799705f0c9dca4d41c039256e2184fbe.ppt
- Количество слайдов: 43



Bieber Fever

General Data of the Neonate • • • Bb C. L. Filipino born via normal spontaneous delivery on March 5, 2012 Full term 39 5/7 weeks AOG Birth weight of 2. 91 kg Maturity Testing 40 weeks Appropriate for gestational age APGAR 9, 9

History of Present Illness • 1 st – 2 nd day of life active good suck no changes, no symptoms, discharged from tmc • 3 rd day of life patient had fever Tmax 38. 9’C

Obstetric and Maternal History • • • Age: 24 Marital Status: Single with live in partner OB score: G 1 P 1 (1001) Race: Asian/ Filipino LMP: 2 nd week of May PMP: EDD:

Obstetric and Maternal History • 1 st Trim: no tests done, UTZ + contractions took isoxsuprine 2 nd Trim: no tests done, UTZ 3 rd Trim: no tests done, UTZ • M: I: D: A: S:

Obstetric and Maternal History • • Denies history of STI No contraception / family planning used Not a planned pregnancy (-) Smoke, occasional drinker before pregnancy

Course of Labor and Delivery • Spontaneous labor 36 hrs PTA at home – (+) contractions – No fetal monitoring • Early rupture of membranes 12 hrs prior to delivery • Duration of labor was unknown • Baby was delivered by normal spontaneous vaginal delivery • Amniotic fluid was thickly meconium stained but baby had good cry and activity

Course of Labor and Delivery • Routine resuscitation was done • APGAR were: – 1 minute APGAR: 9 – 5 minute APGAR: 9

Course in the Transitional Nursery • Vitals Stable • Problems: none • Estimate of gestational age – Maturity testing 40 weeks, AGA
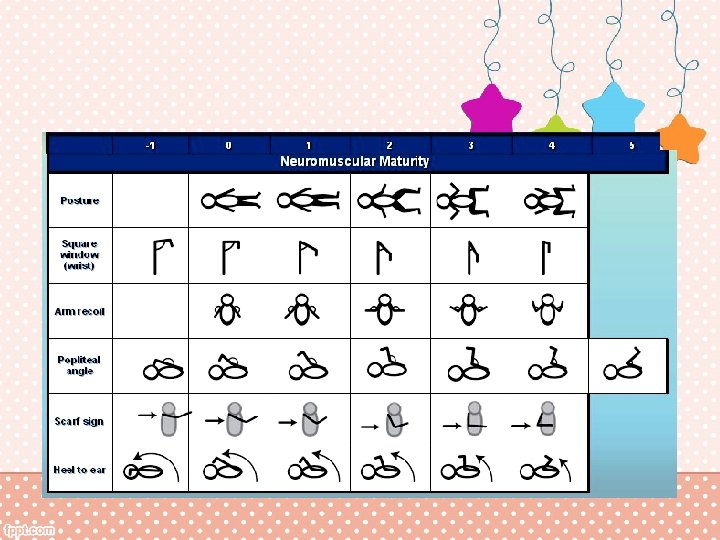
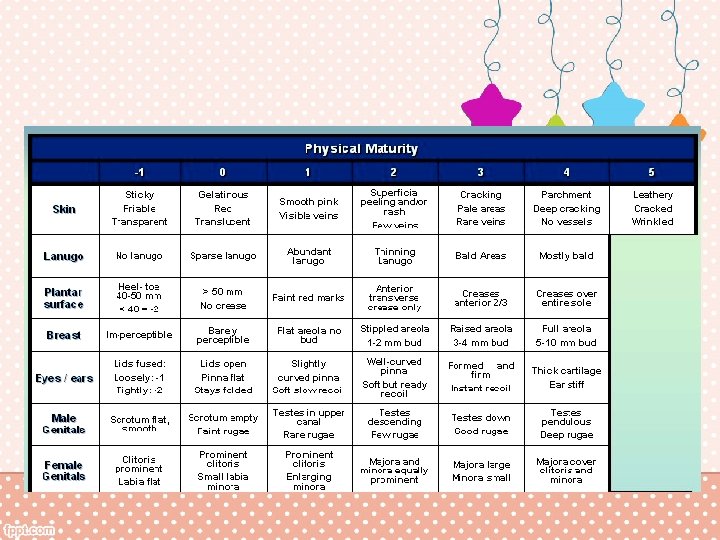

Maturity Rating Score Weeks 35 38 40 40

Family History 24 yo 3 days old

Family History • Mother and Father are not married but live together in one home • Mother and father both work in marketing • No illnesses in the family • Father: Breadwinner • Mother: Caregiver and Decision Maker

Nutritional History • Patient is purely breastfed Vaccination History • Hep B x 1
 tonic neck (+) startles")
Developmental History (+) tonic neck (+) startles

Environmental History • Lives in a one storey house with mother’s family • 7 members in one roof (mother, father, patient, maternal grandparents, and aunt, uncle) • Mother, father and patient stay in one room • Use filtered water for drinking (but patient is still purely breastfed) • With adequate ventilation, windows, cooks inside the house using a gas stove • Trash collected 3 x a week

Physical Exam General. Awake, active, good cry, pinkish in color, no retractions/ nasal flaring, no tremors/ twitching, not in cardiorespiratory distress Anthropometrics. BW: 3. 2 kg BL: 49 cm HC: 33 cm CC: 31 cm AC: 32 MA: 10

Physical Exam • HEENT. No caput, anterior fontanelle flat and palpable. Anicteric and non hemorrhagic sclerae, pink palpebral conjunctivae. No eye discharge. Equally brisk and reactive to light. Clear canal, intact tympanic membrane. Clear nasal canal, no discharge, no hyperemia. No cleft lip or palate, no lesions on oral mucosa, no hyperemia. • Neck. No masses, supple, no cervicolymphadenopathy.

