256b802d97214b811cf9999207b2a1e1.ppt
- Количество слайдов: 87



BACTERIAL MENINGITIS Gebre K. Tseggay, MD November 21, 2005

MAJOR CHANGES IN EPIDEMIOLOGY OF MENINGITIS SINCE THE 1990’S mainly due to the introduction of Hib vaccine n Dramatic drop in the number of H. influenzae meningitis cases n Dramatic drop in the overall number of meningitis cases n Shift in age of distribution of bacterial meningitis (median age was 15 months in 1986, but 25 yrs in 1995) n Before the 1990’s: H. infl> S. pneumoniae> N. meningitidis n Since the 1990’s: S. pneumoniae> N. meningitidis>>>H. infl. NEJM 1997; 337: 970 -6

Etiology Of Bacterial Meningitis In The US Organism H. Influnezae N. meningitidis S. pneumoniae Strep. agalactiae Listeria m. Other Unknown JAMA. 1985; 253: 1749 -1754 JID. 1990; 162: 1316 -1323 NEJM. 1997; 337: 970 -976 Percentage of Total Cases (1978 -81) (1985) (1995) 48 45 7 20 14 25 13 18 47 3 6 12 2 3 8 8 14 6 - -

INCIDENCE OF BACTERIAL MENINGITIS IN THE USA Per 100, 000 population % n n n S. pneumoniae 1. 1 47 N. meningitidis 0. 6 25 Group B Strep. 0. 3 12 L. monocytogenes 0. 2 8 H. influenzae 0. 2 7 NEJM 1997; 337: 970 -6
 n Increase in cases of MDR- S. pneumoniae. [Resulted in")
CHANGES IN EPIDEMIOLOGY (cont’d) n Increase in cases of MDR- S. pneumoniae. [Resulted in changes in empiric Rx] n Clusters of cases of meningococcal meningitis in adolescents & young adults. [Resulted in change in recommendation for meningococcal vaccination] n Cochlear implants and higher risk for bacterial meningitis. [Change in recommendation for Pneumococcal +/- Hib? ] n Decrease in pneumococcal invasive disease including meningitis after widespread use of of pediatric pneumococcal vaccine.

ETIOLOGY OF BACTERIAL MENINGITIS BY AGE <1 month Streptococcus agalactiae, Escherichia coli, Listeria monocytogenes, Klebsiella species 1 - 23 mos Streptococcus pneumoniae, Neisseria meningitidis, S. agalactiae, Haemophilus influenzae, E. coli 2 - 50 yrs N. meningitidis, S. pneumoniae >50 yrs S. pneumoniae, N. meningitidis, L. monocytogenes, aerobic gram-negative bacilli

ETIOLOGY OF BACTERIAL MENINGITIS BY PREDISPOSING CONDITION Immunocompromised state: S. pneumoniae, N. meningitidis, Listeria, aerobic GNR (including Ps. aeruginosa) Basilar skull fracture: S. pneumoniae, H. influenzae, betahemolytic strep group A. Head trauma or post-neurosurgery: S. aureus, S. epidermidis, aerobic GNR CSF shunt: S. epidermidis, S. aureus, aerobic GNR, Propionibacterium acnes

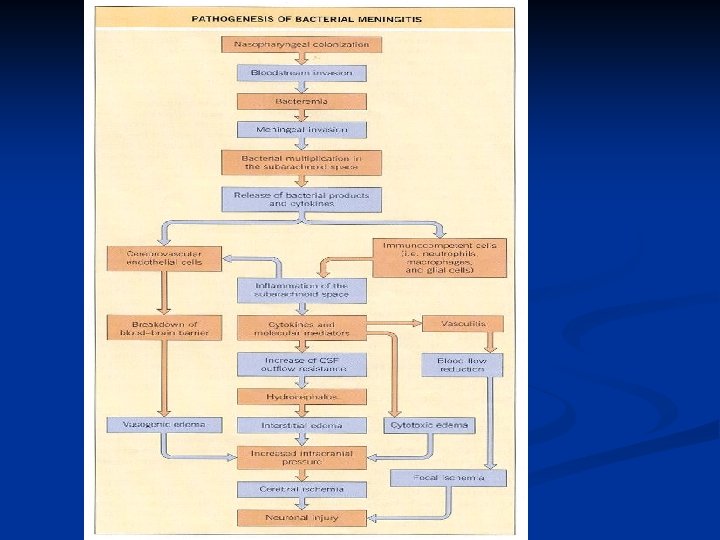
PATHOGENESIS OF BACTERIAL MENINGITIS 1. 2. Nasopharyngeal colonization Direct extension of bacteria. n n 3. Parameningeal foci (sinusitis, mastoiditis, or brain abscess) Across skull defects/fracture From remote foci of infection (e. g. , endocarditis, pneumonia, UTI…)

