenia Bipolar Disorder 15. 0 20. 3 Major Depression History of Suicide Attempt 38. 4 0 0 Inskip H et al. Br J Psych 1998; 172: 35 -37. 5 5 10 10 15 1 5 20 20 25 2 5 30 30 35 3 40 40 5 36

Bipolar Disorder: Untreated vs Treated Standardized Mortality Ratios 29. 2* *P < 0. 001 †P < 0. 05 Untreated Treated Zurich cohort, n = 406 1959– 1997 6. 4 1. 4* 0. 6 Neoplasm 2. 2*1. 7 1. 6† 1. 3 Cardiovascular Cerebrovascular Accidents 2. 0* 1. 3 1. 6 2. 0 Adapted from Angst F et al. J Affect Disorder. 2002; 68: 167 -181. Suicide 2. 2* 1. 3 Other All Causes 37

Treatment Psychotherapy Medications Improved Outcome

Therapies With Bipolar Disorder Indications Therapy Valproic acid Lithium Carbamazepine Divalproex Bipolar Mania Bipolar Depression Maintenance Relapse Prevention No No No √ Yes No* No No Yes No Aripiprazole √ Yes No Quetiapine Risperidone Ziprasidone *Limited √ Yes No No** No √ No No Olanzapine+fluoxetine (OFC) Yes No Lamotrigine Olanzapine √ No √ √ √ Yes Yes No No No data; **Emerging data Physicians’ Desk Reference®. 59 th ed. Montvale, NJ: Medical Economics Co; 2005.

Treatment of Mania

Response Rates Percent Responders in 20 Acute Mania Trials From Ketter TA. Review of Psychiatry, vol 24, no. 3

Risperidone vs Placebo in Acute Mania: Mean Reduction in YMRS Score Mean Change in Total YMRS Score Baseline Day 3 Week 1 Week 2 Week 3 Endpoint 0 LOCF analysis; *P < 0. 001 risperidone vs placebo -2 Placebo (n = 125; BL YMRS = 29. 2) -4 -6 * -8 Risperidone (n = 134; BL YMRS = 29. 1 ) Median dose 4. 1 mg/day -10 -12 * * * BL = Baseline Hirschfeld RM et al. Presented at ACNP Annual Meeting. San Juan, Puerto Rico. December 2002. *

Overview of 15 Acute Mania Monotherapy Studies Placebo Atypical Antipsychotics Percent Responders Mood Stabilizers 1950 Mg/d 1694 Mg/d 707 Mg/d 4. 9 Mg/d 16 Mg/d 575 Mg/d 121 Mg/d 28 Mg/d Adapted from Ketter TA. Advances in the Treatment of Bipolar Disorder. Review of Psychiatry, vol. 24, no. 3

Treatment of Bipolar Depression

Positive Antidepressant Trials with Adequate Sample Size* in Bipolar Depression Slide Courtesy G Sachs *Statistical Power ≥ 0. 8 to detect meaningful difference at p<. 05

Effectiveness of Adjunctive Antidepressant Treatment for Bipolar Disorder NS NS Sachs GS et al. NEJM 2007; 356(17)

Conversion to Rapid Cycling Antidepressant

Problems with Antidepressants: Mrs. A. . . ”After 10 days noticed racing & distorted thoughts, increased irritability, hostility, aggressive behavior and decreased need for sleep. She described feeling “speedy” and began driving aggressively; she later described her state as one of ‘radical agitation. ’” Schneck CD. J Clin Psychiatry 59: 12, 1998
 3.")
Antidepressant Associated with Increased Cycle Rates Episodes Odds Ratio Statistic 4+ Episodes (N=48) 3. 8 95% CI=1. 2 -2. 3, p=0. 001 2 -3 Episodes (N=225) 2. 0 95% CI=1. 4 -2. 9, p=0. 0001 One episode (N=263) 1. 7 95% CI=1. 7 -8. 5, p=0. 001 Schneck et al. Am J Psych 165 (3), 2008

Time to Relapse for Patients with Bipolar Disorder Who Discontinued Antidepressant Treatment Within 6 Months of Remission or Continued Treatment Beyond 6 Months Proportion of Subjects Not Relapsing 1. 0 Medication Discontinuation Group Medication Continuation Group 0. 8 0. 6 0. 4 0. 2 0. 0 0 8 16 24 32 Number of Weeks Until Relapse 40 48 Altshuler L et al. Am J Psych 160, 2003

Treatment Response in Modern Trials with >100 Depressed Bipolar Subjects Placebo Response Rate Active Placebo Difference Adapted from Ketter TA. Advances in the Treatment of Bipolar Disorder. Review of Psychiatry, vol. 24, no. 3
 the Book")
Psychotherapy by (buy) the Book


Be on the look-out for: • • Repeated antidepressant failures Irritability/agitation on antidepressants Severe post-partum depression Rapid onset/offset of mood changes “Too many to count” Psychosis Family history of bipolar disorder Substance abuse

Ask: • Duration of mood symptoms • Hypomanic symptoms • Friends, family • Family history • Prior response to antidepressants • MDQ or BSDS

Refer When Possible….