Physical Exam Chest. Symmetric chest expansion, no retractions, no milk discharge, no thrills, femoral and carotid pulse are normal, resonant lungs, no murmurs. Abdomen. Globular abdomen, brownish stump, 2 arteries and 1 vein, normoactive bowel sounds, liver edge palpable at 1. 5 cm below the costal margin, spleen not palpable Hip Exam and Genital Exam. No hip dislocation, grossly normal male external genitalia, no masses, no dimples or tufts of hair on sacrum.

Physical Exam Neurologic. Patient is responsive with good cry, symmetry of mouth, symmetric expressions, intact EOMs, symmetric patellar test reflex, (+) Babinski Primary Reflex. (+) Moro, good sucking reflex Extremities. No deformities, full and equal pulses.

Salient Features • • Maternal history of UTI untreated 3 rd trim Small for gestational age Had episode of jaundice Fever Abnormal CBC Abnormal Urinalysis Unwanted Pregnancy

Initial Assessment • Live, term, 39 weeks by Pediatric Aging, delivered via NSD, to a 17 year old G 1 P 0, small for gestational age, low birth weight of 2. 3 kg, APGAR 8, 9 • Neonatal Sepsis • r/o UTI

Differentials

Congenital Pneumonia Rule in Rule out • Infection of maternal GU tract • No tests done • PE may be systemic • Systemic findings are similar to sepsis • No pulmo manifestations like retractions or alar flaring • Xray must be done

Nosocomial Infection Rule In Rule Out • Developed Fever day 3 • Usually 5 -7 days of life • No risk factors seen in the patient prematurity, LBW, invasive procedures, indwelling vascular catheters, parenteral nutrition with lipid emulsions, endotracheal tubes, ventricular shunts, alterations in the skin and/or mucous membrane barriers, frequent use of broadspectrum antibiotics, and prolonged hospital stay

Meningitis Rule In Rule Out • Maternal infection • Had fever • No fever during delivery • No reported change in sleeping or eating habits, irritability or lethargy, vomiting, high-pitched cry, or seizures • No bulging fontanelle

Diagnostics • CBC with platelet count • Blood culture and sensitivity

Plan • Admission • Antibiotic therapy – Ampicillin and Amikacin IV • Supportive therapy

Course in the wards S O Patient asleep, no febrile episodes Stable vitals, slightly yellow up to chest (10%) A P

Course in the wards S O A P

Course in the wards S O A P

Discussion

Bacterial sepsis • Confirmed: culture proven • Clinical: symptomatic + CBC/ C-reactive protein only • Early onset: first 3 -5 days of life (infection came from the mother) • Late onset: – Nosocomial: 5 -7 days of life/ after 3 rd day of life in VLBW (wt<1, 500 g) – Community Acquired: 8 -9 days, usually due to UTI, Group B beta-hemolytic strep
 • MMC: 1/1000 births (2008) • Mortality")
Incidence • PGH: 62/ 1000 births (2007) • MMC: 1/1000 births (2008) • Mortality due to sepsis is 15% in Philippines, 2004 data
/ Pneumonia – Instrumentation/ Internal Exam")
Risk Factors • Maternal – Peripartal infection: UTI/PROM/GI (diarrhea)/ Pneumonia – Instrumentation/ Internal Exam • Infant – Prematurity: immune system, thin skin, interventions like intubations, IV insertions, catheterization – Congenital anomalies (areas of mucosal breakdown) • Environment – Overcrowding, inadequate facilities – Septic home delivery

Bacterial Infections Gram Negative Gram Positive • • • E. coli Klebsiella Pseudomonas Serratia Hemophilus Bacteroides Staphylococcus Group B streptococcus Peptostreptococcus Clostridia *in bold common in Phils
 – Apnea, bradycardia, poor")
Clinical Manifestations • Asymptomatic until severe • Symptoms (non specific) – Apnea, bradycardia, poor activity, poor suck, feeding intolerance, poor tone, abdominal distension, vomiting, diaarrhea, bleeding, pallor, irritability, jaundice, rash – Tachypnea, desaturation – Hypo/hyper-glycemia – Temperature instability – Bulging fontanel, seizure, jitteriness, mottling, poor perfusion – Fever: late onset sepsis, community acquired

Diagnosis • CBC: – WBC 10, 000 -30, 000 1 st few days of life (N 5 k) – ANC: (%segmenter + % bands) x WBC = <1500 – Left shift: segmenter predominance/ immature cells – I: T (immature neutrophils to Total neutrophils ratio) > 0. 20 – Platelet < 100, 000 (N 150 k-400 k) • C-reactive protein: positive increased> 24 h after infection – Acute phase reactant

Diagnosis • Blood culture – 1 ml – Untreated mother, untreated baby • • Lumbar puncture Chest X-ray, pain abdomen Urinalysis Stool culture

Management • Antibiotics – Ampicillin and Gentamicin – Cephalosporin and aminoglycoside – Piperacillin – Tazobactam – Carbapenems – Quinolones (ciproflozacin, ofloxacin) • Supportive Therapy – Pressor for hypotensive – NPO/ TPM (food = food for bacteria) – Ventilation/ O 2 for hypotensive, apneic, bradycardic

Management – PRBC/ Platelet transfusion – Fresh frozen plasma for those developing DIC – Double volume exchange transfusion – Intravenous Immune Globulin – Granulocyte cell stimulating factor transfusion

799705f0c9dca4d41c039256e2184fbe.ppt