Brain with inflammatory exudate covering the cortical hemispheres in purulent meningitis. Cohen & Powderly: Infectious Diseases, 2 nd ed. , Copyright © 2004 Mosby
 FEVER >90")
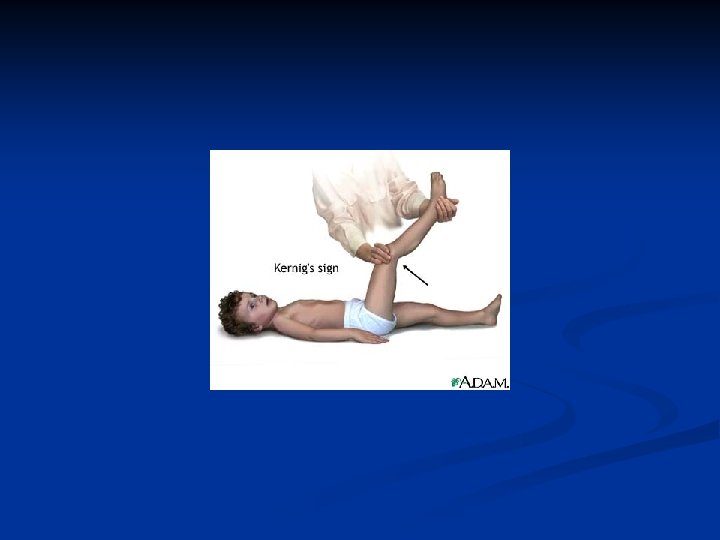
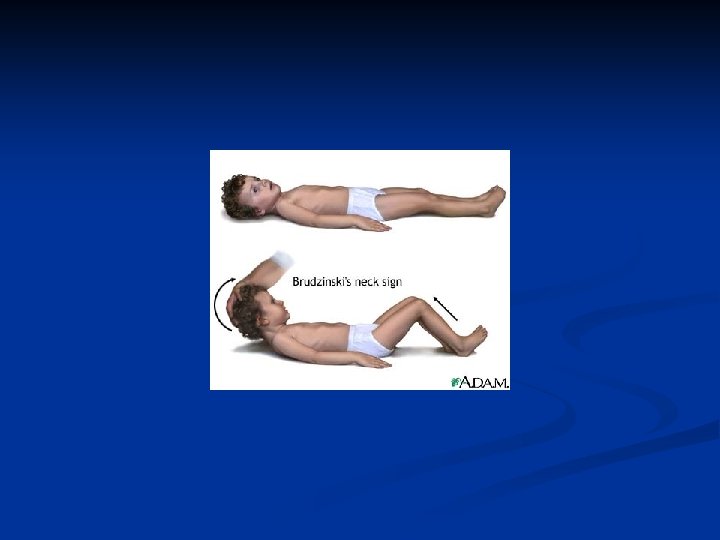
CLINICAL PRESENTATION Symptom or Sign n n n Relative Frequency (% ) FEVER >90 HEADACHE >90 NUCHAL RIGIDITY >85 ALTERED MENTAL STATUS 80 BRUDZINSKI SIGN 50 KERNIG SIGN 50 VOMITING ~35 SEIZURES 10 -30 FOCAL NEURO SIGNS 10 -30 PAPILLEDEMA <1 PHOTOPHOBIA SKIN RASH (e. g. , petechia/purpura in meningococcemia)


CONFIRMATION OF SUSPECTED BACTERIAL MENINGITIS n Lumbar puncture ASAP. n If LP has to be delayed for any reason, send blood culture and start empiric antibiotics. n Who should undergo CT prior to lumbar puncture?

Who should undergo CT prior to lumbar puncture? Criterion Comment Immunocompromised state HIV infection or AIDS, receiving immunosuppressive therapy, or after transplantation History of CNS disease Mass lesion, stroke, or focal infection New onset seizure Within 1 week of presentation; some authorities would not perform a lumbar puncture on patients with prolonged seizures or would delay lumbar puncture for 30 min in patients with short, convulsive seizures Papilledema Presence of venous pulsations suggests absence of increased intracranial pressure Abnormal level of consciousness Focal neurologic deficit . . . Including dilated nonreactive pupil, abnormalities of ocular motility, abnormal visual fields, gaze palsy, arm or leg drift

DIAGNOSIS - CSF Examination Typical CSF in Patients with Bacterial Meningitis n n n n n Opening pressure White blood cell count Neutrophils Protein Glucose CSF/serum glu ratio Gram stain Culture Bacterial antigen detection 200 -500 mm. H 2 O 1000 -5000/mm 3 >80% >100 mg/dl <40 mg/dl <0. 4 Positive in 50 -80% Positive in ~85% Positive in 50 -100%

CSF ANALYSIS PARAMETER OPENING PRESSURE WBC BACTERIAL 200 -500 mm H 20 VIRAL <250 mm H 20 1000 -5000 <1000 (mainly neutrophils) (mainly lymphocytes) GLUCOSE <40 mg/d. L >45 mg/d. L PROTEIN 100 -500 mg/d. L <200 mg/d. L

CSF PREDICTIVE OF BACTERIAL MENINGITIS WITH 99% ACCURACY, IF: n WBC count >2, 000 n Neutrophils >1180 n Protein >220 mg/dl n Glucose <34 mg/dl n Glu (CSF/serum): <0. 23 Spanos et al. JAMA 1989; 262(19): 2700 -7