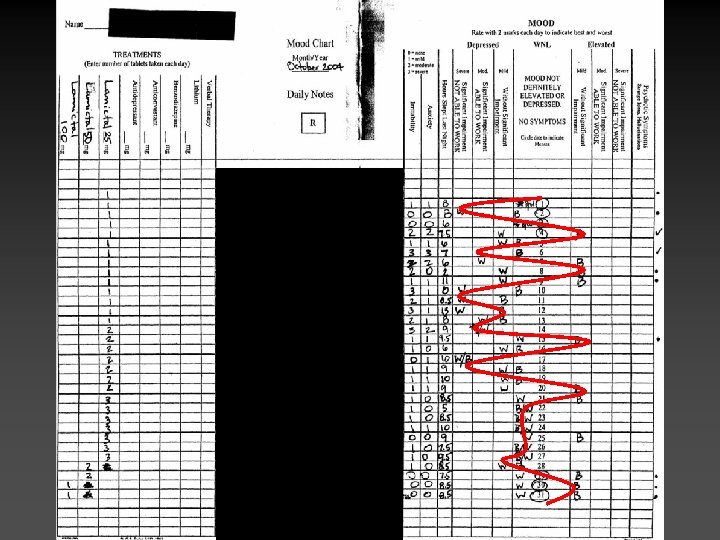
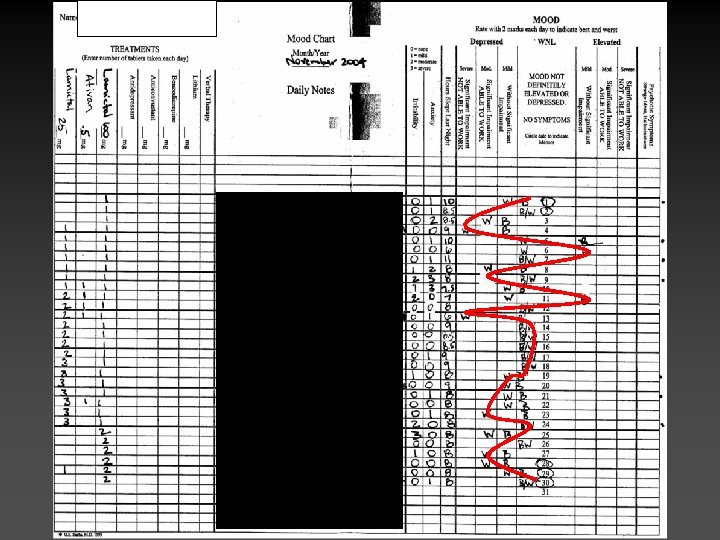
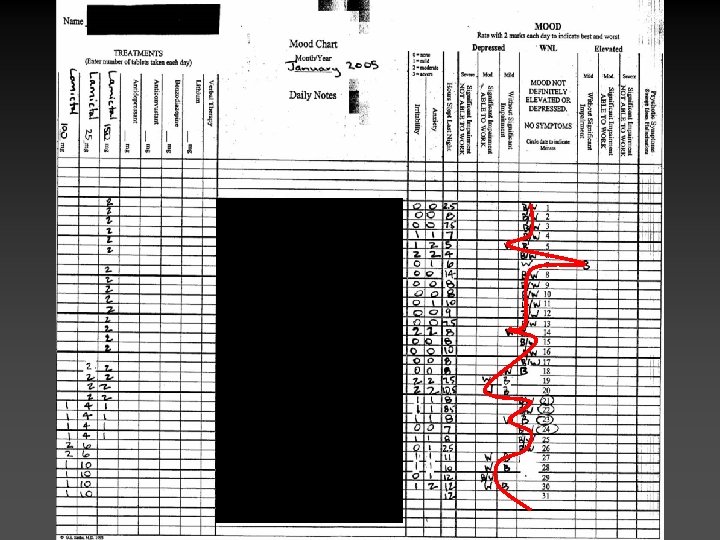
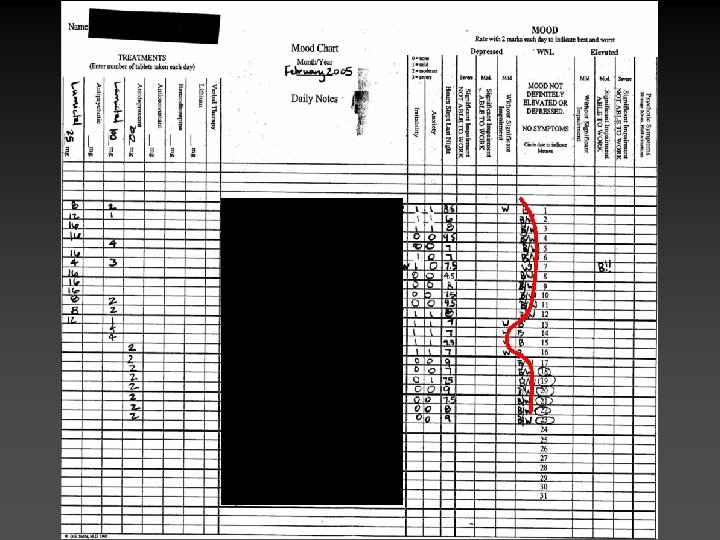
Patient L. R. • Diagnosis: Bipolar Spectrum – Collateral information: episodic irritability, pressured speech at times • Antidepressants tapered • Started on lamotrigine • Dose pushed to 400 mg daily

Questions?
f2e0a5c5bd09b034a51deaded7ce3e99.ppt