What Specific CSF Diagnostic Tests Should Be Used to Determine the Bacterial Etiology of Meningitis? n n Gram Stain Latex Agglutination (the Practice Guideline Committee does not recommend routine use of this modality): n Does not appear to modify the decision to administer antimicrobial therapy n False-positive results have been reported n Some would recommend it for patients with a negative CSF Gram stain result and may be most useful for the patient who has been pretreated with antimicrobial therapy and whose Gram stain and CSF culture results are negative. Polymerase Chain Reaction (PCR) n Broad-based PCR may be useful for excluding the diagnosis of bacterial meningitis, with the potential for influencing decisions to initiate or discontinue antimicrobial therapy. n Although PCR techniques appear to be promising for the etiologic diagnosis of bacterial meningitis, further refinements of the available techniques may lead to their use in patients with bacterial meningitis for whom the CSF Gram stain result is negative. CID 2004; 39: 1267 -1284

What Laboratory Testing May Be Helpful in Distinguishing Bacterial from Viral Meningitis? n CSF LACTATE: n Not recommended in suspected community-acquired bacterial meningitis n May be helpful in the postoperative neurosurgical patient, n If CSF lactate concentrations are 4. 0 mmol/L, initiation of empirical antimicrobial therapy should be considered pending results of additional studies. n C-REACTIVE PROTEIN: n Normal CRP has a high negative predictive value in the diagnosis of bacterial meningitis. n Measurement of serum CRP concentration may be helpful in patients with CSF findings consistent with meningitis, but for whom the Gram stain is negative and you’re considering withholding antimicrobial therapy. n PROCALCITONIN: At present, because measurement of serum procalcitonin concentrations is not readily available in clinical laboratories, recommendations on its use cannot be made at this time. n PCR: Enterovirus-PCR (rapid, sensitivity 86 -100% specificity 92 -100%) CID. 2004; 39: 1267 -1284

IS CSF CULTURE ALWAYS POSITIVE IN BACTERIAL MENINGITIS?

BACTERIAL MENINGITIS CAN BE “CULTURE-NEGATIVE” n n n 10 -15% of bacterial meningitidis are culture-neg. Pre-LP use of even oral antibiotics may lower n Gram stain positivity by 20% & n Culture positivity by 30% In children (S. pneumo, H. flu, N. mening. ) in 90 -100% of pts within 24 -36 h of “appropriate” antibiotic Rx: n CSF became culture-negative n No sig change in cell count/chemistry. Ped. ID J. 1992 11 423 -32

ARE NEUTROPHILIC PLEOCYTOSIS & LOW CSF GLUCOSE UNIQUE FOR BACTERIAL MENINGITIS?

NEUTROPHILIC PLEOCYTOSIS & LOW CSF GLUCOSE May Not Always Mean Bacterial Meningitis n n n INFECTIONS: NON-INFECTIOUS: Viral meningitis (early n Chemical-meningitis phase only) (contrast…) Some parameningeal n Behcet syndrome foci/ cerebritis n Drug –induced ( NSAIDs, Leakage of brain Sulfa, INH, IVIG, OKT 3…) abscess into ventricle Amebic meningoencephalitis TB meningitis (rarely, & usu. only early)

BACTERIAL MENINGITIS MAY NOT ALWAYS HAVE NEUTROPHILIC PLEOCYTOSIS? n Partially Rx’d bacterial n n Listeria some GNR. . .

PRINCIPLES OF TREATMENT Suspected Bacterial meningitis Prompt initiation of treatment. n Bactericidal agents, with adequate CSF levels. n Empiric Rx (based on age and predisposing factors) n Specific Rx (based on Gram-stain or antigen). n Include steroids where indicated n

EMPIRIC THERAPY Common pathogens Antimicrobial therapy Patient’s Age <1 month Streptococcus agalactiae, Escherichia coli, Listeria monocytogenes, Klebsiella species Ampicillin plus cefotaxime or ampicillin plus an aminoglycoside 1 - 23 mos Streptococcus pneumoniae, Neisseria meningitidis, S. agalactiae, Haemophilus influenzae, E. coli Vancomycin plus a third-generation cephalosporin 2 - 50 yrs N. meningitidis, S. pneumoniae Vancomycin plus a third-generation cephalosporin >50 yrs S. pneumoniae, N. meningitidis L. monocytogenes, aerobic gram-negative bacilli Vancomycin plus ampicillin plus a third-generation cephalosporin

EMPIRIC THERAPY Predisposing Common pathogens factor Antimicrobial therapy Basilar skull fracture S. pneumoniae, H. influenzae, group A -hemolytic streptococci Vancomycin plus a thirdgeneration cephalosporin Penetrating trauma Staphylococcus aureus, coagulase- Vancomycin plus cefepime, negative staphylococci (especially vancomycin plus ceftazidime, or Staphylococcus epidermidis), vancomycin plus meropenem aerobic gram-negative bacilli (including Pseudomonas aeruginosa) Post- Aerobic gram-negative bacilli neurosurgery (including P. aeruginosa), S. aureus, coagulase-negative staphylococci (especially S. epidermidis) Vancomycin plus cefepime, vancomycin plus ceftazidime, or vancomycin plus meropenem CSF shunt Vancomycin plus cefepime, c vancomycin plus ceftazidime, c or vancomycin plus meropenemc Coagulase-negative staphylococci (especially S. epidermidis), S. aureus, aerobic gram-negative bacilli (including P. aeruginosa), Propionibacterium acnes

SPECIFIC-RX Microorganism Recommended Rx Alternative therapies Streptococcus pneumoniae Vancomycin plus a third-generation cephalosporina, b Meropenem (C-III), fluoroquinolonec (B-II) Neisseria meningitidis Third-generation cephalosporina Penicillin G, ampicillin, chloramphenicol, fluoroquinolone, aztreonam Listeria Ampicillind or penicillin Trimethoprim-sulfamethoxazole, monocytogenes Gd meropenem (B-III) Streptococcus agalactiae Ampicillind or penicillin Third-generation cephalosporina (B-III) Gd Haemophilus influenzae Third-generation cephalosporina (A-I) Chloramphenicol, cefepime (A-I), meropenem (A-I), fluoroquinolone Escherichia coli Third-generation cephalosporina (A-II) Cefepime, meropenem, aztreonam, fluoroquinolone, trimethoprimsulfamethoxazole . a Ceftriaxone or cefotaxime. b Some experts would add rifampin if dexamethasone is also given (B-III). c Gatifloxaxin or moxifloxacin. d Addition of an aminoglycoside should be considered.

PATHOGEN susceptibility Standard therapy Alternative therapies Streptococcus pneumoniae Penicillin MIC <0. 1 g/m. L Penicillin G or ampicillin Third-generation cephalosporin, chloramphenicol 0. 1 - 1. 0 g/m. L Third-generation cephalosporin Cefepime (B-II), meropenem > 2. 0 g/m. L Vancomycin plus a third -generation cephalosporin Fluoroquinolone Cefotaxime or Vancomycin plus a third ceftriaxone MIC 1. 0 -generation g/m. L cephalosporin Fluoroquinolone > Neisseria meningitidis Penicillin MIC <0. 1 g/m. L Penicillin G or ampicillin Third-generation cephalosporin, chloramphenicol

PATHOGEN STANDARD RX ALTERNATIVE RX Listeria monocytogenes Ampicillin or penicillin G Trimethoprim-sulfamethoxazole, meropenem Strep. agalactiae Ampicillin or penicillin G Third-generation cephalosporin E. coli and other Enterobacteriaceae Third-generation cephalosporin Aztreonam, fluoroquinolone, meropenem, trimethoprimsulfamethoxazole, ampicillin Pseudomonas aeruginosa Cefepime or ceftazidime Aztreonam ciprofloxacin, meropenem (consider plus aminoglycoside) Haemophilus influenzae B -Lactamase Ampicillin. negative Third-generation cephalosporin, cefepime, chloramphenicol, fluoroquinolone B -Lactamase positive Cefepime, chloramphenicol, fluoroquinolone Third-generation cephalosporin

PATHOGEN STANDARD RX ALTERNATIVE RX Methicillin susceptible Nafcillin or oxacillin Vancomycin, meropenem Methicillin resistant Vancomycin (consider Trimethoprim-sulfamethoxazole, adding rifampin) linezolid (consider adding rifampin) Staphylococcus epidermidis Vancomycin Staphylococcus aureus Linezolid Enterococcus species Ampicillin susceptible Ampicillin + gentamicin . . . Ampicillin resistant Vanc + gentamicin . . . Ampicillin and vancomycin resistant Linezolid . . .
 15 mg/kg (8) Ampicillin")
Amikacin In adults Total daily dose (dosing interval in hours) 15 mg/kg (8) Ampicillin Aztreonam Cefepime 12 g (4) 6 -8 g (6 -8) 6 g (8) Cefotaxime Ceftazidime Ceftriaxone Chloramphenicol Ciprofloxacin Gatifloxacin 8 -12 g(4 -6) 6 g (8) 4 g (12 -24) 4 -6 g (6) 800 -1200 mg (8 -12) 400 mg (24) Antimicrobial agent CID. 2004; 39: 1267 -1284
 Gentamicin 5 mg/kg (8) Meropenem")
Antimicrobial agent Total daily dose (dosing interval in hours) Gentamicin 5 mg/kg (8) Meropenem Moxifloxacin Nafcillin 6 g (8) 400 mg (24) 12 g (4) Oxacillin Penicillin G Rifampin Tobramycin 12 g (4) 24 m. U (4) 600 mg (24) 5 mg/kg (8) TMP-SMZ Vancomycin 10 -20 mg/kg (6 -12) 30 -45 mg/kg (8 -12) 9 CID 2004; 39: 1267 -1284
 Neisseria meningitidis 7 Haemophilus influenzae 7 Streptococcus pneumoniae 10")
Microorganism Duration of therapy (days) Neisseria meningitidis 7 Haemophilus influenzae 7 Streptococcus pneumoniae 10 -14 Streptococcus agalactiae 14 -21 Aerobic gram-negative bacilli 21 Listeria monocytogenes >21 Clinical Infectious Diseases 2004; 39: 1267 -1284

BACTERIAL MENINGITIS CASE FATALITY n n n S. pneumoniae L. monocytogenes Group B Strep. H. influenzae N. meningitidis (%) 21 15 7 6 3 NEJM 1997; 337: 970 -6 (based on 248 cases from 4 states, in 1995)

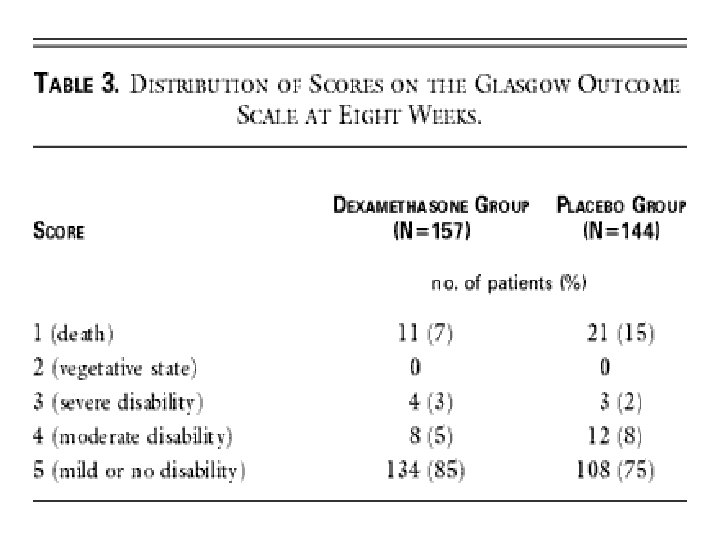
ROLE OF STEROIDS n Decrease subarachnoid space inflammatory response to abx-induced bacterial lysis n Significant reduction in deafness in pediatric H. influenzae & pneumococcal meningitis (JAMA 1997; 278: 925). n In adults, reasonable to use steroids: n for pts with evidence of cerebral edema. n for adult with pneumococcal meningitis (Nov 14, 2002 issue of NEJM) Give immediately before or with the 1 st dose of antibiotic. Dexamethasone dose: 0. 15 mg/kg q 6 x 2 -4 days

Dexamethasone in Adults with Bacterial Meningitis Jan de Gans, et. al. , for the European Dexamethasone in Adulthood Bacterial Meningitis Study Investigators NEJM 2002. 347: 1549 -1556. (Nov. 14, 2002)

Use of Adjunctive Dexamethasone Therapy in Adults with Bacterial Meningitis § In suspected or proven pneumococcal meningitis cases. • Dexamethasone should only be continued if the CSF Gram stain reveals gram-positive diplococci, or if blood or CSF cultures are positive for S. pneumoniae. • Adjunctive dexamethasone should not be given to adult patients who have already received antimicrobial therapy, because administration of dexamethasone in this circumstance is unlikely to improve patient outcome. • Addition of rifampin to the empirical combination of vancomycin plus a thirdgeneration cephalosporin may be reasonable pending culture results and in vitro susceptibility testing , in patients with suspected pneumococcal meningitis who receive adjunctive dexamethasone. § Some authorities would initiate dexamethasone in all adults because the etiology of meningitis is not always ascertained at initial evaluation, although the data are inadequate to recommend adjunctive dexamethasone to adults with meningitis caused by other bacterial pathogens

Use of Adjunctive Dexamethasone Therapy in Pediatric Patients with Bacterial Meningitis Infants and Children • Use in H. influenzae type b meningitis. • For pneumococcal meningitis, controversial. Neonates Insufficient data to make a recommendation on the use of adjunctive dexamethasone. CID 2004; 39: 1267 -1284

What Are the Indications for Repeated Lumbar Puncture in Patients with Bacterial Meningitis? • Not indicated routinely in patients with bacterial meningitis who have responded appropriately to antimicrobial therapy, • Repeated CSF analysis should be performed in: • Any patient who has not responded clinically after 48 h of appropriate antimicrobials This is especially true for the patient with pneumococcal meningitis caused by penicillin-or cephalosporin-resistant strains, especially for those who have also received adjunctive dexamethasone therapy. • Neonate with meningitis due to gram-negative bacilli should have repeated LPs • To document CSF sterilization, because the duration of antimicrobial therapy is determined, in part, by the result. • In patients with CSF shunt infections • The presence of a drainage catheter after shunt removal allows for monitoring of CSF parameters to ensure that the infection is responding to appropriate antimicrobial therapy and drainage). CID 2004; 39: 1267 -1284

PREVENTION OF BACTERIA MENINGITIS n Isolation of index patient n n Droplet precautions For 24 hrs after 1 st dose of appropriate abx) Post-exposure prophylaxis n Vaccination n

POST-EXPOSURE PROPHYLAXIS n Candidates: n Household members n Day care center contacts n Direct exposure to pt’s oral secretion ( as in kissing, mouth-to-mouth , intubation/ET tube management) n Index patient (if not treated w 3 rd gen cephalosporins) n Regimen: n Meningococcus: Rifampin, ciprofloxacin, or ceftriaxone n Hempohilus influenzae serotype b: Rifampin.

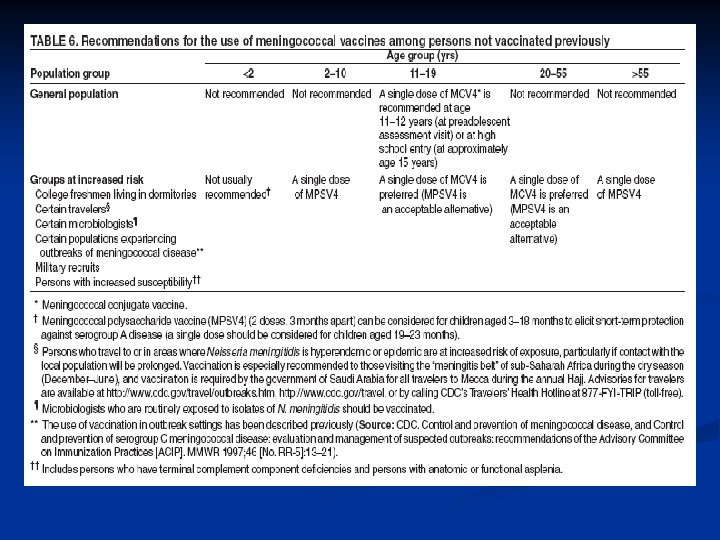
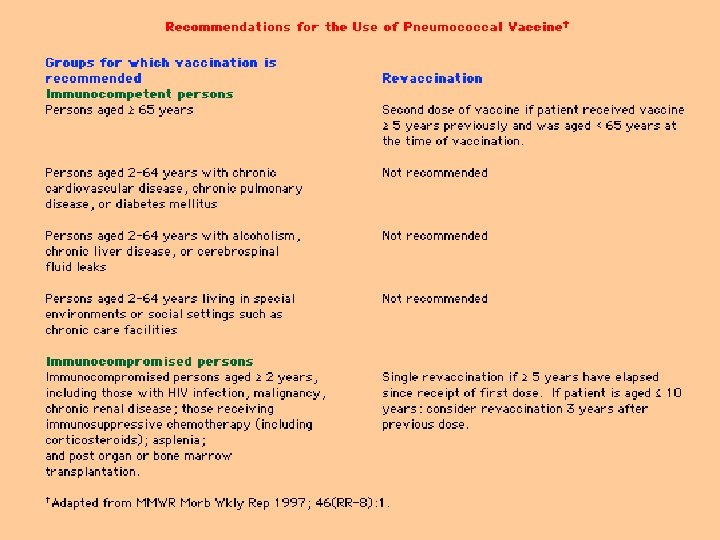
Vaccination n Hib vaccine. n n Pneumococcal vaccine. n n n Has had major impact in incidence of pediatric Hib meningitis For chronically ill and elderly, & now universal use in children. PCV-7. Use of PCV-7 for children has been an effective means of preventing disease in older adults (JAMA. Vol. 294 No. 16, October 26, 2005 ) Meningococcal vaccine n n n Effective vs serotype A, C, Y, W 135 Major reduction of disease in military recruits Recommended for travelers to endemic areas. Offered to college students, specially those residing in dormitory A new quadrivalent vaccine (Menactra) was recently approved.
 • Children aged 11")
Who Should Be Vaccinated with the NEW MENINGOCOCCAL VACCINE (Menactra) • Children aged 11 -12 years • Previously unvaccinated adolescents before entering high school or at age 15 (whichever comes first) • All first-year college students living in dormitories • Other high-risk groups, such as those with underlying medical conditions or travelers to areas with high rates of meningococcal disease, such as Africa and India. • Other adolescents who choose to get the vaccine to reduce their risk "As the vaccine supply increases, CDC hopes, within three years, to recommend routine vaccination [for] all adolescents beginning at 11 years of age, " per CDC's news release

FDA and CDC Issue Alert on Menactra Meningococcal Vaccine and Guillain Barre Syndrome • FDA and CDC alerted consumers and health care providers to five reports of Guillain Barre Syndrome (GBS) following administration of Meningococcal Conjugate Vaccine (trade name Menactra). • It is not known yet whether these cases were caused by the vaccine or are coincidental. • Prelicensure studies conducted by Sanofi Pasteur of more than 7000 recipients of Menactra showed no GBS cases. • CDC conducted a rapid study using available health care organization databases and found that no cases of GBS have been reported to date among 110, 000 Menactra recipients. September 30, 2005

CRITERIA FOR OUTPATIENT ANTIMICROBIAL THERAPY IN PATIENTS WITH BACTERIAL MENINGITIS • Inpatient antimicrobial therapy for > 6 days • Absence of fever for at least 24 - 48 h prior to initiation of outpatient therapy • No significant neurologic dysfunction, focal findings, or seizure activity • Clinical stability or improving condition • Ability to take fluids by mouth • Access to home health nursing for antimicrobial administration • Reliable intravenous line and infusion device (if needed) • Daily availability of a physician • Established plan for physician visits, nurse visits, laboratory monitoring, and emergencies • Patient and/or family compliance with the program • Safe environment with access to a telephone, utilities, food, and refrigerator CID 2004; 39: 1267 -1284

REVIEW n n n n Most common cause overall…. CT? Duration of Rx… Steroids for… Most deadly… Isolation for…. How long? Chemoprophylaxis n n For which pathogens? Which contacts? What Regimen? Vaccination?

MANAGEMENT




DO YOU WANT MORE SLIDES ON BACTERIAL MENINGITIS? ?

SHUNT INFECTION § Removal of all components of the infected shunt, external drainage, +abx COAG-NEGATIVE STAPH. : 1. If normal CSF findings, and a negative CSF culture results after externalization, the patient can be reshunted on the 3 rd day after removal. 2. If CSF abnormalities are present and a coagulase-negative staphylococcus is isolated, 7 days of antimicrobial therapy are recommended prior to reshunting as long as additional CSF culture results are negative and the ventricular protein concentration is appropriate (<200 mg/d. L); 3. If additional culture results are positive, abx are continued until CSF culture results remain negative for 10 consecutive days before a new CSF shunt is placed. STAPH. AUREUS : 10 days of negative culture results are recommended prior to reshunting. GRAM-NEGATIVE BACILLI: 10 -14 day course of antimicrobial therapy should be used, although longer durations may be needed depending on the clinical response. [Some experts also suggest that consideration be given to a 3 -day period off antimicrobial therapy to verify clearing of the infection prior to shunt reimplantation; although this approach is optional, it may not be necessary for all patients].

Neisseria Meningitidis n 5 -15% asymptomatic nasopharyngeal colonization. n Transmission by air-droplets, kissing, sharing saliva… n Most common cause of meningitis in children and young adults , with overall mortality rate of 3 - 13%. n Causes epidemics in the “meningitis belt. ” n Predisposing Factors : n Deficiencies in the terminal complement components (C 5 -C 9) n Splenectomy n Crowding (military recruits, college dormitory, Hajj…). Tarvel. n College freshmen in dormitory>>dormitory >> freshman>>college students overall.

Rates of meningococcal disease, by risk group --United States, Sept. 1998 --Aug. 1999 Risk group Children aged 2 -5 years Rate per 100, 000 1. 7 Persons aged 18 -23 years 1. 4 Non-college students aged 18 -23 years 1. 5 College students 0. 6 Undergraduates 0. 7 Freshmen 1. 8 Dormitory residents 2. 2 Freshmen living in dormitories MMWR 2000, 49(RR-7)1 -20 4. 6

 n Resistance to penicillin still very")
Meningococcal Meningitis Penicillin (or 3 rd gen cephalosporin) n Resistance to penicillin still very rare n If penicillin used for Rx, eradication of pharyngeal colonization of index case advisable n Duration of Rx, 7 days n Chemoprophylaxis for close contacts n Droplet isolation (for 24 h after 1 st dose of abx) n

Streptococcus Pneumoniae n Most common cause of bacterial meningitis in the US, with mortality rate of 19 to 26%. n n Often from contiguous or distant foci of infection (e. g. , pneumonia, otitis media, mastoiditis, sinusitis, endocarditis, or after head trauma w CSF leak). Predisposing factors: n Anatomic or functional asplenia, multiple myeloma, hypogammaglobulinemia, alcoholism, malnutrition, chronic liver or renal disease, malignancy, and diabetes mellitus.

Pneumococcal Meningitis n n n n Before MICs: Vancomycin + 3 rd gen cephalosporin If PSSP: Penicillin (or 3 rd gen cephalosporin) alone If PRSP(CTX-S): 3 rd gen cephalosporin If PRSP&CTX-R: Vancomycin +3 rd gen cephalosp Steroids in children & adults If on vanc, and steroids have to be used, add rifampin? For PRSP: re-LP in few days for response. Duration of Rx 10 -14 days

Haemophilus Influenzae n n n Meningitis usually seen in children <6 years (peak 612 mo). Capsular type b causes >90% of invasive disease. Meningitis in above 6 yrs usually associated with: sinusitis, otitis, pneumonia, sickle cell disease, splenectomy, DM, alcoholism, immuno-deficiency, or head trauma w csf leak. Causes 7% of meningitis cases in US Mortality 3 -6%.

H. influenzae meningitis Ceftriaxone or cefotaxime n Steroids in chldren n Duration of Rx: 5 -7 days n Chemoprophylaxis of close contacts. n Droplet precaution (in pediatric cases, x 24 h of abx) n

Listeria monocytogenes n May be isolated from dust, soil, water, sewage, and decaying vegetable matter. Usually foodborne infections (contaminated cole slaw, raw vegetables, milk, cheese. . . ) n Causes 8% of cases of bacterial meningitis in the US, mortality rate of 15 -29%. (Seizures, focal signs, rhomboencephalitis common) n Meningitis most common in neonates/elderly, alcoholics, malignancy, corticosteroid Rx. n Other predisposing factors: DM, liver disease, chronic renal disease, collagen-vascular diseases, & conditions with Fe overload.

Streptococcus agalactiae n Asymptomatic vaginal or rectal colonization in 15 to 35% of pregnant women. n Most common cause of meningitis in newborns n Mostly vertical transmission (but some horizontal transmission from the hands of nursery personnel) n Can also cause meningitis in ADULTS. Risk factors in adults include: age>60 years, diabetes mellitus, pregnancy/the postpartum state, cardiac disease, collagen-vascular diseases, malignancy, alcoholism, hepatic failure, renal failure, previous stroke, neurogenic bladder, decubitus ulcers, and corticosteroid therapy.
 meningitis is mainly postneurosurgical, CSF shunts, or")
Staphylococci n Staphylococcus aureus (&/or coag-neg Staph) meningitis is mainly postneurosurgical, CSF shunts, or post-trauma. n Community-acquired S. aureus meningitis can be seen in patients with sinusitis, endocarditis, osteomyelitis, and pneumonia. n Other underlying conditions include diabetes mellitus, alcoholism, hemodialysis, injection drug use, and malignancies

Aerobic Gram-Negative Bacilli n Increasingly important cause of bacterial meningitis (e. g. , Klebsiella spp. , E. coli, Serratia marcescens, Pseudomonas aeruginosa, Salmonella spp. ) n Usually after head trauma or neurosurgery. n May be seen in neonates, the elderly, immunosuppressed patients, and pts with gram-negative sepsis. n Seen w the hyperinfection syndrome of disseminated strongyloidiasis
 + an aminoglycoside n Re-LP for")
Garm negative meningitis Ceftazidime (or Cefepime or meropenem) + an aminoglycoside n Re-LP for proof of response, in 2 -4 days? n Duration of Rx: 21 days n


 Deafness (5 -10%)")
BACTERIAL MENINGITIS COMPLICATIONS n n n Death ( Pneumococcal> Listeria> Meningococcal) Deafness (5 -10%) Mental retardation (4. 2%) Seizures( 4. 2%) Paresis/spasticity (3. 5%) Poorest prognosis: >60, seizure `24 h, obtunded/coma

COMPLICATIONS OF BACTERIAL MENINGITIS Immediate n Coma Loss of airway reflexes Seizures Cerebral edema Vasomotor collapse Disseminated intravascular coagulation (DIC) Respiratory arrest Dehydration Pericardial effusion Death Delayed n Seizure disorder Focal paralysis Subdural effusion Hydrocephalus Intellectual deficits Sensorineural hearing loss Ataxia Blindness Bilateral adrenal hemorrhage Death

COMPLICATIONS of BACTERIAL MENINGITIS Cerebral infarction from occlusion of inflammed vessels (focal neurologic signs, seizures, AMS. . ) n Brain edema from disturbance of cerebrovascular autoregulation, leakage of fluid from damaged vessels, cytotoxic edema from damaged barin cells, or dural sinus thrombosis which impede blood drainage from brain) n Obstruction of flow of CSF (hydrocephalus) n
. Daily intraventricular dose,")
Recommended dosages of antimicrobial agents administered by the intraventricular route (A-III). Daily intraventricular dose, mg Antimicrobial agent Vancomycin 5 20 Gentamicin 1 8 Tobramycin 5 20 Amikacin 5 50 Polymyxin B 5 Colistin 10 Quinupristin/dalfopristin 2 5 Teicoplanin 5 40 NOTE. There are no specific data that define the exact dose of an antimicrobial agent that should be administered by the intraventricular route. a Most studies have used a 10 -mg or 20 -mg dose. b Usual daily dose is 1 2 mg for infants and children and 4 8 mg for adults. c The usual daily intraventricular dose is 30 mg. d Dosage in children is 2 mg daily. e

RECURRENT MENINGITIS Bacterial: n Anatomic defect/CSF leak n Parameningeal infection n Immunologic (Ig def, asplenia, complement def. . . ) Chemical: Endogenous: craniopharyngioma, epidermid cyst. Drugs, Behcet, SLE, Mollaret. . .
: 1727")
Hasbun et al. NEJM 2001: 345 (24): 1727
: 1727 -33")
Hasbun et al. NEJM 2001: 345 (24): 1727 -33

What Laboratory Testing May Be Helpful in Distinguishing Bacterial from Viral Meningitis? CSF Lactate • Not recommended for patients with suspected community-acquired bacterial meningitis • However, measurement of CSF lactate concentrations was found to be superior to use of the ratio of CSF to blood glucose for the diagnosis of bacterial meningitis in postoperative neurosurgical patients, in which a CSF concentration of 4. 0 mmol/ L was used as a cutoff value for the diagnosis… Therefore, in the postoperative neurosurgical patient, initiation of empirical antimicrobial therapy should be considered if CSF lactate concentrations are > 4. 0 mmol/L, pending results of additional studies. C-reactive Protein Measurement of serum CRP concentration may be helpful in patients with CSF findings consistent with meningitis, but for whom the Gram stain result is negative and the physician is considering withholding antimicrobial therapy, on the basis of the data showing that a normal CRP has a high negative predictive value in the diagnosis of bacterial meningitis. Procalcitonin At present, because measurement of serum procalcitonin concentrations is not readily available in clinical laboratories, recommendations on its use cannot be made at this time (C-II). Polymerase Chain Reaction In patients who present with acute meningitis, an important diagnostic consideration is whether the patient has enteroviral meningitis. Rapid detection of enteroviruses by PCR has emerged as a valuable technique that may be helpful in establishing the diagnosis of enteroviral meningitis.

IMPACT OF PCV-7 Annual Incidence of Invasive Pneumococcal Disease by Age Group for Adults >50 Years—Active Bacterial Core Surveillance, 1998 -2003 Percentage reductions from 1998 -1999 to 2002 -2003: for persons aged 85 years, – 28% (95% confidence interval [CI], – 36% to – 19%); 75 -84 years, – 35% (95% CI, – 41% to – 28%); 65 -74 years, – 29% (95% CI, – 36% to – 21%); and 50 -64 years, – 17% (95% CI, – 24% to – 11%). Percentage reductions were significant (P<. 001) in each age group. PCV-7 indicates 7 -valent pneumococcal conjugate vaccine. JAMA. Vol. 294 No. 16, October 26, 2005

JAMA. Vol. 294 No. 16, October 26, 2005

JAMA. Vol. 294 No. 16, October 26, 2005
256b802d97214b811cf9999207b2a1e1.ppt